
Abstract
The sonographic findings and corresponding pathology reports of 83 premenopausal and 55 postmenopausal women were retrospectively reviewed to evaluate the significance of color Doppler imaging in the evaluation of the endometrium. Premenopausal women had flow noted in the single malignancy case and in 16 of 21 (76%) polyps, with 7 polyps (33%) presenting as a vascular pedicle. In postmenopausal women, flow was seen in 3 of 5 (60%) malignancies and 5 of 9 (56%) polyps, with 2 polyps (22%) presenting as a vascular pedicle. Postmenopausal women with thin endometria had flow in 1 of 2 (50%) polyps, while those with thicker endometria had flow in 4 of 7 (56%) polyps and 3 of 5 (60%) malignancies. The data showed that color Doppler imaging was useful in detecting vascular pedicles in endometrial polyps, but it was not otherwise helpful as an independent predictor of malignancy.
Introduction
Endometrial abnormalities are common diagnostic challenges facing the sonographer and interpreting physician. In the US, carcinoma of the uterine corpus is the most common malignancy of the female reproductive system, with 49 560 new cases and 8190 deaths estimated for 2013. 1 Endometrial carcinoma is by far the most common variety, while malignant tumors of the myometrium are quite rare. Women with endometrial cancer typically present with abnormal uterine bleeding, which can also be caused by benign uterine conditions such as hormonal imbalance, endometrial atrophy, inflammation, endometrial hyperplasia, and/or polyps. 2 Imaging plays an important role in detecting abnormalities in these women and in identifying those who may require further evaluation with endometrial biopsy. In the past two decades alone, mortality due to endometrial cancer has decreased by 25% due to early detection, diagnosis, and treatment. 3
Endovaginal ultrasonography (EVU) is the imaging modality of choice to initially evaluate women with post- or perimenopausal and intermenstrual uterine bleeding. In postmenopausal women with abnormal bleeding, endometrial cancer may be reliably excluded when the endometrial thickness is less than 4 mm, with a sensitivity rate of 94.8% and specificity of 46.7%.4,5 In premenopausal women with abnormal uterine bleeding, endometrial thickness can be difficult to evaluate because of its variability being affected by exogenous or endogenous sex hormones.
Given the known role of angiogenesis in tumor growth, the evaluation of tissue vascularization by Doppler has been thought to be useful in the prediction of malignant endometrial changes, since malignancy has been associated with increased blood flow.6,7 A study conducted by Timmerman et al 8 showed that the presence of a vascular pedicle is highly suggestive for the presence of an endometrial polyp in women with abnormal vaginal bleeding. Various studies using spectral Doppler indices, power Doppler threshold values, and color Doppler features have also considered the characterization of endometrial lesions; however, all of these demonstrated overlap between benign and malignant pathologies.9 -12
Although studies have evaluated endometrial thickness and Doppler patterns in pre- and postmenopausal patients separately, to the best of our knowledge, there are no studies that correlate endovaginal color Doppler (EVCD) findings in a combined pre- and postmenopausal population. The purpose of this study is to report our findings regarding the utility of color Doppler imaging in the evaluation of the endometrium.
Materials and Methods
The Human Subjects Review Committee of our institution approved this study. All information was obtained by retrospective chart review of the electronic medical records. A list of women who underwent endometrial pathological studies for a three-year period was obtained from our Pathology department. From this list, all patients who underwent EVCD evaluation prior to biopsy were selected for analysis. All consecutive adult patients available to us were included, both pre- and postmenopausal patients, who were of consenting age.
The study population included 138 women with an age range from 25 to 86 years (mean, 49 years). Of the 138 cases, 83 were premenopausal and 55 were postmenopausal, as determined by either the referring gynecologic examination and/or the dictated sonogram report. Natural menopause was defined and established as one year of absence of menstruation in women who were older than 45 years. Women receiving hormone replacement therapy (HRT), including tamoxifen and Provera, with irregular bleeding were included in the study. Eleven postmenopausal women were taking HRT, and 7 premenopausal women were taking oral contraceptives.
Sonographic examinations were performed with Sequoia 512 scanners (Siemens Medical Solutions, Mountain View, CA). Curved or vector transducers were used for transabdominal scanning with frequencies of 3 to 8 MHz. Endovaginal scanning was performed using probe frequencies of 5 to 8 MHz. Every study included both transabdominal and endovaginal sonography with color Doppler imaging performed in all cases. Trained sonographers with 2 years to 25 years of sonographic experience performed the studies. As per study protocol, endometrial thickness was measured in the longitudinal plane with conventional technique. Color Doppler imaging was performed with optimized parameters to assess vascularization of the endometrium in each patient. Power level, threshold, persistence, and wall filter were adjusted to maximize blood flow detection. Initial image review and dictated reports were completed by medical center faculty. Each case was reexamined by one of the authors (EOG) to assure appropriate inclusion in the study and verify the sonographic findings.
Specific sonographic findings including endometrial thickness, uterine size, and the presence/absence of endometrial blood flow were recorded at the time of the initial sonographic examination. Because endometrial thickness in premenopausal women can vary significantly in response to exogenous or endogenous sex hormones, this was not reported. Each postmenopausal subject was placed into a category of either a thin or thick endometrium based on a bi-layer measurement of less than or equal to 4 mm. In those patients identified as taking hormone replacement therapy, a thickness cutoff of 8 mm was used.13-15 Postmenopausal women were further divided into distinct categories based on those with detectable endometrial flow and those without.
A vascular pedicle was identified by linear color Doppler flow penetrating the endometrium from the myometrium. In all subjects identified with a pathologic diagnosis of a polyp, both gray-scale and color Doppler findings were recorded for each subgroup, specifically to evaluate for polyps detected solely by gray-scale, polyps detected solely by a single vascular pedicle, or polyps detected by combined gray-scale and a vascular pedicle.
These results were then compared to pathological specimens obtained by either hysterectomy, hysteroscopy, and/or endometrial histology on dilatation and curettage, all within one year of the sonographic examination. The average time from EVCD to tissue collection for histological analysis was 74 days, ranging from the same day to 335 days. Women with a time lapse of greater than 365 days between sonographic examination and tissue collection were excluded from the study.
To facilitate data analysis, pathology results were sorted into four distinct categories depending on patient category types (premenopausal vs. postmenopausal): benign, polyp, malignant, or inconclusive. Cases with benign findings included proliferative, secretory, dys-synchronous, and atrophic endometrium, as well as endometrium with inflammation and ciliated metaplasia. The polyp category included only benign polyps. Histological findings of malignant pathologies included endometrial cancer and complex endometrial hyperplasia with atypical cells. The inconclusive category included those specimens too scant for pathological diagnosis. Because benign and malignant endometria do not reliably demonstrate discrete gray-scale features, gray-scale findings were not reported.
Results
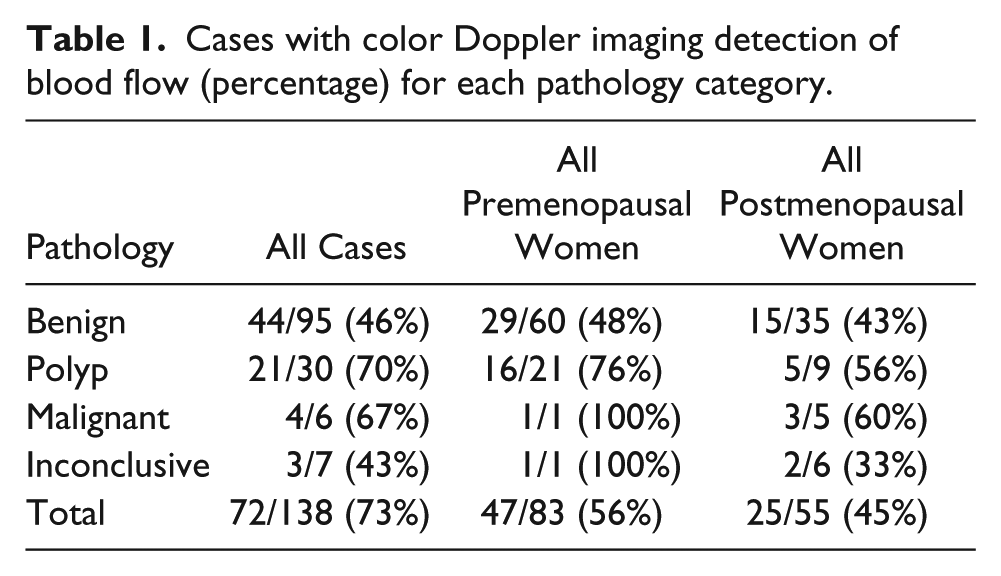
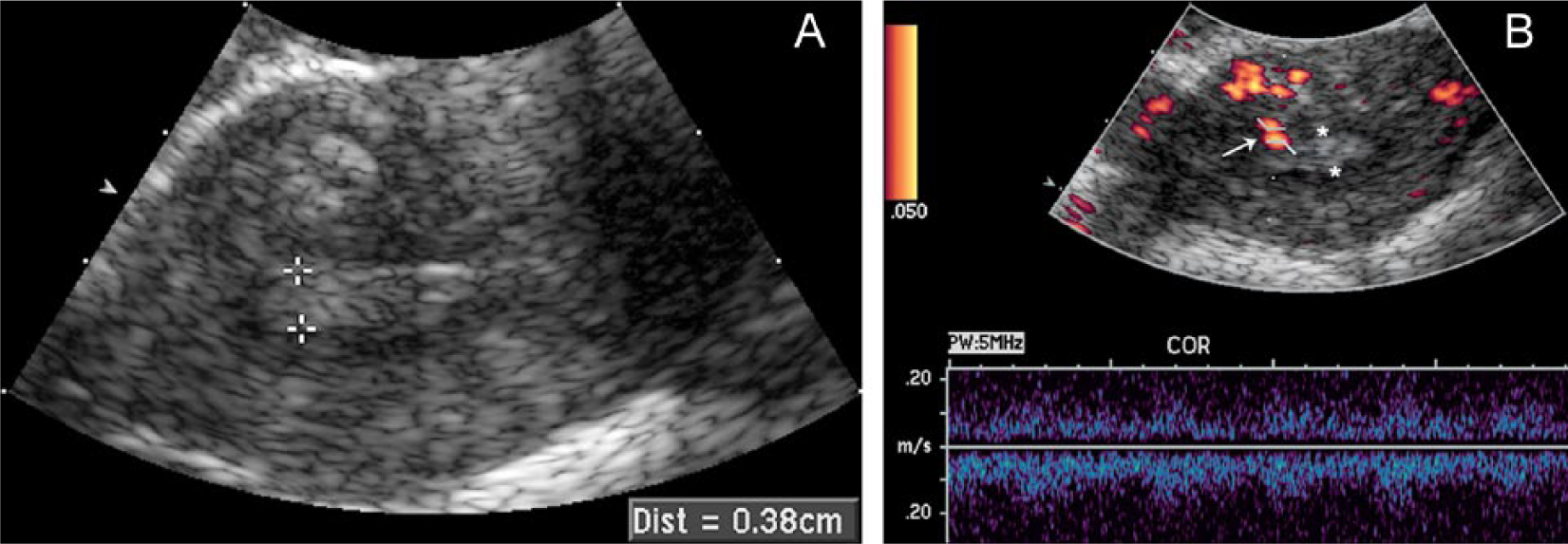
The pathology records of the 138 subjects showed 95 benign cases, 30 polyps, 6 malignancies, and 7 inconclusive cases. Blood flow percentages for each pathology category in all women are reported in Table 1. In premenopausal patients, 47 of 83 (56%) had color Doppler imaging detection of blood flow. Pathology for premenopausal patients showed 60 benign specimens, 29 with blood flow detected (48%); 21 polyps, 16 with blood flow detected (76%); 1 malignancy with blood flow detected (100%); and 1 inconclusive case with blood flow detected (100%). Figures 1A and 1B demonstrate the sonographic findings in a premenopausal patient with subsequent pathological diagnosis of polyp. Figures 2A and 2B demonstrate sonographic findings in a premenopausal woman with subsequent diagnosis of adenocarcinoma.
Cases with color Doppler imaging detection of blood flow (percentage) for each pathology category.
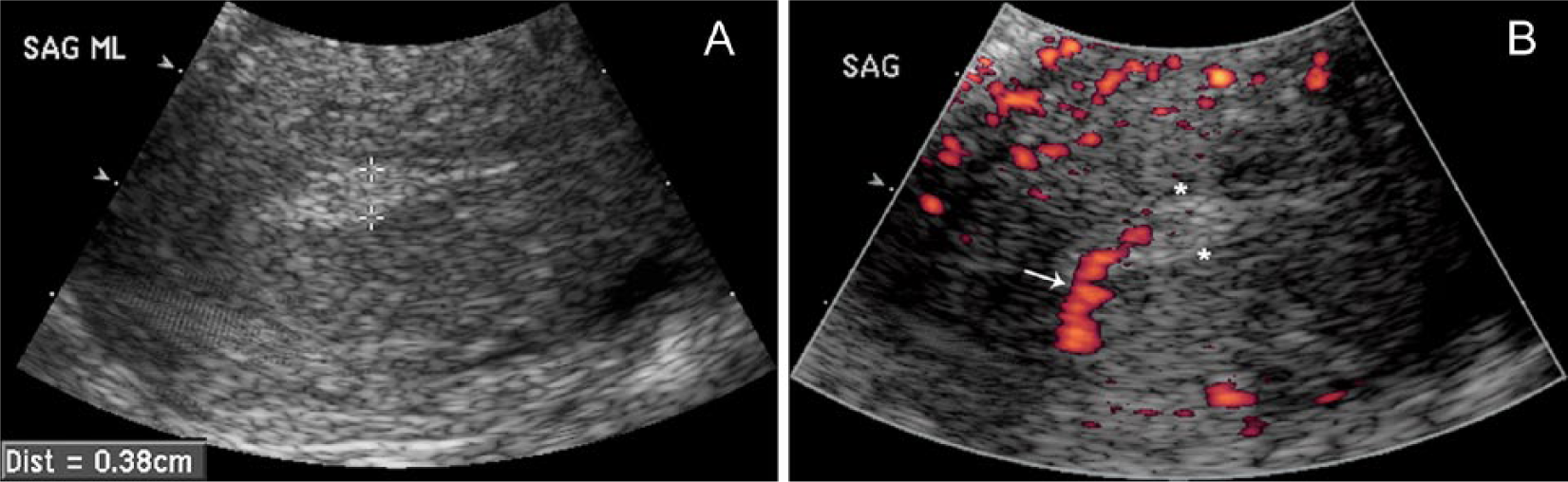
Twenty-five-year-old patient with last menstrual period one week before sonography and a clinical history of vaginal spotting for four months. Endometrial pathology showed an ulcerated benign polyp.
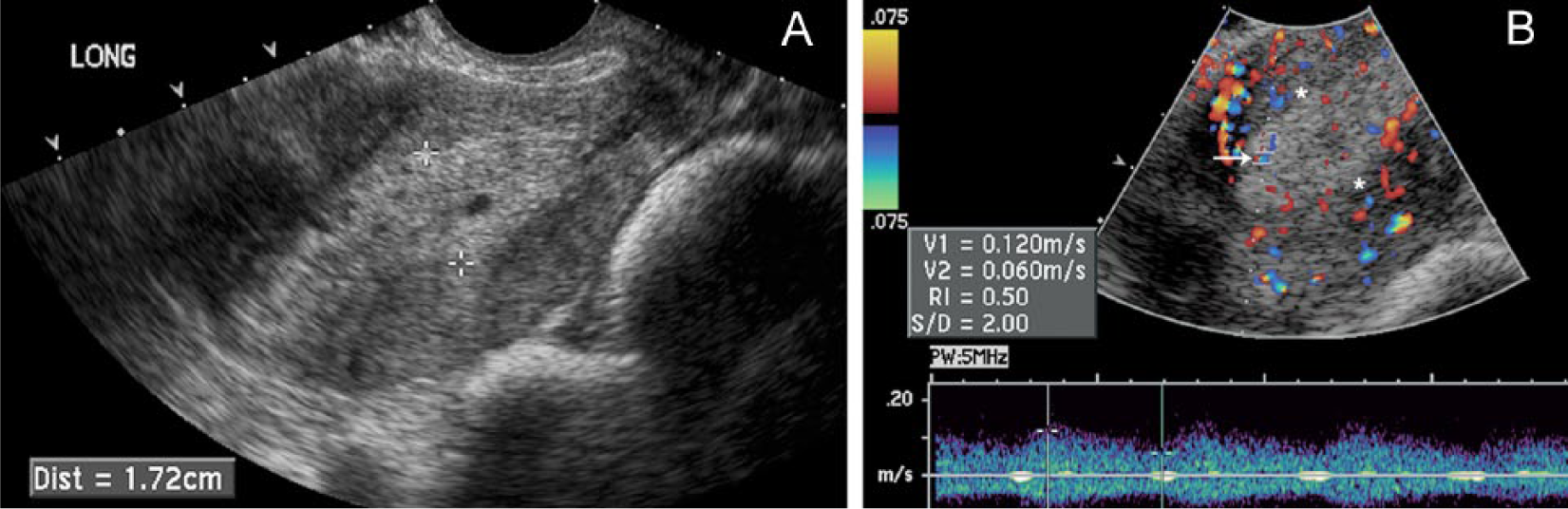
Forty-three-year-old premenopausal patient with no history of hormonal medication and irregular menses for two years. Endometrial pathology showed adenocarcinoma.
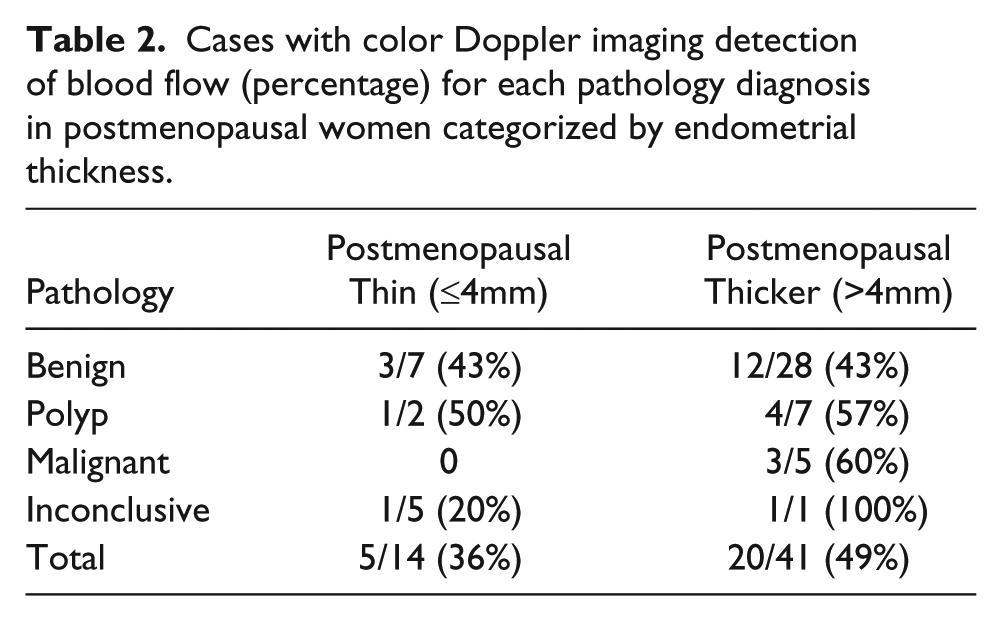
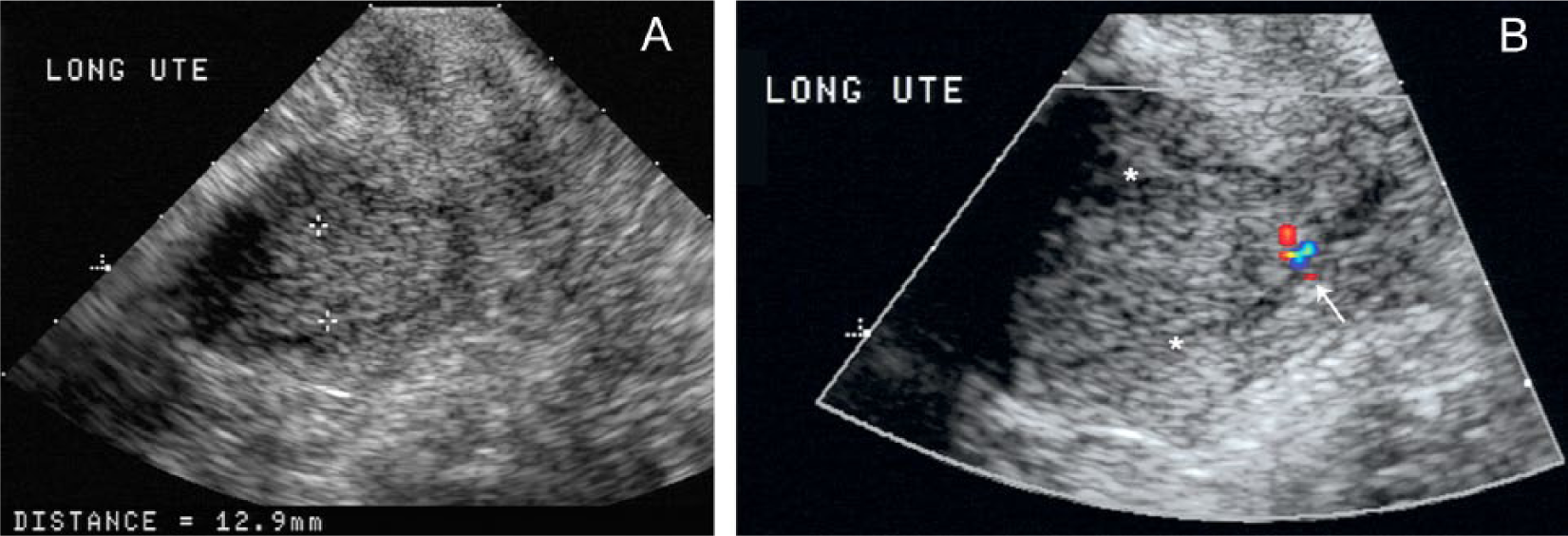
Using the specified endometrial thickness cutoff parameter, 14 postmenopausal women were identified as having a thin endometrium with color Doppler imaging detection of blood flow in 5 patients (36%). Pathology results in this subgroup showed seven benign specimens, three with blood flow detected (43%); two polyps, one with blood flow detected (50%); zero malignancies; and five inconclusive cases, one with blood flow detected (20%) (Table 2). Figures 3A and 3B demonstrate the sonographic findings of a postmenopausal woman with a thin endometrium and the subsequent pathologic diagnosis of a benign polyp.
Cases with color Doppler imaging detection of blood flow (percentage) for each pathology diagnosis in postmenopausal women categorized by endometrial thickness.
Fifty-five-year-old postmenopausal patient with history of uterine bleeding. Endometrial pathology showed a benign polyp.
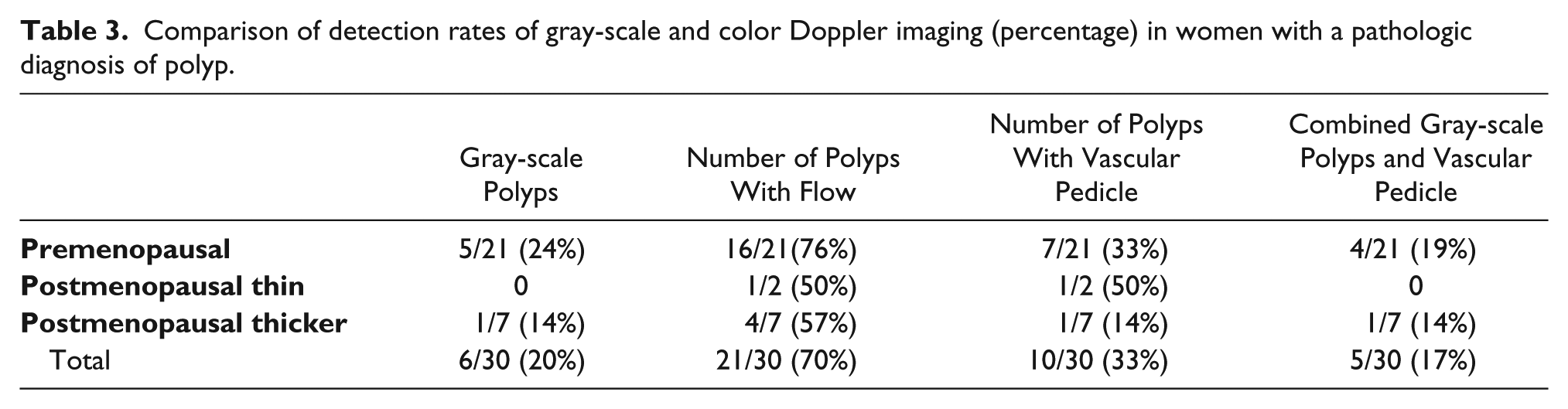
In the remaining 41 postmenopausal women with thicker endometria, color Doppler imaging detected blood flow in 20 patients (49%). Pathology for these patients showed 28 benign specimens, 12 with blood flow detected (43%); 7 polyps, 4 with blood flow detected (57%); all 5 malignancies, 3 with blood flow detected (60%); and 1 inconclusive case with blood flow detected (100%) (Table 2). Figures 4A and 4B demonstrate the sonographic findings in a postmenopausal woman with a thicker than expected endometrium and subsequent diagnosis of adenocarcinoma. The gray-scale sonogram and color Doppler findings in all women with pathologic diagnosis of polyps are reported in Table 3.
Sixty-three-year-old postmenopausal patient with no history of hormonal medication and uterine bleeding. Endometrial pathology showed carcinoma.
Comparison of detection rates of gray-scale and color Doppler imaging (percentage) in women with a pathologic diagnosis of polyp.
Discussion
The present study reports the EVCD results in detecting endometrial flow in women of all ages with variable endometrial thickness. While sonographic measurements of endometrial thickness have shown to be useful for detecting endometrial disease, gray-scale endovaginal sonography has not been demonstrated to be as accurate in the detection of endometrial polyps. Because second-stage tests to diagnose endometrial lesions, such as saline contrast sonohysterography and office hysteroscopy, are invasive, EVCD has been suggested as a useful adjunct to demonstrate abnormal vascular flow patterns related to polyps and/or endometrial cancer.8,16,17
In this study both polyp and malignancy categories demonstrated higher percentages of detectable flow than what was found with benign tissue diagnosis. This may be due to the fact that benign cases with detectable flow could be secondary to dysregulation of endometrial blood flow, known to be associated with several benign menstrual disorders including dysmenorrhea, menorrhagia, intermenstrual bleeding, and endometriosis.18,19 The single premenopausal malignant case had both a prominent endometrium (22 mm) and positive color Doppler flow. Endometrial malignancy in premenopausal women previously has been positively correlated with a family history of endometrial cancer, younger age at menarche, null parity, infertility, obesity, radiation exposure, and long-term use of unopposed estrogens for hormone replacement therapy.20,21
When considering postmenopausal cases, endometrial thickness (using a cutoff of 4 mm) was useful in detecting all five endometrial malignancies, while color Doppler imaging only detected flow in three (60%) of these cases. These findings are consistent with prior studies indicating endometrial flow characteristics are not sufficiently sensitive, specific, or predictive to be used alone as sole criteria for prediction of malignancy.6,22 Kurjak et al 23 demonstrated tumoral blood flow to be present in 91% of endometrial carcinomas, a much higher rate than in our experience, possibly related to sample size differences, differences in the criteria or techniques used, as well as their utilization of a gold standard of a hysterectomy specimen being the only specimen sampled in every case.
In postmenopausal women identified as having a thin endometrium, no malignancies were found in any cases. This is consistent with findings reported by Gull and colleagues 24 who followed 339 postmenopausal women for up to 10 years and also found no cases of malignancy when an endometrial thickness cutoff of 4 mm was used. A meta-analysis by Gupta et al 25 suggested that a cutoff of 5 mm is optimal for ruling out endometrial pathology. The current study provided findings to support the idea that patients experiencing postmenopausal bleeding and having a sonographic endometrium measurement of less than or equal to 4 mm safely predicts a benign diagnosis.24,26 Rare false-negative sonographic studies in postmenopausal women have been reported and may be caused by disease confined to the myometrium from foci of adenomyosis or the result of a suboptimal performance of sonographic examination. 27
In postmenopausal women with thicker endometria, detectable flow in malignant cases may in part be related to increased endometrial blood vessels, which can also be seen in cases of complex hyperplasia.23,28,29 Prior studies indicate hormone replacement therapy also affects endometrial flow, and postmenopausal patients who receive tamoxifen may show an increased occurrence of endometrial polyps, hyperplasia, and endometrial carcinoma.30,31 It has also been demonstrated that malignant degeneration of endometrial polyps can occur in postmenopausal women. There is a reported minimal increased risk of endometrial cancer in women with endometrial polyps.29,32 In this study, no findings of polyps (benign or malignant) in cases of hormone replacement therapy were found.
A recent study by Timmerman et al 8 reported a sensitivity rate of 76.4% in the detection of endometrial polyps using the pedicle artery sign. This sign includes the color Doppler findings of a feeding vessel to the endometrium. This was a much higher rate than our experience, as only 33% of our patients with a pathologic diagnosis of polyps demonstrated a vascular pedicle at sonography, although it was reassuring that we did not find any false-positive results.
The patient population in this study did have higher percentages of both detectable color Doppler flow and gray-scale findings indicative of a polyp in the premenopausal population as compared to the postmenopausal population. This study also demonstrated that in postmenopausal women presenting with a thick endometrium the pedicle artery sign was not very useful, with only one of seven polyps demonstrating flow as a vascular pedicle.
In placing the results of this study in a clinical context, its limitations should also be considered. These include: (1) lack of a histopathologic gold standard (hysterectomy) in every studied case due to practical limitations and (2) the fact that premenopausal women with abnormal uterine bleeding may present with an endometrial thickness that is inherently difficult to evaluate because it may be affected by exogenous or endogenous sex hormones. (3) The average time from sonographic examination to actual tissue collection averaged 74 days, which diminished the validity of the retrospective observation. However, one can argue that when considering lesions such as polyps or malignancy, they are unlikely to change in this short timeframe. (4) The number of patients in this study with endometrial malignancy was small. (5) Focal endometrial lesions can be missed on blind biopsies such as those that were utilized in these samples. False-negative rates for office-based endometrial biopsy procedures have been reported at more than 15%, and false-negative rates for dilation and curettage have been reported as high as 10%.33-36 (6) The retrospective nature of this study meant that all cases collected during this period do not necessarily represent all cases of endometrial flow detected due to incomplete medical records, patient omission, or lack of adequate follow-up.
In summary, the aforementioned indicate that color Doppler imaging should not be utilized as an independent diagnostic predictor but rather as a useful adjunct technique in the detection of endometrial abnormalities in women undergoing sonographic evaluation. This study also indicated that polyps, with their characteristic vascular pedicle, can be missed by gray-scale sonogram but may be seen by color Doppler imaging. Finally, this study found that other endometrial pathologies, benign and malignant, have an overlapping pattern of present or absent color flow, as has been reported in the literature.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.