
Abstract
This report describes the use of echocardiographic measurements for the assessment of left ventricular diastolic function in two young patients with newly diagnosed hypertension. Measurements for the assessment of left ventricular relaxation and filling pressures included mitral inflow, Doppler tissue imaging (DTI), color M-mode propagation velocity slope, and the isovolumic relaxation time. The mitral inflow, propagation velocity, and isovolumic relaxation time measurements were all within normal limits; however, DTI measurements of the E′ velocity at the septal and lateral annulus were significantly reduced in both patients. Further visual inspection demonstrated discrete proximal septal wall thickening that is thought to be modulated by pressure loading (i.e., increased afterload due to hypertension) and ejection. These findings may represent a “transitional state” of early ventricular remodeling and organ failure in the development of hypertensive disease. In summary, DTI appears to be more sensitive compared to other markers in identifying abnormal relaxation in subclinical hypertensive disease and normal ejection fraction.
Introduction
Echocardiographic assessment of the “diastology workup” includes a combination of structure, valvular interrogation, ventricular relaxation, and filling pressures1,2 (Table 1). The role of the sonographer is to obtain high-quality tracings in patients with known or suspected cardiac disease.1-4 Standard echocardiographic measurements for the assessment of filling pressures include the mitral inflow E/A ratio, E-wave deceleration time, A-wave duration, pulmonary vein ratio of the systolic and diastolic profiles, occasionally atrial reversal velocity and duration, and mitral E-wave divided by the Doppler tissue imaging (DTI) E′-wave velocity (i.e., E/E′ ratio). Additional measurements for the assessment of filling pressures include the Valsalva maneuver, size and volume of the left atrium (LA), and the presence or absence of pulmonary hypertension (HTN).1-5 Assessment of ventricular relaxation, however, is limited to mitral inflow E/A ratio, E-wave deceleration time, DTI E′-wave velocity, isovolumic relaxation time (IVRT), and color M-mode propagation velocity (Vp)1,2 (Figure 1). An increase in LA volume and elevated pulmonary pressures are helpful only in identifying patients with suspected elevated filling pressures and do not provide insights to the extent of ventricular relaxation. In addition, the majority of these measurements are unreliable in patients with normal systolic function (ejection fraction [EF] > 50%), limiting the application of this technology in populations such as patients with systemic HTN.1,2,5,6 Of the aforementioned measurements, mitral inflow, Vp, and IVRT have the greatest load dependence, convoluting assessment of ventricular filling pressures and relaxation.1,2,4-7 However, DTI is relatively load independent and can be accurately assessed in patients with various cardiac disorders in abnormal and normal EF.1,2,5-8 A low DTI E′-velocity (< 8 cm/s) is considered abnormal1,8-10 and reflects a reduction of velocity and displacement of the myocardium in early diastole. As a consequence, slowing of myocardial relaxation in early diastole increases the time constant of relaxation (tau > 48 milliseconds) and is considered a marker of intrinsic myocardial disease notwithstanding geometry.1,8-10 Identifying those who are at risk of developing abnormal relaxation and concomitant elevated filling pressures, with treatment in the early stages of hypertensive disease, would be desirable.7,11-13 This report describes the use of standard echocardiographic measurements for the assessment of left ventricular (LV) relaxation and filling pressures in two young patients with newly diagnosed HTN and normal EF. In addition, this report draws attention to subtleties in early ventricular remodeling identified by 2D imaging and the strengths and limitations of Doppler techniques.
Echocardiographic Correlates in the Estimation of Relaxation and Filling Pressures.
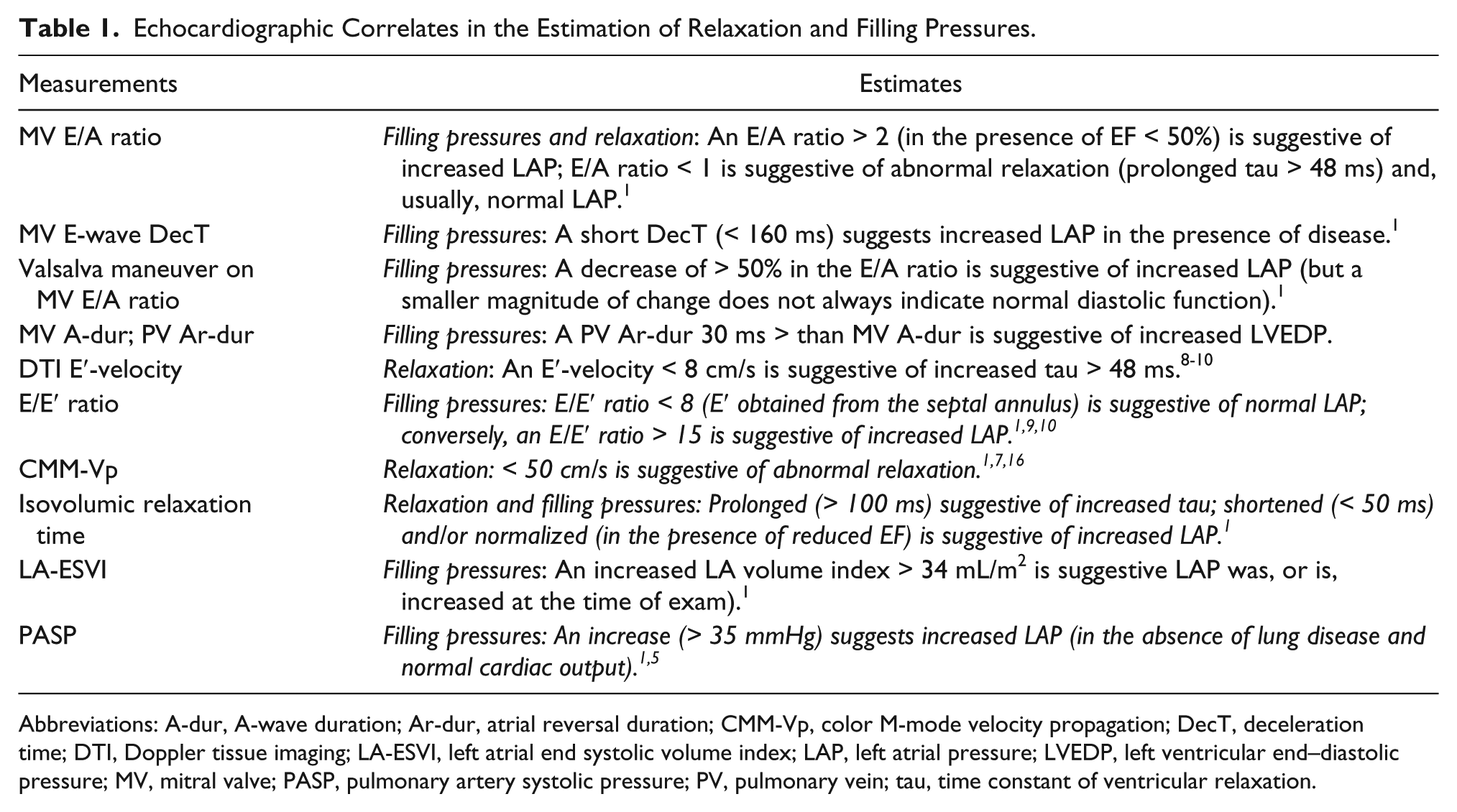
Abbreviations: A-dur, A-wave duration; Ar-dur, atrial reversal duration; CMM-Vp, color M-mode velocity propagation; DecT, deceleration time; DTI, Doppler tissue imaging; LA-ESVI, left atrial end systolic volume index; LAP, left atrial pressure; LVEDP, left ventricular end–diastolic pressure; MV, mitral valve; PASP, pulmonary artery systolic pressure; PV, pulmonary vein; tau, time constant of ventricular relaxation.
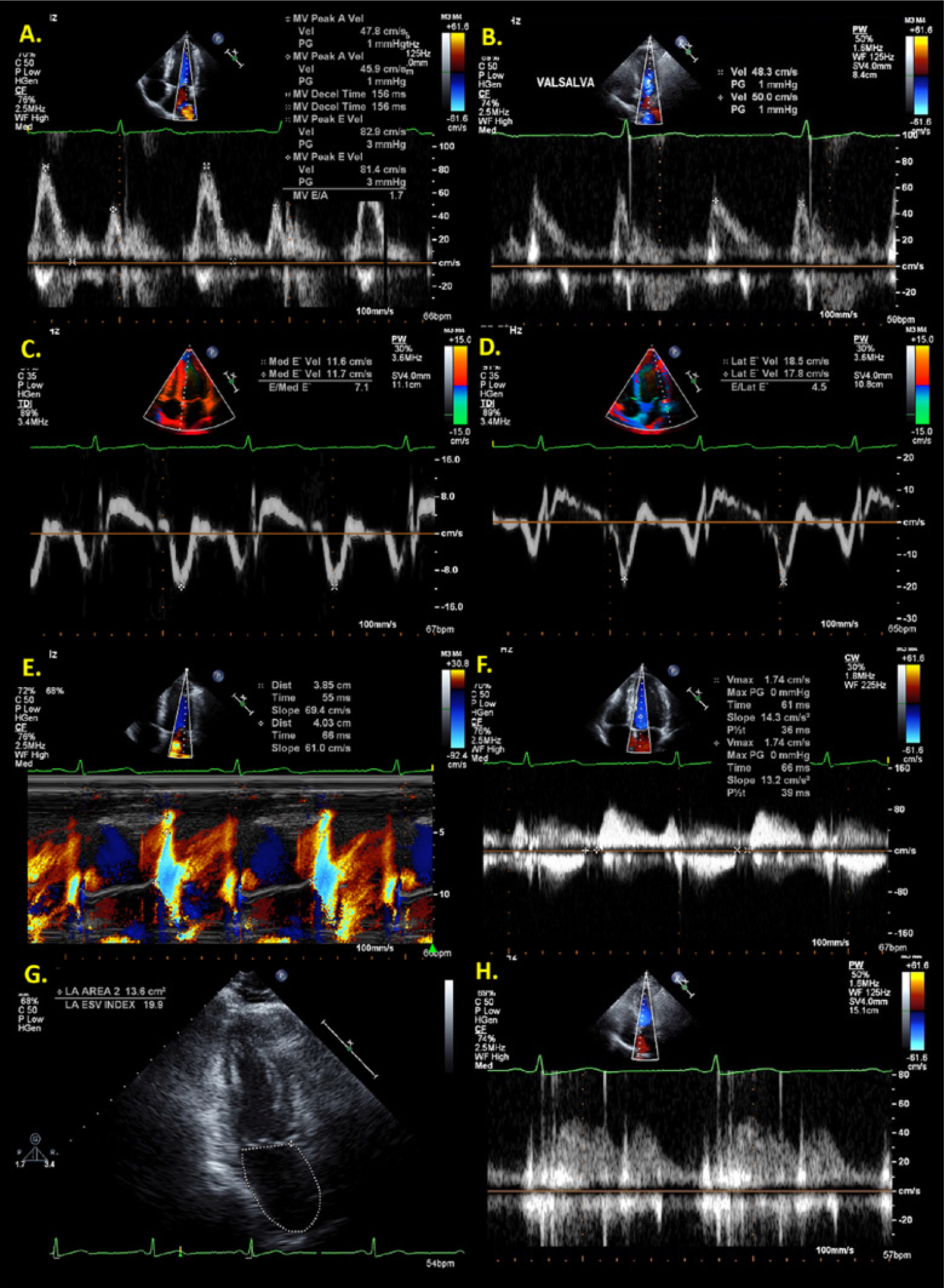
Echocardiographic measurements for the assessment of relaxation and filling pressures in a 31-year-old male patient; all values are normal for age. 1 (A) Mitral inflow Doppler recording obtained with the sample volume (SV) placed at the leaflet tips; (B) mitral inflow Doppler recording obtained with the SV placed at the leaflet tips during the strain phase of the Valsalva maneuver; (C-D) Doppler tissue imaging obtained with the SV placed at septal and lateral annulus; (E) color M-mode propagation velocity slope measurements obtained at early diastole with the cursor placed across the mitral valve inflow, a decrease in the sector depth, and an increase in the color pulse repetition frequency baseline; (F) isovolumic relaxation time obtained with the SV placed between the mitral inflow and left ventricular outflow; (G) measurements of left atrial area and end-systolic volume index obtained from the apical two-chamber at end-ventricular systole; (H) pulmonary vein Doppler recording obtained with the SV placed within 1 cm of the right upper pulmonary vein.
Case Studies
Case 1
Patient Demographics
A 36-year-old man with chest pain and newly diagnosed systemic HTN presented to the echocardiography laboratory for the evaluation of structural heart disease. Body surface area was 2.0 m2, and the patient’s blood pressure obtained at the time of the echocardiogram was 130/86 mm Hg. The patient was in normal sinus rhythm throughout examination.
Echocardiography
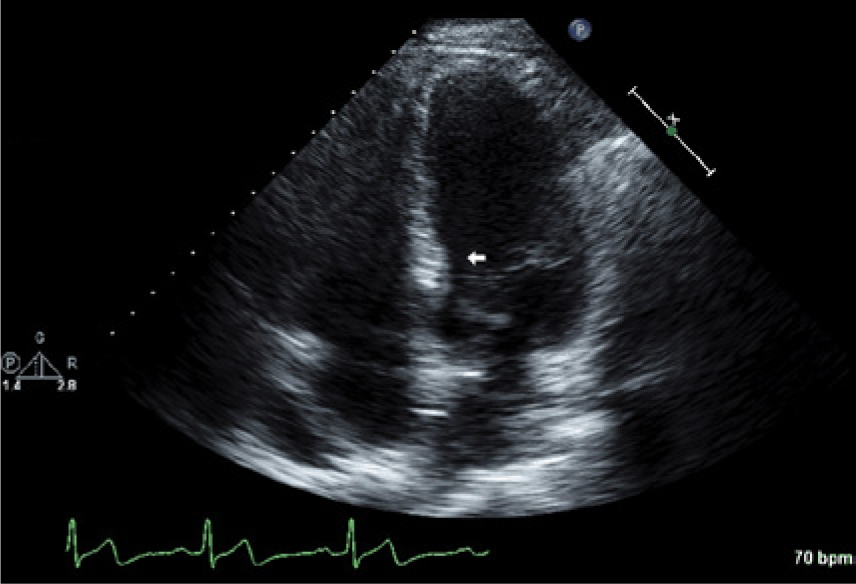
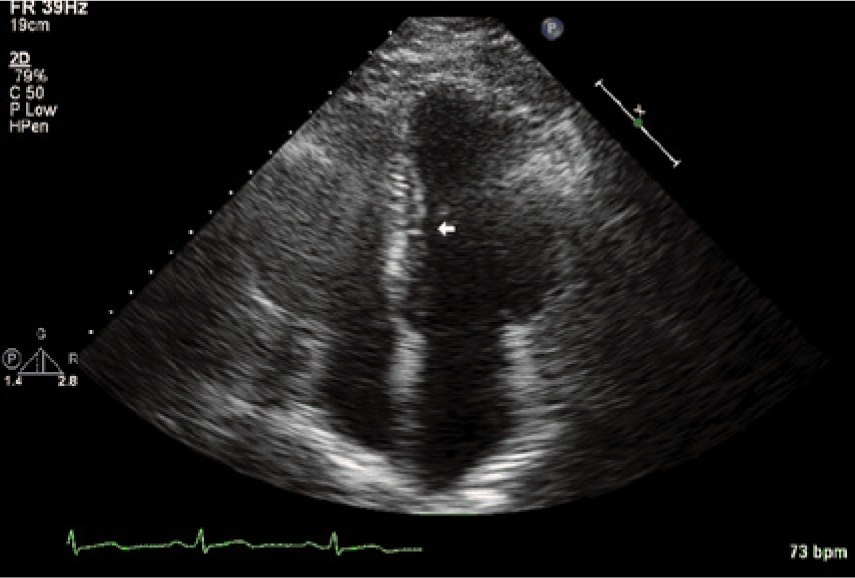
The echocardiogram demonstrated normal LV cavity size, upper-normal wall thickness (Figure 2A), and normal systolic function. The EF was estimated at 70%; heart rate was 69 beats per minute; and stroke volume was 85 mL, with an estimated cardiac output of 5.9 L/min. LV mass index was 101 g/m2; all values were normal. The parasternal long axis view demonstrated discrete proximal septal thickening (Video 1, arrow) but was more pronounced in the apical 4-chamber view (Video 2, arrow). No other structural or valvular abnormalities were reported. Pulmonary artery systolic pressure could not be estimated due to the lack of the tricuspid regurgitation continuous-wave Doppler signal. There was no physiologic or structural evidence of pulmonary hypertension. Left atrial area and end-systolic volume index values were normal at 20 cm2 and 26 mL/m2, respectively. Left atrial indices and LV mass were calculated per the area-length formula. 14 All measurements were obtained during end-expiratory apnea and were made with current echocardiography guidelines and standards. 14
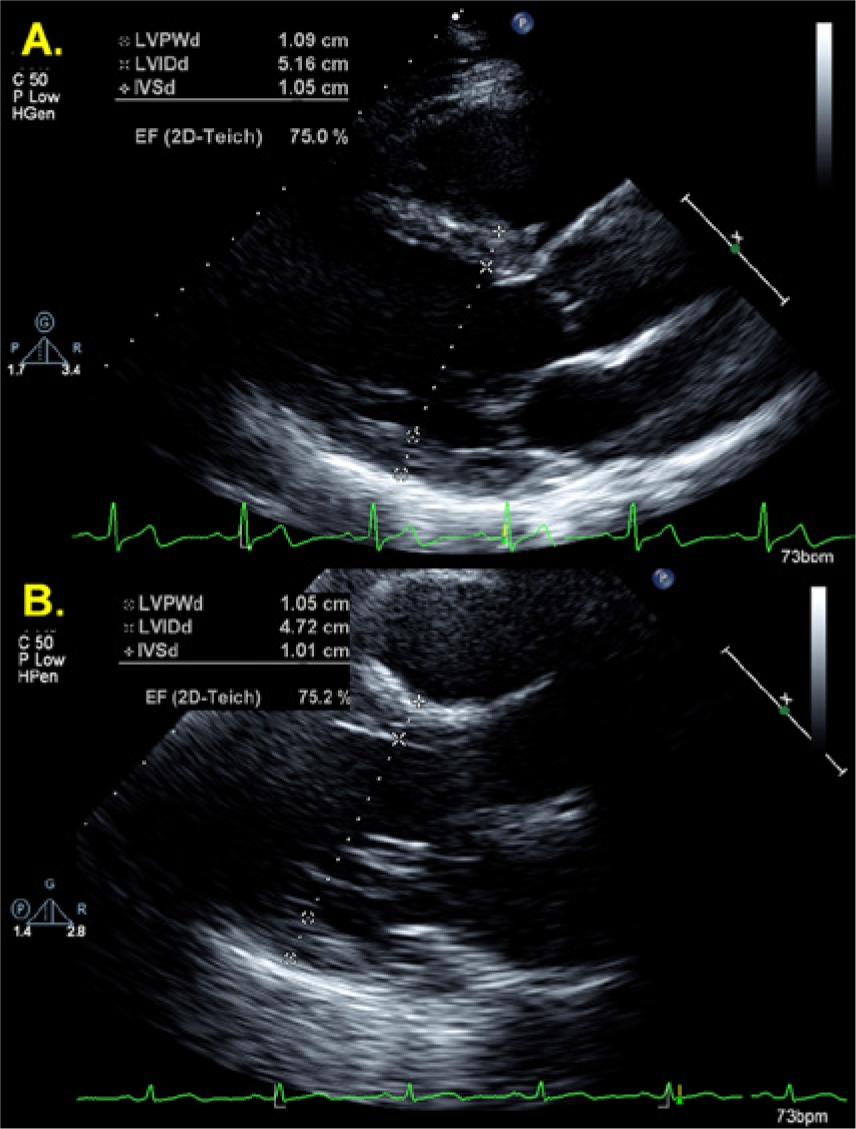
Case 1 (A) and Case 2 (B): 2D measurements of left ventricular wall thickness and chamber size obtained at end-diastole from the parasternal long axis view. LVPWd, left ventricular posterior wall thickness, end diastole; LVIDd, left ventricular internal dimension, end diastole; IVSd, interventricular septal wall thickness, end diastole; EF (2D-Teich), 2D measures of ejection fraction by Teicholz method.
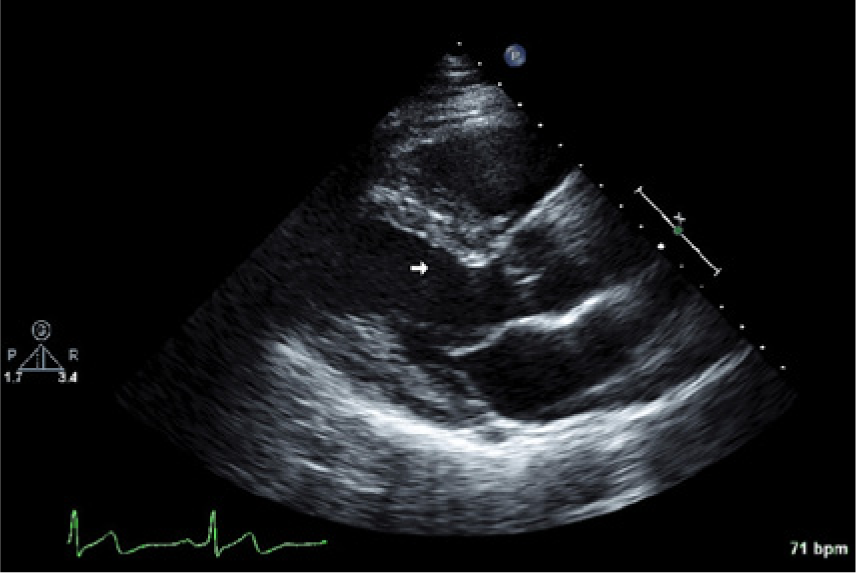
Case 1 showing a parasternal long axis view suggesting discrete proximal ventricular septal thickening (arrow).
Case 1 showing an apical four-chamber view suggesting discrete proximal ventricular septal thickening (arrow).
Diastolic Function Assessment
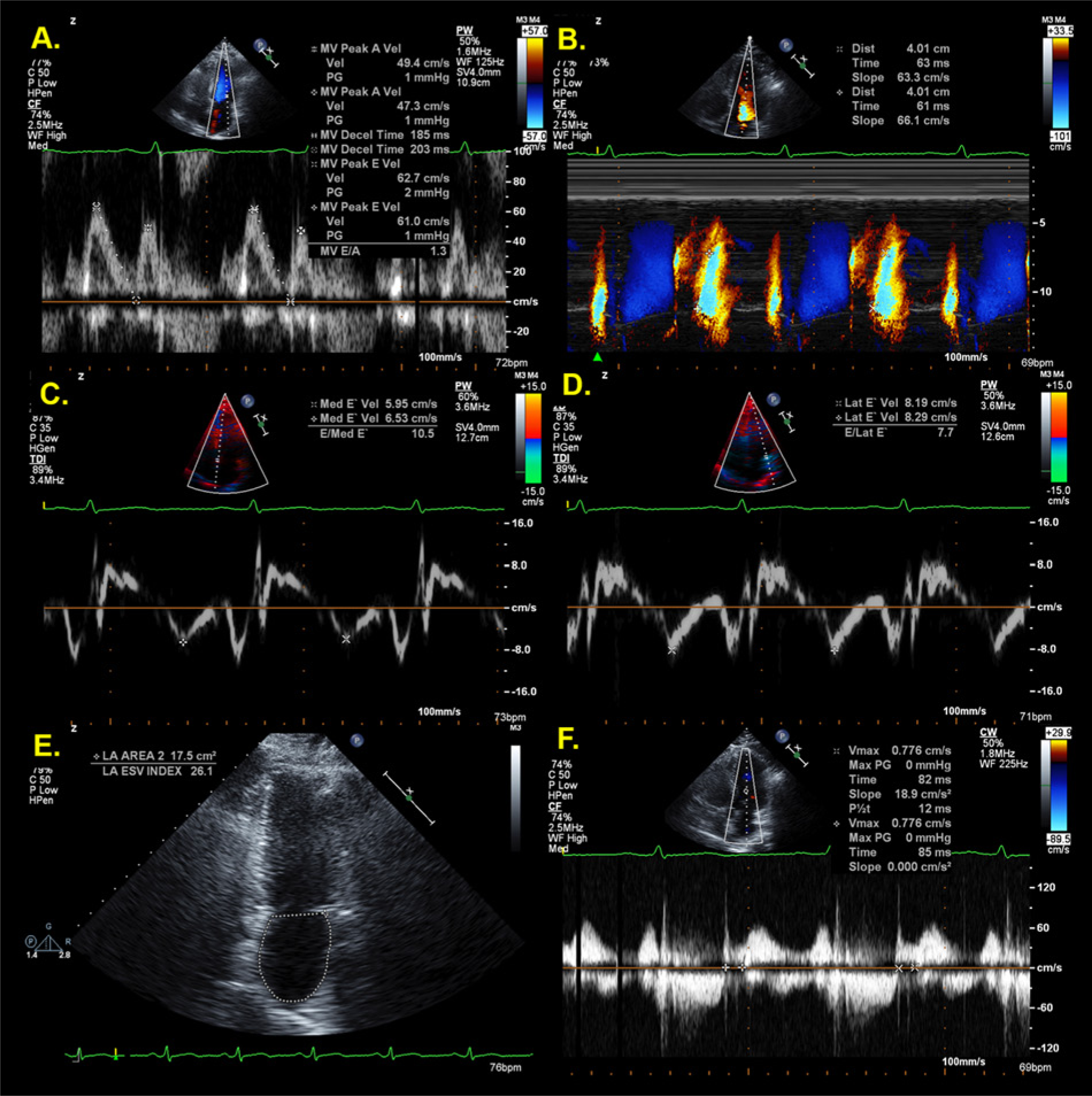
A comprehensive protocol for the assessment of diastolic function was performed1-3 (Figure 3), and measurements are reported in Table 2. All values for the assessment of diastolic function were attainable except for the pulmonary vein atrial reversal velocity and duration, due to incomplete spectral Doppler profiles (images not shown). A normal E/A ratio in a 36-year-old is 1.53 ± 0.40 with 95% confidence intervals of 0.73 and 2.33. 1 The E/A ratio was 1.2, and the mitral E-wave, E-wave deceleration time, and A-wave values were also normal (see Table 2). A normal IVRT mean value is 67 ± 8 milliseconds with 95% confidence intervals of 51 and 83 milliseconds, 1 and the IVRT in this patient was 78 milliseconds. A normal Vp value is > 50 cm/s, 1 and the Vp in this patient was 52 cm/s. The averaged E/E′ ratio was 8, indicating no evidence of elevated filling pressures (≤ 8, normal), which is supported by normal left atrial size and volumes. Based on the values reported from the guidelines and standards for the assessment of diastolic function, 1 a normal septal E′-velocity in a 36-year-old is 15.5 ± 2.7 cm/s with 95% confidence intervals of 10.1 and 20.9 cm/s; normal lateral E′-velocity is 19.8 ± 2.9 cm/s with 95% confidence intervals of 14 and 25.6 cm/s. In this patient, the septal E′-velocity averaged 7.0 cm/s, and the lateral E′-velocity averaged 11.0 cm/s. Both DTI values were well beyond the normal range and confidence limits, whereas all other echocardiographic indices of diastolic function were normal.
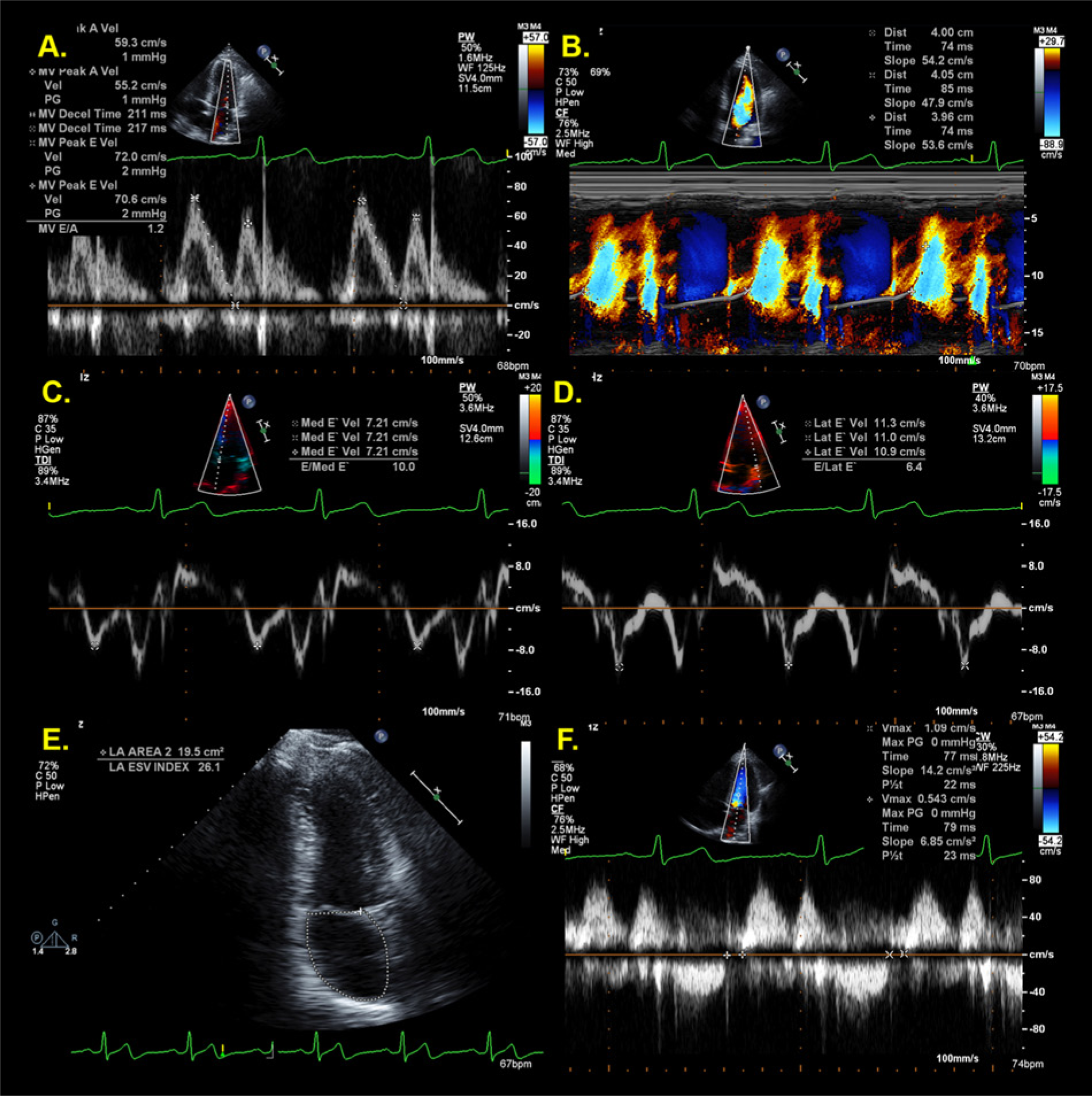
Echocardiographic measurements for the assessment of relaxation and filling pressures in the patient presented as case 1; all values are normal except for the DTI E’-velocities (C, D). 1
Echocardiographic Data for Case 1 and Case 2 a .
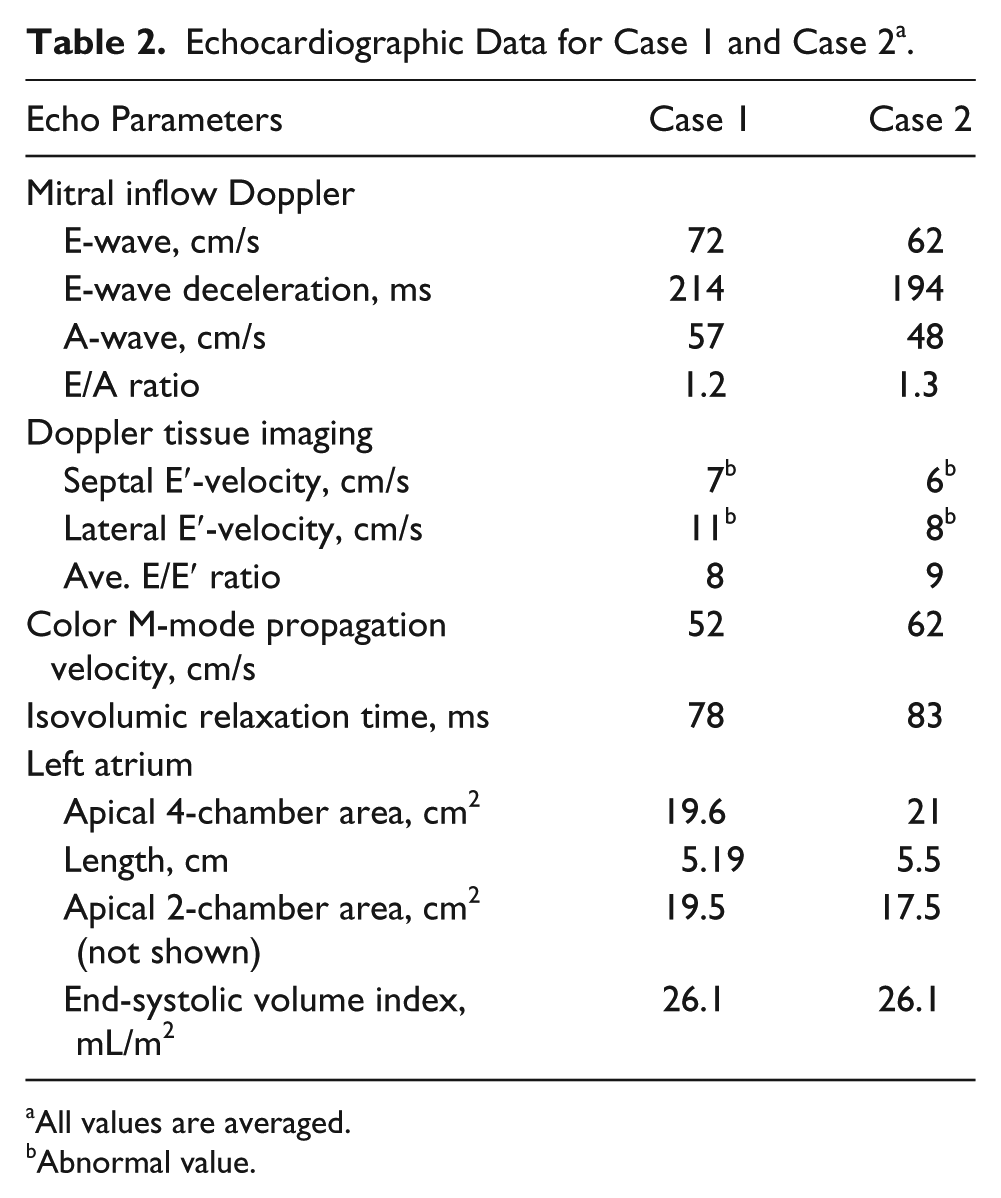
All values are averaged.
Abnormal value.
Case 2
Patient Demographics
A 38-year-old man with pedal edema and borderline systemic HTN presented to the echocardiography laboratory for the evaluation of structural heart disease. Body surface area was 2.18 m2, and the patient’s blood pressure at the time of the echocardiogram was 124/82 mm Hg. The patient was in normal sinus rhythm throughout examination.
Echocardiography
Striking similarities were seen between cases 1 and 2, as the 2D echocardiogram demonstrated normal LV cavity size and upper normal wall thickness (Figure 2B). The EF was estimated at 70%; heart rate was 69 beats per minute; and stroke volume was 65 mL, with an estimated cardiac output of 4.5 L/min. LV mass index was 100 g/m2. All values were normal. The parasternal long axis view demonstrated discrete proximal septal thickening (Video 3, arrow) but was more pronounced in the mid- to distal septal wall in the apical four-chamber view (Video 4, arrow). Otherwise, no structural or valvular abnormalities were reported. The left atrial area and end-systolic volume index values were normal at 19 cm2 and 26 mL/m2, respectively.
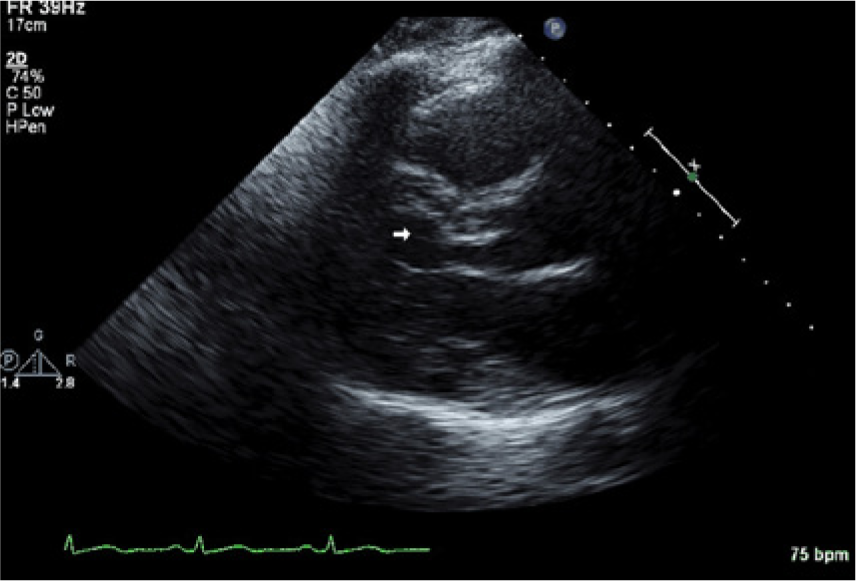
Case 2 showing a parasternal long axis view suggesting discrete proximal ventricular septal thickening (arrow).
Case 2 showing an apical 4-chamber view suggesting discrete proximal ventricular septal thickening (arrow).
Diastolic Function Assessment
As seen in case 1, all values for the assessment of LV diastolic function were normal except for the DTI velocities (Figure 4, Table 2). The averaged E/E′ ratio was 9, indicating no evidence of elevated filling pressures, which is supported by normal left atrial size and volumes. The septal and lateral E′ velocities were abnormal, measuring 6.0 cm/s and 8.0 cm/s, respectively. The DTI E′-velocity values in both cases were well beyond the normal range and confidence limits, thus providing insights to early relaxation abnormalities and a proposed “transitional state” in early ventricular remodeling in subclinical hypertension.
Echocardiographic measurements for the assessment of relaxation and filling pressures in the patient presented as case 2; all values are normal except for the DTI E’- velocities (C, D). 1
Discussion
Hypertension affects more than 65 million people in the United States, increasing the risk of heart failure, stroke, and myocardial infarction. 15 A recent study demonstrated that lowering blood pressure along with antihypertensive therapy in individuals with diastolic dysfunction may improve the rate of ventricular relaxation measured by DTI. 11
Echocardiography therefore plays a pivotal role in the evaluation of diastolic function, recording abnormalities in ventricular relaxation and filling pressures with reasonable accuracy.1,8-10
The characterization of ventricular filling pressures and relaxation has been extended from traditional measurements of the mitral inflow velocities and IVRT to color M-mode Vp and DTI.1,7,16,17 The mitral inflow velocities and ratio provide a rudimentary introduction to relaxation and filling pressures as the foundation for the assessment of diastolic function.1,2 If the E-wave velocity is low (< 50 cm/s), the left atrial pressure is most likely normal, irrespective of E/A ratio and ventricular function; conversely, if the mitral inflow pattern appears normal (E/A > 1, normal E-wave deceleration time) in a patient with significantly reduced EF (< 30%), the left atrial pressure is most likely elevated.1-4 Because ventricular compliance decreases as stiffness increases in patients with systolic dysfunction, the ventricular “suction effect” in early diastole is exacerbated. The result is an increase in driving pressure from the LA to LV in early diastole, respectively. As the transition occurs from stage 1 to stage 2 diastolic dysfunction, LA pressure gradually increases, and the E-wave velocity and deceleration time increase, resulting in a “normal appearing” or so-called pseudo-normal pattern seen on the mitral inflow Doppler display.1-4,8-10 Conversely, as the transition occurs from moderate to severe (stage 3) diastolic dysfunction, the E-wave tends to increase, and the E-wave deceleration decreases; these findings are due to a significant decrease in ventricular compliance and relaxation, marked increase in LAP, resulting in a restrictive filling pattern as seen on the Doppler display.
However, estimation of filling pressures and relaxation in a hypertensive patient with a “normal appearing” mitral inflow pattern and normal EF cannot be accurately dichotomized.1,3,4,6,7,12 The height of DTI E′-velocity and E/E′ ratio corrects for the obscurity on transmitral filling and normal EF by accurately estimating relaxation and filling pressures. The IVRT is the first phase of diastole, representing the period between aortic valve closure and mitral valve opening, and it is a direct estimation of LV relaxation. 1 However, the E/A ratio and IVRT have limited accuracy given the influence of preload, which opposes the effect of LV relaxation. 1 Color M-mode Vp represents the flow from the mitral valve to the apex in early diastole and has shown to correlate with the rate of LV relaxation.1,16,17 However, Vp can be “pseudo-normal” in patients with abnormal relaxation, normal LV volumes, and EF.1,6 The Vp, IVRT, and mitral inflow measurements are most accurate in patients with depressed LV systolic function,1,6 which is in sharp contrast to the patients presented in this report.
When diastolic function was assessed by multiple echocardiographic parameters, DTI was the only method that identified a relaxation abnormality in these patients. The mitral inflow velocities, IVRT, and Vp were within the normal range in both patients, demonstrating the confounding effects of ventricular function and EF on these measurements. These findings are consistent with those of Rovner et al. 7 showing that the mitral inflow velocities and time intervals, IVRT, and Vp parameters could not discriminate among different groups with and without HTN and normal EF. This is supported by the notion that mitral inflow velocities and Vp may have greater load dependency than DTI and are influenced by several factors, including atrial pressure, rate of ventricular pressure decline, ventricular “suction” effect, and end-systolic volume.1,2,6
A recent report by Mogelvang et al. 12 included a large community-based population of 1036 participants with HTN, diabetes, ischemic disease, and normal and abnormal EF. Measurements of DTI, color DTI–displacement imaging, and mitral inflow parameters were included. Results demonstrated that in the general population, persons with HTN, diabetes, or ischemic disease and normal EF have impaired cardiac function by DTI independently of the other parameters measured. In other words, DTI was the most powerful predictor of intrinsic cardiac dysfunction after adjusting for age, sex, body mass index, and heart rate. In addition, it has been reported that relaxation abnormalities detected by DTI precede deformation indices such as strain imaging 13 (i.e., velocity of shortening and lengthening have decreased, but absolute percentage shortening or lengthening is normal) and are present in 21% of patients with hypertension without LV hypertrophy and normal EF. 7 Thus, low DTI velocities could represent an early measure of myocardial organ damage in HTN that precedes ventricular hypertrophy.7,11
There are some limitations inherent in the case studies reported. There is a lack of invasive hemodynamics in these cases, which would confirm or exclude relaxation abnormalities and elevated filling pressures. However, several reports have validated DTI1,8-10 and provide partition values in normal patients of various ages,1,2,7-10,11,16-19 supporting the abnormal DTI findings.
Conclusion
Two-dimensional imaging identified early ventricular remodeling, prompting detailed evaluation of diastolic function. Mitral inflow velocities, IVRT, and Vp were normal, demonstrating the confounding effects of ventricular function on these measurements. DTI was superior in detecting a relaxation abnormality compared to other echocardiographic techniques in these patients with normal EF. This finding underscores the importance of careful evaluation of diastolic function, especially in patients with newly diagnosed HTN, and may represent a subclinical abnormality in early relaxation in hypertensive disease.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.