
Abstract
Transabdominal sonography has proved to be an efficacious imaging technology to diagnose urolithiaisis. However, the location of the calculus may cause a sonographic examination to be limited. Since the majority of ureteral stones are located in the distal ureter, calculi may not always be visualized transabdominally, especially if the bladder is not full. This case study demonstrates the use of transvaginal sonography in the diagnosis of distal ureterolithiasis and discusses the optimal visualization of a ureteral stone in a female patient using transvaginal sonography. The case demonstrates the importance of this imaging method when distal urinary tract stones are suspected.
Keywords
Introduction
Urolithiaisis is a common disorder of the urinary system, with approximately 10% of the population in the United States experiencing at least one event during their lifetime. 1 Urolithiasis is a condition resulting from mineral and acid salts forming stones within the urinary system. 2 The exact cause of urolithiasis in any given case may be unknown since there can be several contributing factors to the condition. Certain foods may aid the formation of kidney stones, as high-protein and high-salt diets have both been associated with stone formation. 3 Urolithiasis is more common in Caucasians and is developed more commonly in men than in women, though the incidence of urolithiasis in women is steadily increasing. 3 The strongest risk factors, however, are a family or personal history of urolithiasis. 3 Risk factors particularly affecting women are pregnancy, medications, underlying diseases, and urinary tract infections.4,5
Urolithiasis usually forms when crystal-forming substances are not being adequately diluted by the fluid in urine. 2 There are several types of kidney stones, but the leading mineral in urolithiasis formation is calcium. Calcium stones, consisting of calcium oxalate that is mostly acquired through diet, comprise up to 70% of kidney stones.2,4 Other types of urolithiasis that are prevalent are struvite stones, which grow rapidly and usually form as a response to infection; uric acid stones; and cysteine stones. 2 Uric acid calculi usually occur in people who don’t drink enough fluids or who lose too much fluid, and cystine stones usually form in people with a genetic condition that causes their kidneys to excrete too many amino acids. 2
Patients with urolithiasis may be asymptomatic or symptomatic. The symptomatic patient may present with acute flank pain, nausea, vomiting, and fever. 3 Intravenous urography (IVU) and computed tomography (CT) are the standard imaging modalities to detect renal calculi.3,6,7 These imaging modalities are not hindered by bowel gas or body habitus in evaluating for calculi, which makes them preferable to sonography. However, the use of intravenous radio-opaque contrast and the length of time required to perform an IVU make this imaging method impractical in an emergency setting.1,7 CT can reliably detect urinary calculus regardless of size or location, but this method of imaging exposes the patient to radiation.1,6 Such exposure to ionizing radiation should be avoided in particular in pregnant women and women of childbearing age. Because of these drawbacks, transvaginal sonography is a common alternative method used in the detection of urolithiasis.
Transabdominal sonography has proven to be an effective imaging modality in the assessment of nephrolithiasis, but it has been less effective in diagnosing ureterolithiasis. 8 Transvaginal sonography can help overcome the limitations of transabdominal imaging. The higher frequencies of the transvaginal transducer and the closer proximity of the ureter to the transducer make transvaginal sonography more sensitive at detecting ureterolithiasis compared to transabdominal sonography. 9 In addition, the symptoms of urinary calculi often mimic the symptoms of pelvic disorders, and in these cases transvaginal sonography can be used to safely assess for both ureteral calculi and pelvic abnormalities in a single examination. 9
Case Report
A woman in her early twenties presented with persistent right lower quadrant pain that was only mildly alleviated when she lay in the fetal position. The patient said she felt “achy” and was cramping. She had not been experiencing nausea or vomiting and was afebrile at the time of her presentation. Because of the right lower quadrant pain, appendicitis was suspected and a sonogram of the right lower quadrant was ordered. A 12 MHz linear transducer was used on a Philips iU22 ultrasound machine (Philips Ultrasound, Bothel, WA). Imaging of the right lower quadrant did not show an inflamed appendix; however, a dilated distal right ureter was visualized (Figure 1). A pelvic sonogram was then ordered to further investigate, as right lower quadrant pain can also be associated with menstrual pain, pelvic inflammatory disease (PID), ovarian torsion, and ruptured ovarian tumors. 9
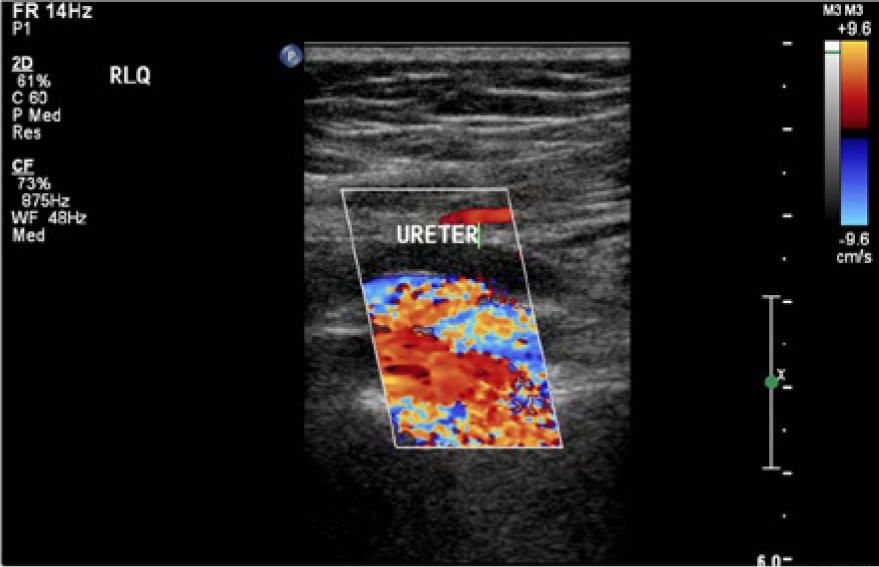
Initial sagittal transabdominal color Doppler image of the right lower quadrant showing a dilated right ureter.
Transabdominal and transvaginal sonograms were performed on the same Philips iU22 ultrasound machine using a 5 MHz curvilinear transducer and an 8 MHz endovaginal transducer, respectively. The pelvic sonogram was unremarkable, but an incidental finding of a dilated right distal ureter with an intraluminal calculus was noted. The echogenic foci found in the ureter demonstrated posterior acoustic shadowing and color Doppler twinkle artifact, characteristic of stones (Figures 2 and 3).6,7 The stone was measured in both sagittal and transverse planes and noted to be 4 mm long and 3 mm wide (Figure 4). Because the calculus was so well visualized sonographically and demonstrated the classic sonographic findings of a calculus, no additional imaging studies were done and a diagnosis of ureteral stone with hydroureter was made. Spontaneous passage of the stone was expected due to its small size. The patient was sent home and told to drink large amounts of fluid to help expel the stone.

Transvaginal sonogram showing a hyperechoic structure with posterior acoustic shadowing within the lumen of the right ureter.
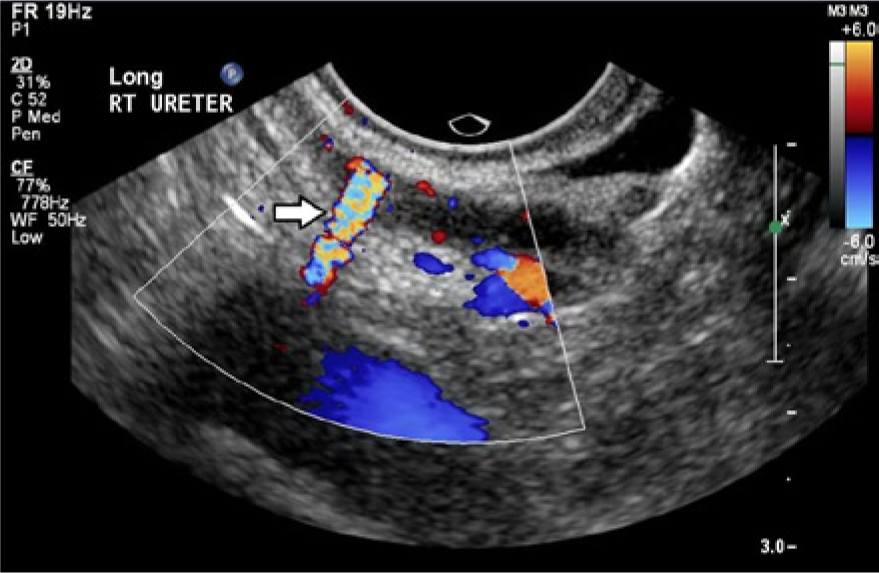
Transvaginal color Doppler image in the sagittal plane showing a prominent twinkle artifact (arrow) of the right ureteral stone.

Transvaginal sonogram in the sagittal plane showing the dilated right ureter with an intraluminal calculus (calipers), which was measured to be approximately 4 mm in size.
Less than a week after her initial visit to the emergency room the patient returned because of recurrent right lower quadrant pain. To investigate her pain, a renal sonogram was ordered that showed moderate hydronephrosis in the right kidney. There was moderate dilation of the right ureter, and the stone was able to be visualized in the distal ureter transabdominally. The right ureteral jet was not well visualized. The stone still measured 4 mm in diameter. The patient was discharged with instructions to take ibuprofen every 12 hours for the pain, continue to drink large amounts of fluid, and to follow up with a urologist in two weeks.
Discussion
Accurate sonographic diagnosis of ureterolithiasis may not have been possible without demonstration of the specific noted sonographic characteristics. In this case, the calculus demonstrated all the positive findings associated with a stone. The calculus was an echogenic structure that demonstrated posterior acoustic shadowing. 6 It also exhibited the twinkle artifact with the application of color Doppler. 6 The stone was clearly defined within the ureter, making the diagnosis of an intraluminal ureteral stone unmistakable.
There are various treatment options for urolithiasis, and the course of action is dependent on the number, size, and location of the stone. All stones measuring less than 5 mm in diameter have a high chance of spontaneous passage within 40 days, and therefore no medical intervention is usually felt to be necessary.1,8 However, if medical intervention is needed, there are several options available. Extracorporeal Shock Wave Lithotripsy (ESWL) is the most common type of kidney stone intervention. ESWL uses high-intensity, focused ultrasound waves to fracture the stone into small pieces that can easily be expelled through the urinary tract. 3 Larger stones that need surgical removal are usually removed via percutaneous nephrolithotomy (PNL). A small incision is made on the affected side that allows the necessary percutaneous instrumentation to be inserted into the body to remove the stone. 3 PNL has been shown to be more effective at clearing stone fragments than ESWL. 3
The prognosis for urolithiasis is good, and many cases spontaneously resolve. For those that do not resolve on their own, medical intervention has proven to be very successful. However, despite optimal treatment of urolithiasis, recurrence is common. People who develop one stone have a 50% chance of developing another stone in their lifetime. 3
Conclusion
This case illustrates the significance of using transvaginal sonography in a woman with a sudden onset of right lower quadrant pain. Transvaginal sonography was successfully used to evaluate the pelvis and the distal right ureter. Although the pelvic examination was unremarkable, ureterolithiasis of the right ureter was shown. Sonography was the sole imaging modality necessary in this case because it provided optimal images, making the interpreting physician confident in his diagnosis. The use of transvaginal sonography specifically allowed accurate characterization of the stone in order to diagnose the ureteral calculus while at the same time ruling out other pelvic disorders. The use of sonography alone avoided any unnecessary exposure to ionizing radiation. Because of the short examination time, optimal visualization of pathology, and safety characteristics, transvaginal sonography should be the procedure of choice in pregnant women and women of childbearing age with a possible distal urinary obstruction.
Footnotes
Acknowledgements
The author would like to thank Courtney Camp, C.W. Scheidt, Dee Sharrock, Michelle Klenklen, Lori Bryan, Marsha Glaskey, Jenny Seaton, and Mark Tinsley for their assistance, leadership, and guidance.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.