
Abstract
Wilson disease, also known as hepatolenticular degeneration, is a disorder in the liver that results in the improper metabolism of copper, which leads to accumulation of excessive amounts of this vital trace element in the liver, brain, eyes, and other organs. Although copper is essential for normal physiologic function, it can become toxic and life-threatening when too much is present within critical organs, especially the liver and the brain. There is no cure for Wilson disease, and patients affected with this disorder face a lifetime of treatment. Fortunately, the disease is very treatable if diagnosed before significant damage to the liver or brain occurs. This article presents a case study on Wilson disease and the role of sonography in helping diagnose and monitor patients with this condition.
In 1912 neurologist Samuel Alexander Kinnier Wilson published the first research related to a rare, genetically inherited autosomal recessive disease. 1 Even though the clinical recognition of Wilson disease occurred more than 100 years ago, it still remains a poorly understood disorder of the liver’s ability to properly metabolize copper. In subsequent years, numerous individuals have contributed to the knowledge of this disease. Their findings have enabled better diagnosis and earlier treatment, which in turn have provided more favorable outcomes for affected patients. This progression in diagnosis and treatment continues today as new research and more sensitive testing and treatment procedures are developed. As the sensitivity of these tests increases, the number of new reported cases of Wilson disease is also increasing. Sonography plays an important role in helping the physician diagnose and follow the treatment of patients with this liver disorder.
Case Report
A right upper quadrant abdominal ultrasound examination of a man in his mid-40s was requested as part of an annual checkup to evaluate the condition of his liver, based on the diagnosis of Wilson disease that had been made a decade earlier. The patient stated that his diagnosis with Wilson disease began as an incidental finding during surgery to remove his gallbladder. A series of tests confirmed the initial diagnosis, and chelation treatment was started immediately. A combination of medications was given for approximately 3.5 years to complete the chelation process and to detoxify his body of excess copper. Once acceptable levels of copper were reached, he began a regimen of 50 mg of zinc orally three times a day, which adequately controlled the absorption and excretion of copper. The patient said that the side effects of the medication cause nausea and general abdominal discomfort but that he remained compliant and had no other complications resulting from the disease. In fact, he remained optimistic for future improvements in treatment.
A series of gray-scale images of the liver were obtained in the longitudinal and transverse scanning planes with a Phillips iU22 scanning system and a broadband, curved array C5-2 transducer (Figures 1–5). For comparison purposes, Figures 1A and 5A of a normal liver are also included. The patient’s liver presented as fatty and difficult to assess with sonography; the interpreting physician stated that the liver demonstrated increased echogenicity without evidence of a focal mass, which was consistent with hepatic parenchymal disease.
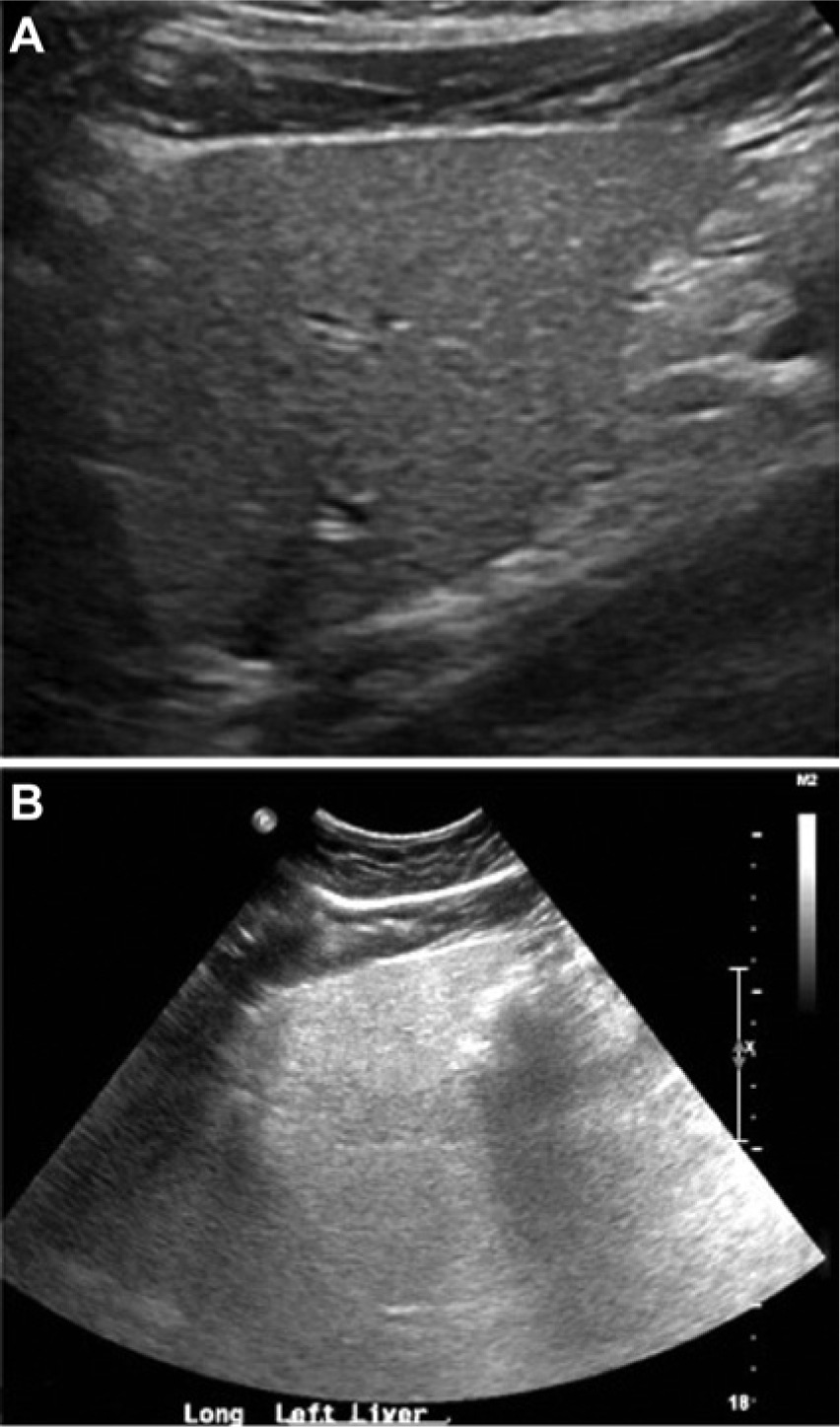
(A) Longitudinal image of the left lobe of a normal liver showing normal tissue echogenicity and texture. (B) Longitudinal image of the left lobe of the liver along a comparable plane (A) in the patient with Wilson disease, showing diffuse, nonspecific increased echogenicity with no evidence of any discrete masses and diminished tissue penetration causing poor visualization of the deeper tissue segments.

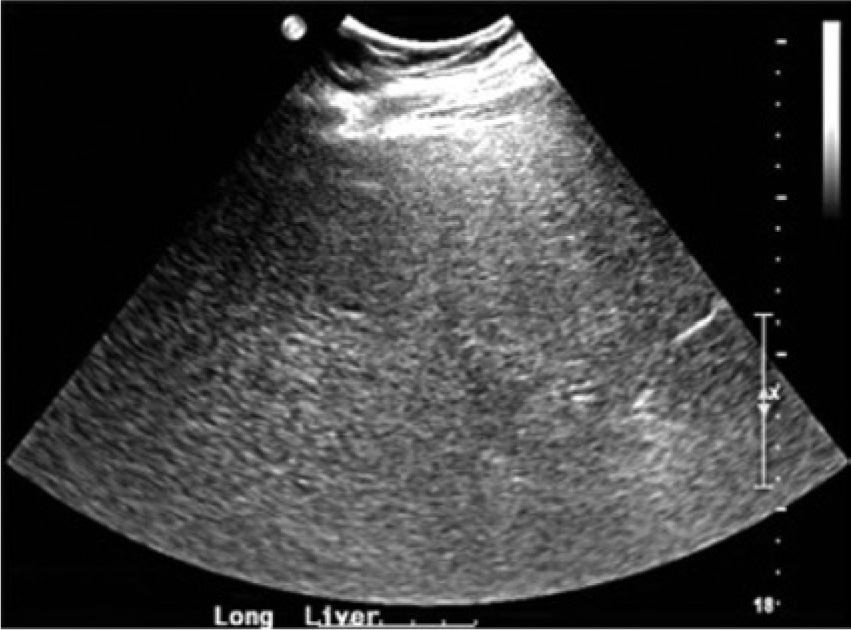
Transverse image of the left lobe of the liver in the patient with Wilson disease showing similar echogenicity to Figure 1B.
Longitudinal image of the right lobe of the liver in the patient with Wilson disease, showing the same echogenicity and tissue characteristics of the left lobe.
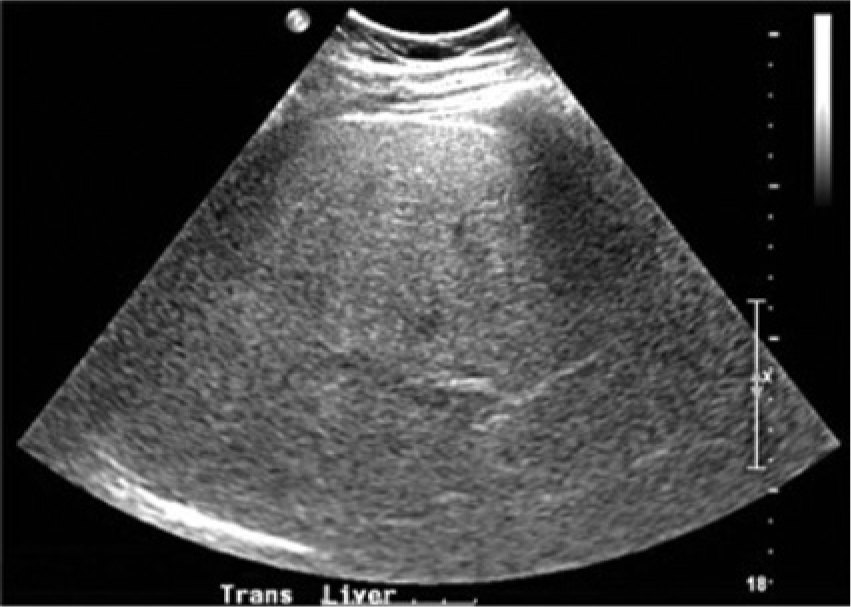
Transverse image of the right lobe of the liver in the patient with Wilson disease showing a similar echogenicity to Figure 3.
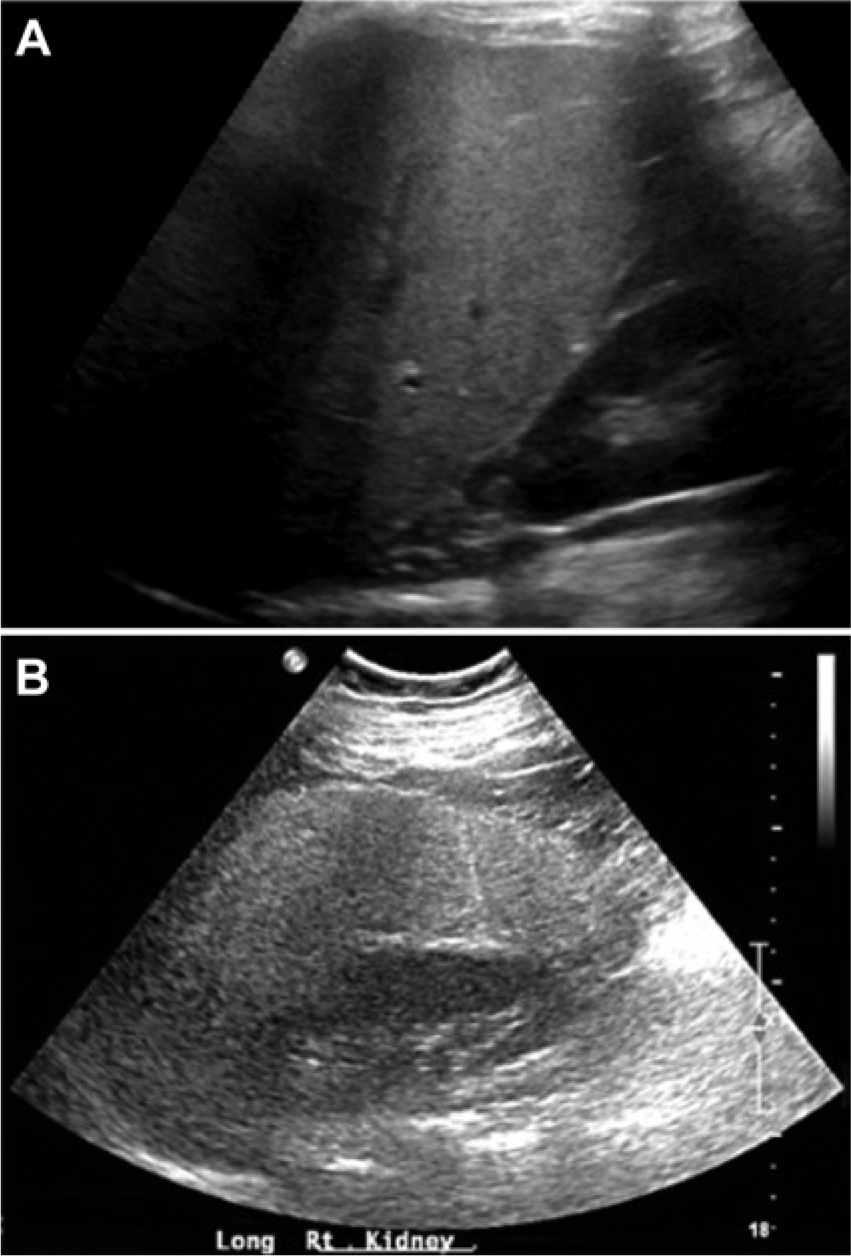
(A) Longitudinal image of the right lobe of a normal liver and right kidney showing normal tissue echogenicity, tissue penetration, and texture. (B) Longitudinal image of the right lobe of the liver and right kidney along a comparable plane (A) in the patient with Wilson disease, showing diffuse, nonspecific increased echogenicity and diminished tissue penetration causing poor visualization of the right kidney.
Discussion
Wilson disease, also known as hepatolenticular degeneration, is a rare autosomal recessive metabolic disorder of the liver in which the organ cannot eliminate excess copper. Copper, in minute amounts, is an essential element needed for many critical functions, including “oxidative metabolism, neurotransmitter synthesis, free radical detoxification, iron uptake, and connective tissue maturation in cells.” 2 Typically, more copper than necessary is ingested; it is stored in the liver until needed, and excess amounts are excreted through the biliary system to maintain a healthy balance. 3 In Wilson disease, the liver is unable to rid itself of excess copper, which results in organ dysfunction and, if not treated, liver failure. As the disease progresses, copper begins accumulating in other areas of the body, including the brain, eyes, kidneys, and heart, with subsequent impairment of the affected organs.1,4,5
The hepatocytes are the functional cells of the liver and are responsible for creating ceruloplasmin, which is an enzyme with six copper atoms; its function is to carry the majority of plasma copper throughout the body via the circulatory system. In addition, the hepatocytes transfer excess copper into the biliary system for eventual elimination in the feces. Wilson disease involves a mutation of the ATP7B gene, which interferes with the attachment of copper to ceruloplasmin and inhibits the transfer of excess copper into the bile. Thus, a toxic level of copper slowly builds up in the liver, resulting in hepatocellular damage, liver disease, and eventual passage of copper into the bloodstream, which results in toxic accumulation of this heavy metal in other organs. Hepatocellular damage can result in hepatomegaly, acute liver failure, hepatitis, chronic active hepatitis, and cirrhosis.1,2 However, many patients do not present with liver dysfunction as a result of Wilson disease; instead, neurologic and psychiatric disorders are the first clinical manifestations, since the brain is most often the second organ affected. 3
The basal ganglia, cerebellum, and brain stem are common areas of the brain affected by copper accumulation. In addition, “atrophy of the cortex and the cerebral white matter” has been noted in numerous studies. 6 Neurologic symptoms can vary widely but often present as “tremor, incoordination, dystonia, rigidity, difficulty with fine motor movements, and dysarthria.” Common psychiatric disturbances “range from depression, including suicide attempts, to temper tantrums, delusions, sexual exhibitionism, hyperkinetic behavior, and paranoia.” 3 Another clinical sign of Wilson disease is the formation of Kayser-Fleischer rings in the eyes, which are deposits of copper around the cornea of the eye. These rings may appear as red, bright green, blue, yellow, or brown. No significant clinical problems are associated with the development of these rings, and they tend to disappear once treatment of the disease is initiated. 2
The diagnosis of Wilson disease is made difficult by the wide range of nonspecific clinical symptoms exhibited by patients and the great variability in the age of affected individuals. It is possible for patients to be asymptomatic and the disease not present until later in life. The onset of the symptoms associated with this disease more typically occurs in adolescence and young adulthood, since it takes time for enough copper to accumulate and reach levels high enough to interfere with organ function. However, patients as young as 3 to as old as 72 have been newly diagnosed with this disease.1,2 The severity of symptoms is directly related to the amount of copper accumulation in the body. Because of the difficulty in diagnosing Wilson disease, it can take up to two years from the time that clinical symptoms appear to treatment. 1 Advanced cases of this disease in the brain can leave the patient bedridden and unable to care for oneself. In addition, severe cases of this disease in the liver can be fatal unless the patient receives a liver transplant. It is imperative to begin treatment immediately upon diagnosis, since early detection and treatment can reverse symptoms and prevent life-threatening damage to the liver and brain.
Diagnosis of Wilson disease is based on numerous clinical findings, including evidence of liver disease, neurologic and/or psychiatric symptoms, the presence of Kayser-Fleischer rings, decreased levels of serum ceruloplasmin, and, in advanced cases, elevated levels of urinary copper excretion. Computed tomography, magnetic resonance imaging, and sonography are the preferred imaging modalities used to help in the diagnosis of this disease. Depending on the stage of the disease, sonographic examination of the abdomen usually reveals hepatomegaly and/or signs of liver disease, including evidence of hepatitis, fibrosis, fatty infiltration, and cirrhosis. Since these signs of liver disease are nonspecific in nature, a diagnosis of Wilson disease is not rendered on the basis of sonographic appearance of the liver; other diagnostic procedures are usually performed. Splenomegaly is also generally noted.1,4,7,8 However, there are documented cases of patients diagnosed with Wilson disease in which the liver appeared normal during sonographic examination. 9 Sonography and magnetic resonance imaging are also used to image the structures of the brain most often affected, especially the basal ganglia. Transcranial sonography demonstrates increased echogenicity within structures related to the basal ganglia.6,10 Although there are many clinical signs and symptoms associated with Wilson disease, none of these are diagnostic in and of themselves; it usually takes a combination of these manifestations to render an accurate diagnosis. The gold standard for diagnosis is a liver biopsy that demonstrates elevated copper content.1 –3
Once diagnosed with Wilson disease, the patient must carefully follow a lifetime regimen of drug treatment, modifications in diet, and other efforts to limit exposure to copper. Chelation therapy, or detoxification of heavy metals, is the initial treatment to rid the body of free copper found in the bloodstream and not covalently bound to ceruloplasmin. 11 The removal of excess copper is accomplished by a combination of oral medications while the patient’s levels of serum copper are closely monitored. Penicillamine was the first oral medication used in chelation therapy, but its side effects, especially on patients with neurologic symptoms, were excessive. Trientine was the second copper-chelating agent used, but it also had significant adverse side effects on patients, causing significant neurologic symptoms. Today zinc is the preferred drug for treating Wilson disease. Unlike penicillamine and trientine, which bond to free copper in the body for urinary excretion, zinc inhibits the absorption of copper in the intestines.3,11 Once a normal copper level is attained, zinc is considered to be adequate therapy for maintaining a healthy level of copper absorption and excretion. Dietary restrictions include ensuring that not more than 1 mg of copper is ingested a day. It is advised to avoid copper supplements and foods high in copper content, such as shellfish, nuts, chocolate, whole wheat, and organ meats. In addition, steps need to be taken to reduce copper consumption in drinking water. These include using only distilled water for drinking and cooking and installing copper removal systems in drinking water lines.3,11
Conclusion
Although Wilson disease is considered to be rare, knowing the signs and the symptoms of this condition is applicable to sonologists and sonographers. As better diagnostic tools become available and awareness of this disease increases, sonographers should expect to see more instances of this life-threatening illness. Whether it is diagnostic imaging of the affected organs, aiding in a liver biopsy, or conducting follow-up studies, sonography can play a significant role in helping to alleviate the devastating effects of this uncommon condition.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.