
Abstract
Intrauterine contraceptive devices (IUD) are a popular method of birth control, typically with minimal side effects, and are used worldwide. Serious side effects such as uterine perforation are rare. Most often, a perforated IUD is found in the intraperitoneal space, although in rare instances, an IUD may perforate to the urinary bladder. In the case presented, a combination of 2D and 3D sonography was used to identify a missing IUD within the urinary bladder. The IUD was removed by cystoscopy without serious consequences to the patient.
Sonography is the initial imaging modality of choice when searching for a missing intrauterine device (IUD) because of its widespread availability, low cost, lack of ionizing radiation, and minimally invasive nature. 1 Transvaginal sonography is the most common examination ordered to confirm proper placement of an IUD. Bladder perforation by an IUD is an extremely rare event with less than 70 reported cases. 2 In the case below, transvaginal sonography failed to locate the device, illustrating the importance of performing a complete examination. If the IUD is not visualized, the examiner should not assume that the IUD has been expelled. Utilization of all sonographic options (transvaginal, transabdominal, 2D and 3D volume assessment) should be made, and in the case presented, they were able to definitively identify the lost IUD, allowing for prompt removal.
Case Report
A P2002 woman in her 30s presented to the office of her obstetrician/gynecologist with a complaint of missing IUD strings. Her relevant medical history consisted of two deliveries by cesarean section. Eighteen months after her second delivery, she had a Mirena (Bayer Healthcare Pharmaceuticals, Wayne, New Jersey) IUD inserted without incident. Four weeks following the IUD insertion, she returned to the office and complained of a pulling sensation with urination. Trace blood was appreciated on urine analysis. Urine culture results were negative. The IUD strings were visualized in the cervix on pelvic examination. Her complaints spontaneously resolved at that time.
Seven months after IUD insertion, the patient returned to the office noting that she could feel the IUD strings earlier in the week but could no longer feel them. At that time, the locator strings were not appreciated on pelvic examination by her gynecologist. A transvaginal sonogram was ordered to locate the IUD. The sonographic examination was performed using a GE Voluson 730 Pro V (GE Healthcare, Milwaukee, Wisconsin), with multifrequency transducers. A 2D and 3D volume assessment was performed by an American Registry for Diagnostic Medical Sonography (ARDMS)–credentialed sonographer having more than 25 years of scanning experience.
The transvaginal sonogram showed the endometrium to be empty (Figure 1). The IUD was not visualized in the myometrium, nor was it seen in the immediate adnexa. The patient’s bladder was filled and transabdominal sonography was performed to obtain a more global view of the pelvis. A T-shaped IUD and locator strings were visualized completely within the urinary bladder (Figures 2–4). A 3D volume assessment clarified this finding (Figure 5). The patient was referred to a urologist for cystoscopy and foreign body removal. On cystoscopy, mild nonerythematous, edematous changes were noted in the inferior posterior midline of the bladder. An IUD with locator threads was visualized floating freely. It was removed from the bladder intact. The patient tolerated the procedure well and had no further complaints.
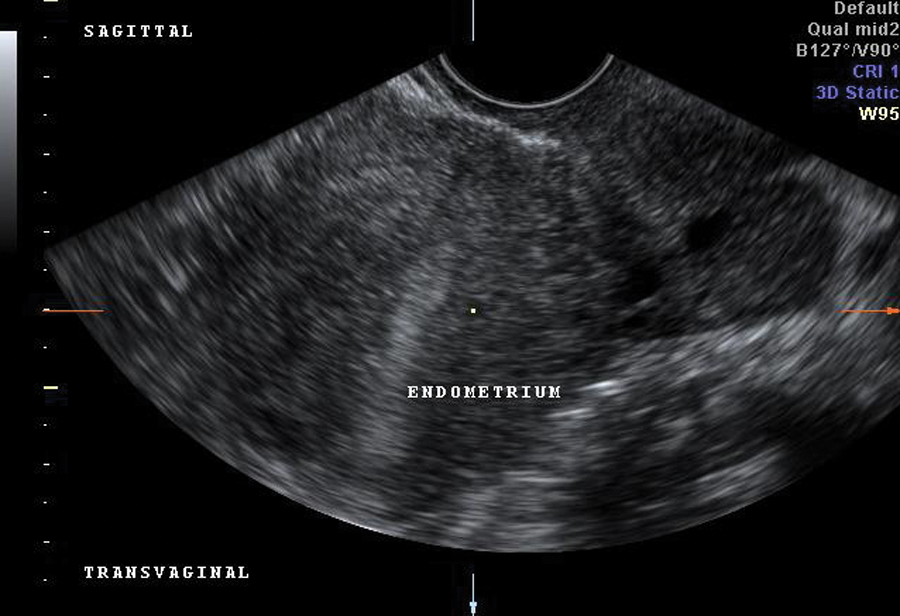
Transvaginal image showing the empty endometrium with nonvisualization of the intrauterine device.
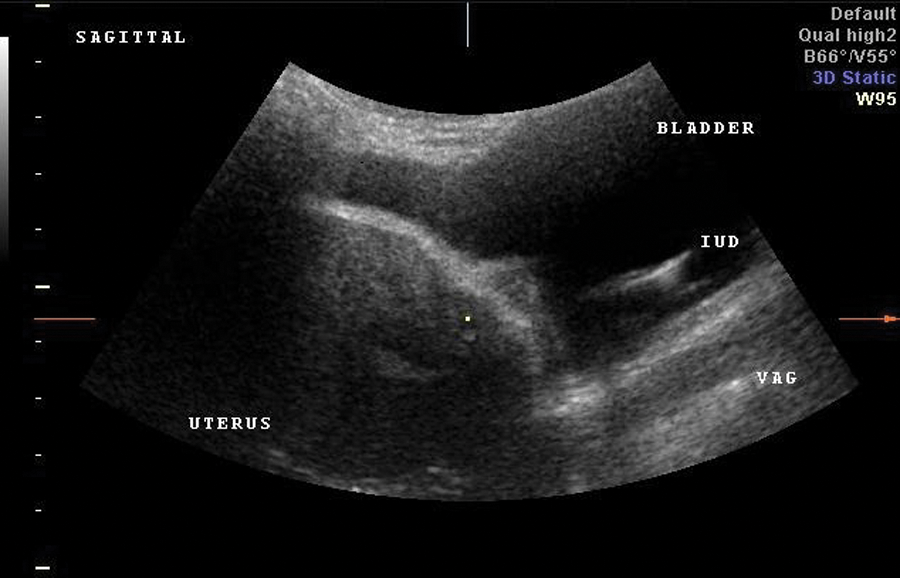
Sagittal transabdominal sonogram showing a partially distended bladder with visualization of the intrauterine device (IUD).
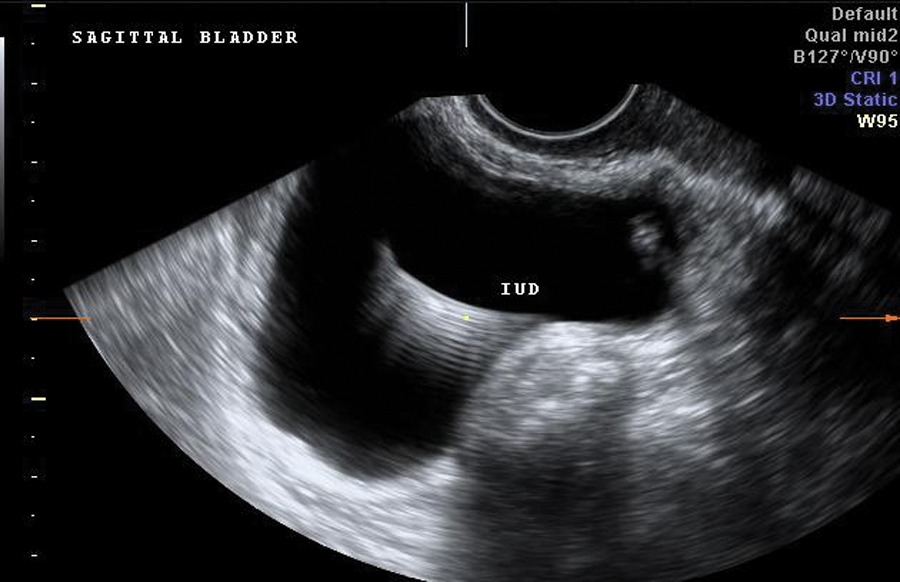
Sagittal transabdominal sonogram centered on the urinary bladder showing the intrauterine device (IUD) with a ring-down artifact.
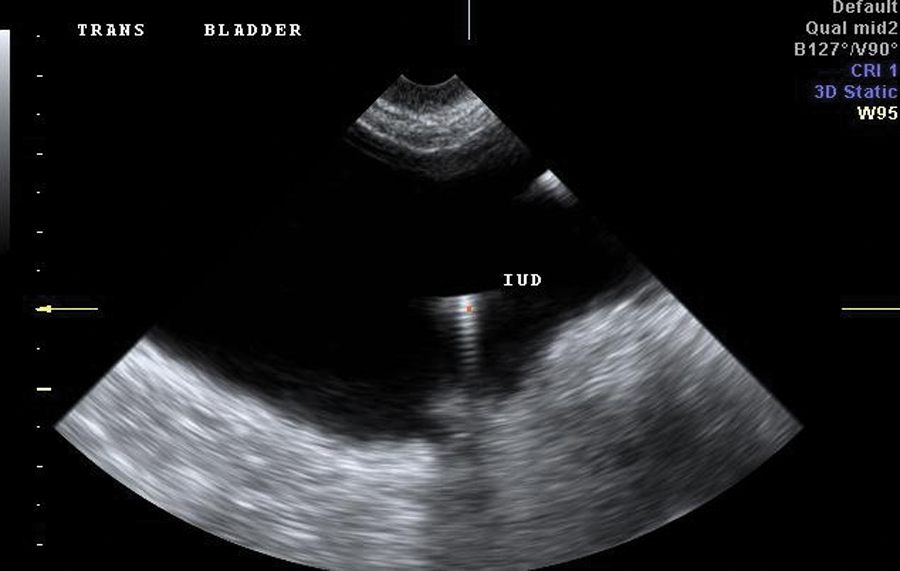
Transverse transabdominal sonogram of the distended urinary bladder with visualization of the intrauterine device (IUD).

A 3D volume rendering showing the location of the intrauterine device (IUD) within the urinary bladder, demonstrating the IUD arms (<), IUD body (<<<), and strings (*).
Discussion
Intrauterine devices, commonly known by the acronym IUD, are the most widely used reversible method of birth control. It is estimated that more than 150 million women worldwide rely on IUDs for contraception. 3 During five years of IUD use, pregnancy occurs in less than 1% to 2% of insertions. 3 The IUD has earned its popularity through efficacy, low cost, ease of use, and low risk of complication. Risks related to IUD use include pregnancy, infection, irregular bleeding, embedment, expulsion, and perforation. An IUD that completely perforates the uterus may migrate to any neighboring structure, including the urinary bladder. 4 Diagnostic sonography is a reliable method of localizing an IUD after insertion and whenever its location is questioned.
Currently, two types of IUDs are available: copper and hormonal. 3 Both are T-shaped plastic devices embedded with barium sulfate to aid in imaging. Strings are attached to the tip of the device to facilitate identification of the location and for removal. In the United States, IUDs are marketed under two brand names: ParaGard T 380A Intrauterine Copper Contraceptive (Teva Pharmaceuticals USA, Sellersville, Pennsylvania) and Mirena levonorgestrel-releasing intrauterine system (Bayer Healthcare Pharmaceuticals). The ParaGard device has copper wire wrapped around T-shaped plastic. It is believed that ParaGard impedes sperm mobility and interferes with implantation,3,5 and it offers protection from pregnancy for up to 10 years after insertion. The Mirena device releases a form of progestin called levonorgestrel (LNG). It is believed that the LNG in Mirena impedes sperm mobility, prevents the endometrium from ripening, and damages sperm; in some cases, it also prevents ovulation and thus may continue to protect against pregnancy even when in an ectopic location.6,7 Levonorgestrel has been found to reduce menstrual bleeding and cramping, which has led to its approval for the treatment of menorrhagia and dysmenorrhea, adding to its popularity. Mirena remains active for 5 years after insertion.6,8
The benefits of IUD usage are clear. It is easy to use, offers effective contraception, and may decrease menstrual bleeding. Side effects are usually minimal. Serious risks such as pelvic inflammatory disease, expulsion of the device, and uterine perforation are rare. The most serious potential complication of an IUD is uterine perforation. Perforation can lead to intraperitoneal adhesions, intestinal penetration, intestinal obstruction, and/or damage to adjacent organs. 5 The risk is comparable between both copper and LNG IUDs and occurs in approximately 0.05 to 13 per 1000 insertions (average, 1.2/1000). 9
Most research suggests that perforation occurs at or soon after insertion.5,10 Successful placement of an IUD depends on the skill of the physician, timing of insertion, and anatomy of the uterus and cervix. A retroverted uterine position is the most common variant affecting perforation because of the extreme angle of the uterus to the cervix. 4 Other conditions that can contribute to IUD perforation are multiparity, recent abortion or pregnancy, delivery by cesarean section, lactation, and stifis.2,11 It is also possible for perforation to occur over time. The IUD can slowly migrate through the muscular wall of the uterus. 2
Symptoms suggesting an abnormally placed IUD typically include pain, cramping, irregular bleeding, dyspareunia, and lengthened or absent strings. 12 IUD locator strings should be appreciated on manual examination by the medical provider. When the strings are missing or a patient is symptomatic, imaging examinations should be performed to locate the IUD. It is most likely that the IUD is within the endometrium while the strings are not visible; 80% of missing IUDs are visualized in the endometrium, in which case, the strings have merely migrated through the cervix. 13 IUD perforation must be considered whenever the IUD is not visualized in the endometrial cavity. In cases of partial perforation, it is possible for the strings to be visible in the cervix while the IUD itself is misplaced.
A combination of 2D and 3D volume assessment sonographic imaging using both the transvaginal and transabdominal approach is recommended to confirm IUD location. Two-dimensional sonography allows for traditional images to be obtained, and 3D volume assessment renders multiple planes, yielding more precise information about location. It has even been suggested by some researchers that sonography be used after insertion and annually to confirm proper placement of an IUD. 14 If the IUD cannot be located in the endometrium, the uterus, the adnexa, and surrounding structures should be examined. Studies have shown that 80% of all complete IUD perforations migrate to the intraperitoneal space. 10 These IUDs are most often located in the region of the intestinal omentum or bowel wall. 9 If the IUD is not identified by sonography, x-ray, computerized tomography (CT), or magnetic resonance imaging (MRI) may be necessary. When an ectopic IUD is located, it should be promptly removed. This may be done in the clinical examination room using forctif, by laparoscopy, or, as in the case presented, via cystoscopy.5,15
Because of its close proximity to the uterus, an IUD can, in rare incidences, migrate to the urinary bladder. Current literature cites only 70 cases of either complete or partial bladder perforation by an IUD. 2 Most of the patients in these cases experienced urinary symptoms, and half of the reported cases resulted in stone formation around the IUD. 4 Bladder perforation should be considered whenever a patient with a “missing” IUD presents with urinary symptoms.
In the case presented, the IUD was found to have perforated the urinary bladder. It is possible, based on the patient’s time course of symptoms, that the IUD migration through the uterine wall occurred over time 4 and that the entry site may have been at the cesarean section scar. It is likely that the strings were visible and palpable until complete perforation occurred. The hormonal activity of the Mirena may have protected the patient from pregnancy even with the displaced IUD. Sonographic localization followed by prompt removal of the IUD limited the patient’s complications.
Conclusion
Bladder perforation by an IUD is a rare occurrence that can be proven by sonographic imaging. The addition of transabdominal sonography and 3D volume assessment may be necessary in cases where the IUD cannot be visualized by transvaginal sonography, as they improve the ability to verify the specific IUD location.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.