
Abstract
The objective of this study was to evaluate the cross-sectional area of the median nerve by ultrasonography before and after release of the transverse carpal ligament in patients with carpal tunnel syndrome. An additional goal was to correlate the cross-sectional area following surgery with clinical symptoms. Eighteen patients and 22 wrists were evaluated. All patients underwent Paine’s surgical technique for release of the transverse ligament. Cross-sectional area was calculated from sonograms taken at the pisiform bone level pre- and postsurgery. Postsurgical measurements were made at 4, 8, 12, and 96 weeks. Before surgery, the mean cross-sectional area was 19.7 mm2. The results following surgery were as follows: 4 weeks, 20.1 mm2; 8 weeks, 17.4 mm2; 12 weeks, 15.5 mm2; and 96 weeks, 13.5 mm2. Three patients remained clinically symptomatic at the time of their last follow-up visit. Cross-sectional area of the median nerve tends to increase 4 weeks after surgery for carpal tunnel syndrome, compared with the measurements taken prior to surgery, and then progressively decreases. There was no evidence of postprocedure correlation between the cross-sectional area of the median nerve and clinical symptoms.
Carpal tunnel syndrome is the most common compressive neuropathy of the upper limb.1,2 This disorder predominantly affects females, with ages typically ranging from 40 to 60 years. Carpal tunnel syndrome can be idiopathic or secondary, the latter more often in patients with diabetes, renal insufficiency, and hypothyroidism.
Numbness, paresthesia, pain in the median nerve territory, and decrease of motor strength are the classical clinical and physical findings reported during medical evaluation. 3
Although the clinical status plays a crucial role in the diagnosis of carpal tunnel syndrome, imaging methods provide complementary information to reach the final diagnosis. The assessment of the carpal tunnel structures by magnetic resonance (MR) studies is already well established in the literature. 4 Although the MR examination provides an excellent soft tissue contrast of the structures, it is expensive and time-consuming.5–8 It has been suggested that sonography should be the first imaging study to be performed in patients with carpal tunnel syndrome because of its availability, low cost, short time required, and the ability to evaluate the nerve and tendons in a dynamic fashion.1,5–7,9–12
We are reporting a study to evaluate the time course of changes in the cross-sectional area of the median nerve after release of the transverse ligament in patients with the diagnosis of carpal tunnel syndrome. A secondary aim is to determine whether there is any correlation between the cross-sectional area of the median nerve after ligament division and clinical symptoms.
Materials and Methods
Institutional review board approval was obtained for this prospective analysis. Patients were enrolled between October 1999 and December 2002. To be eligible, patients were required to fulfill the following criteria: (1) clinical symptoms, physical examination, and electromyography study compatible with carpal tunnel syndrome; (2) treatment failure with medication, physical therapy, and immobilization; (3) eligible for open surgery; (4) willingness to complete sonographic examinations before surgery and 4, 8, 12, and 96 weeks after surgery; and (5) median nerve must have a cross-sectional area measurement above 10 mm2 by dynamic ultrasound before surgery. 13 Patients with a previous history of fracture or surgery of the wrist, cervical myelopathy, and advanced stage of the disease such as hand atrophy were excluded from our analysis. Fifty patients comprised our initial population. Of these, 12 patients were excluded before surgery and 20 patients were excluded because they would not agree to undergo the required follow-up sonographic evaluations after surgery. A total of 18 patients with surgery on 22 wrists made up the final sample size.
All studies were performed at the discretion of the attending orthopedists to evaluate the cross-sectional area of the median nerve. The schedule of ultrasound examinations following surgery was standardized for all patients as 4, 8, 12, and 96 weeks. The sonographic imaging studies were performed using a Logic-700 (General Electric, Milwaukee, Wisconsin) or SD-800 (Philips Medical, Shelton, Connecticut) using a high-frequency linear array transducer. During the examination, patients were seated with the arms and hands in a resting anatomical position, palms upward, with the fingers and thumb extended over the examination table. The volar area was scanned in the longitudinal and transverse plans.
All sonographic examinations were performed by two board-certified radiologists (R.A.S. and C.A.A.) who have specialized in musculoskeletal imaging, with 10 and 5 years of experience, respectively. The radiologists followed an identical protocol for all examinations. First, the volar area was scanned in longitudinal and transverse planes searching for extrinsic lesions that could be the causal factor for carpal tunnel syndrome. Next, identification of the anatomical structures that provide the limit of the carpal tunnel was made; proximally, these were the pisiform and scaphoid and, distally, the trapezium and hamate. For preoperative examinations, identification of the transverse carpal ligament as a hyperechoic arched strip-shaped structure was made. The median nerve was identified as a hypoechoic rounded structure with a hyperechoic rim localized just inferior to the transverse carpal ligament on the transverse plane that remained static during finger movement. Finally, after identification of the median nerve in the transverse plane, the cross-sectional area of the median nerve at the level of the pisiform was measured.
Surgeries were performed under the guidance of two board-certified orthopedic surgeons (B.F.P. and C.H.F.) specializing in hand surgery, each with more than 15 years of experience. Prior to surgery, all patients were given Bier’s anesthesia, an intravenous regional technique often applied for extremity interventions. 14 The Paine retinaculotome, an open surgery commonly used to treat carpal tunnel syndrome, was used for all patients. 15
Statistical analyses were performed using SPSS 9.0 (SPSS, Inc, an IBM Company, Chicago, Illinois). A nonparametric method for repeated measurements (Friedman’s test) was used to compare the categorical variables across time. A P value less than .05 was considered statistically significant.
Results
All patients included in the present analysis were female, with a mean age of 45.2 years (range, 36–56 years). Eleven patients were white (61.1%) and 7 patients nonwhite (38.9%). Fourteen patients underwent unilateral intervention; 12 right wrists were included in the study. A total of 110 sonographic studies were performed: 22 before surgery and 88 after surgery.
Median nerve cross-sectional area data are summarized in Table 1 for each patient. Preoperatively, the group mean cross-sectional area of the median nerve was 19.7 mm2. Postoperatively, at 4 weeks, the group mean cross-sectional area was 20.1 mm2; at 8 weeks postsurgery, 17.4 mm2; at 12 weeks postsurgery, 15.5 mm2; and at 96 weeks postsurgery, 13.5 mm2. Friedman’s test demonstrated a statistically significant difference (P < .001) between the studies before surgery and 4, 8, 12, and 96 weeks after surgery. Figures 1 to 4 illustrate these findings. All patients but two demonstrated a decrease in the cross-sectional area of the median nerve compared with the preoperative value by the 96-week examination. Of note, only examinations that showed a cross-sectional area of the median nerve equal to or less than 19 mm2 before surgery reached the cutoff of 10 mm2 by the 96-week follow-up examination.
Median Nerve Cross-Sectional Area Data by Study Time Point
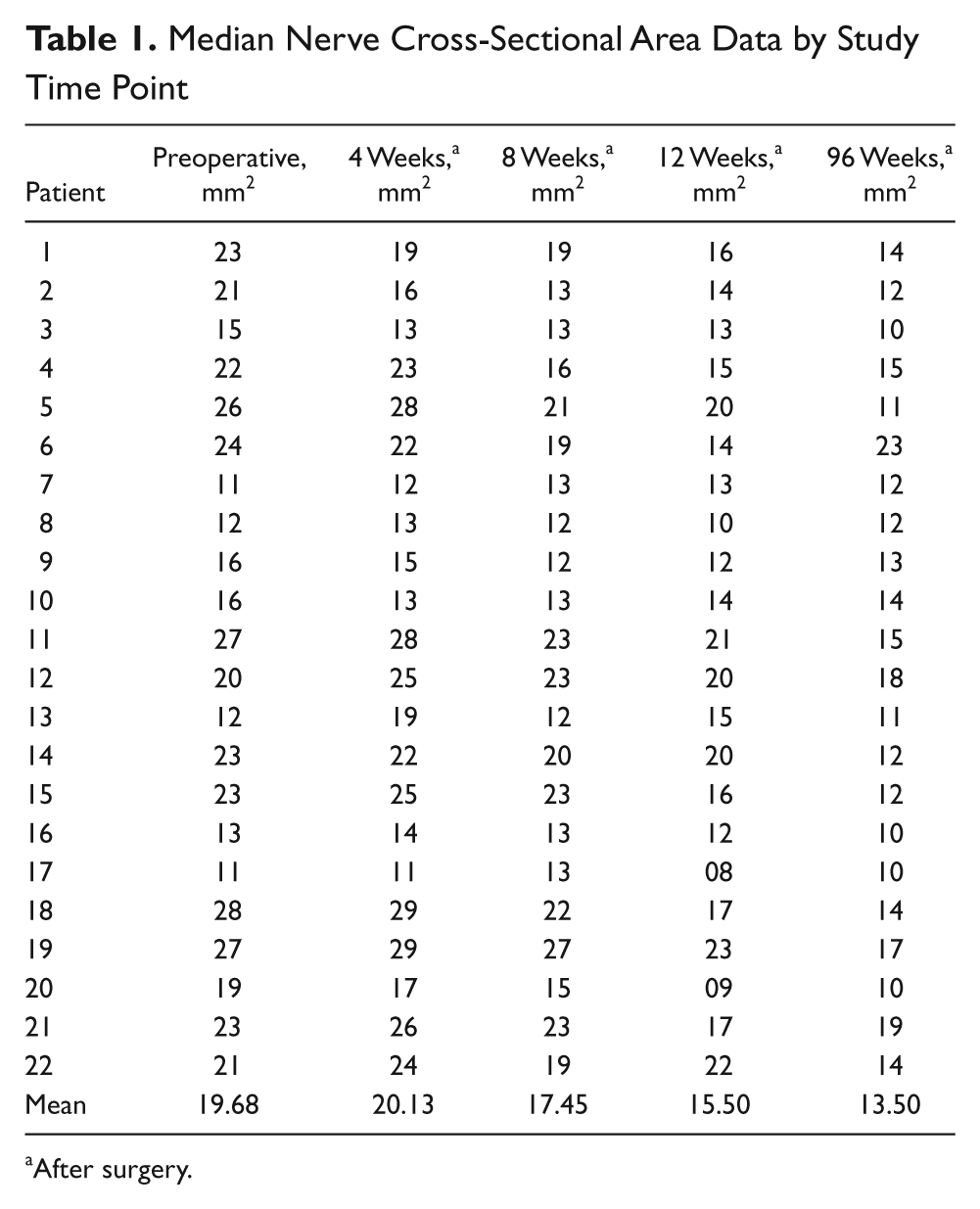
After surgery.

Cross-sectional area of a normal (asymptomatic) median nerve measuring 7 mm2, at the proximal level. ESC, scaphoid; GC, Guyon canal; Nervo mediano, median nerve; PIS, pisiform; T, tendons; TFRC, flexor retinaculum of the hand.
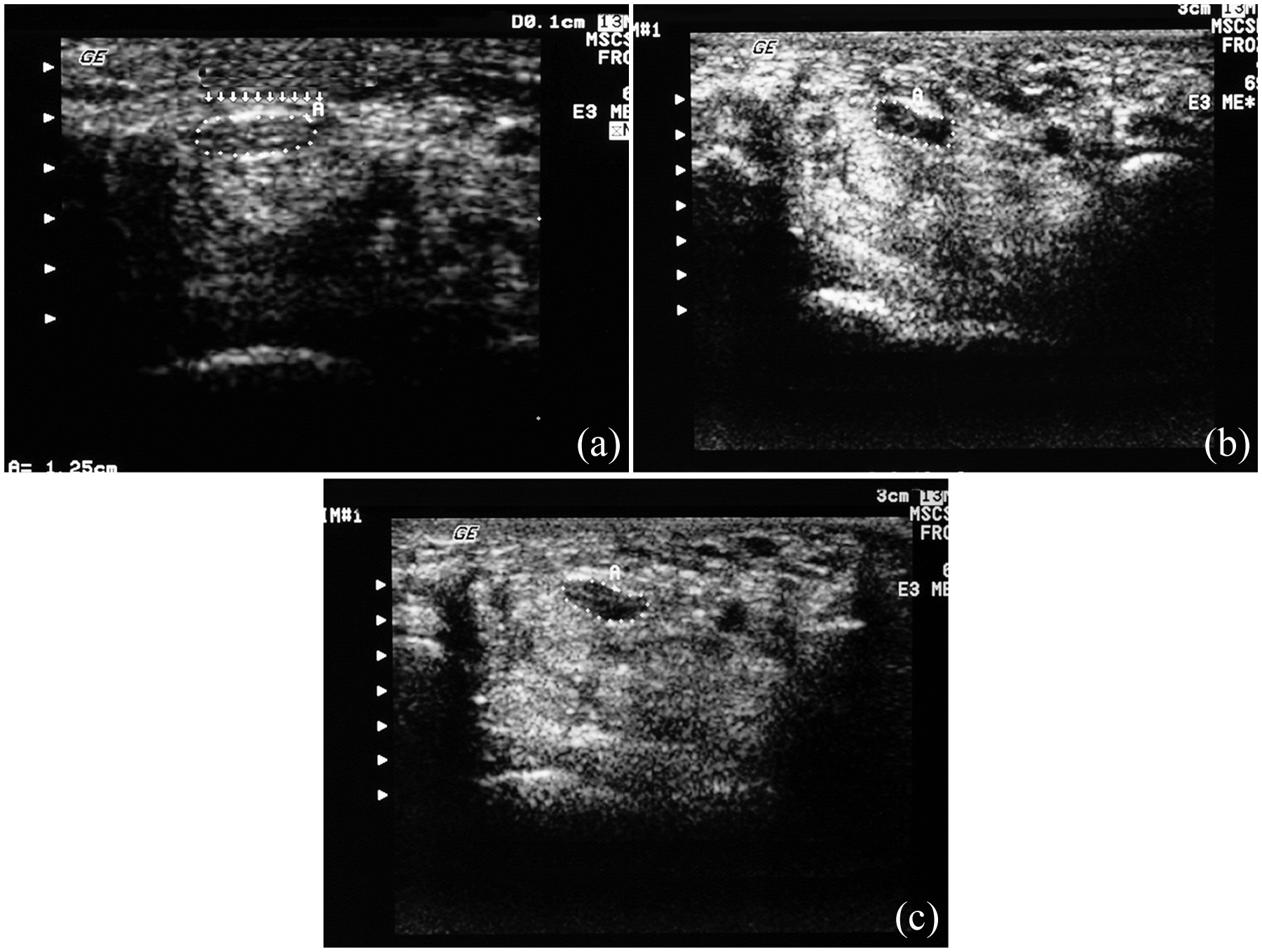
(a) Preoperative ultrasonography on patient 15. Cross-sectional area of the median nerve = 23 mm2 (dotted area). Transverse carpal ligament (arrows and A). (b) Ultrasonography on patient 15 at 4 weeks after surgery. Cross-sectional area of the median nerve = 25 mm2 (dotted area). Transverse carpal ligament (A). (c) Ultrasonography on patient 15 at 96 weeks after surgery. Cross-sectional area of the median nerve = 12 mm2 (dotted area). Transverse carpal ligament (A).
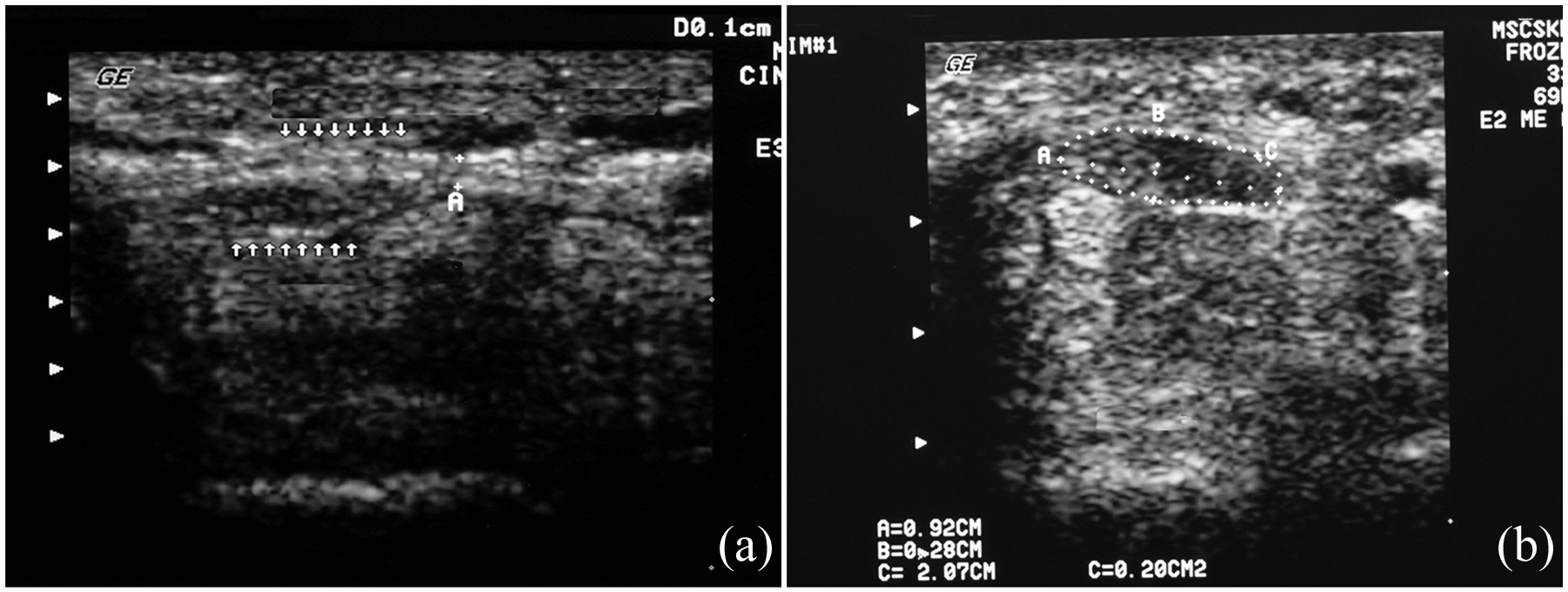
(a) Preoperative ultrasonography on patient 3. Cross-sectional area of the median nerve = 15 mm2 (arrows). Transverse carpal ligament (A). (b) Ultrasonography on patient 3 at 96 weeks after surgery. Cross-sectional area of the median nerve = 10 mm2 (dotted area A, B, C).
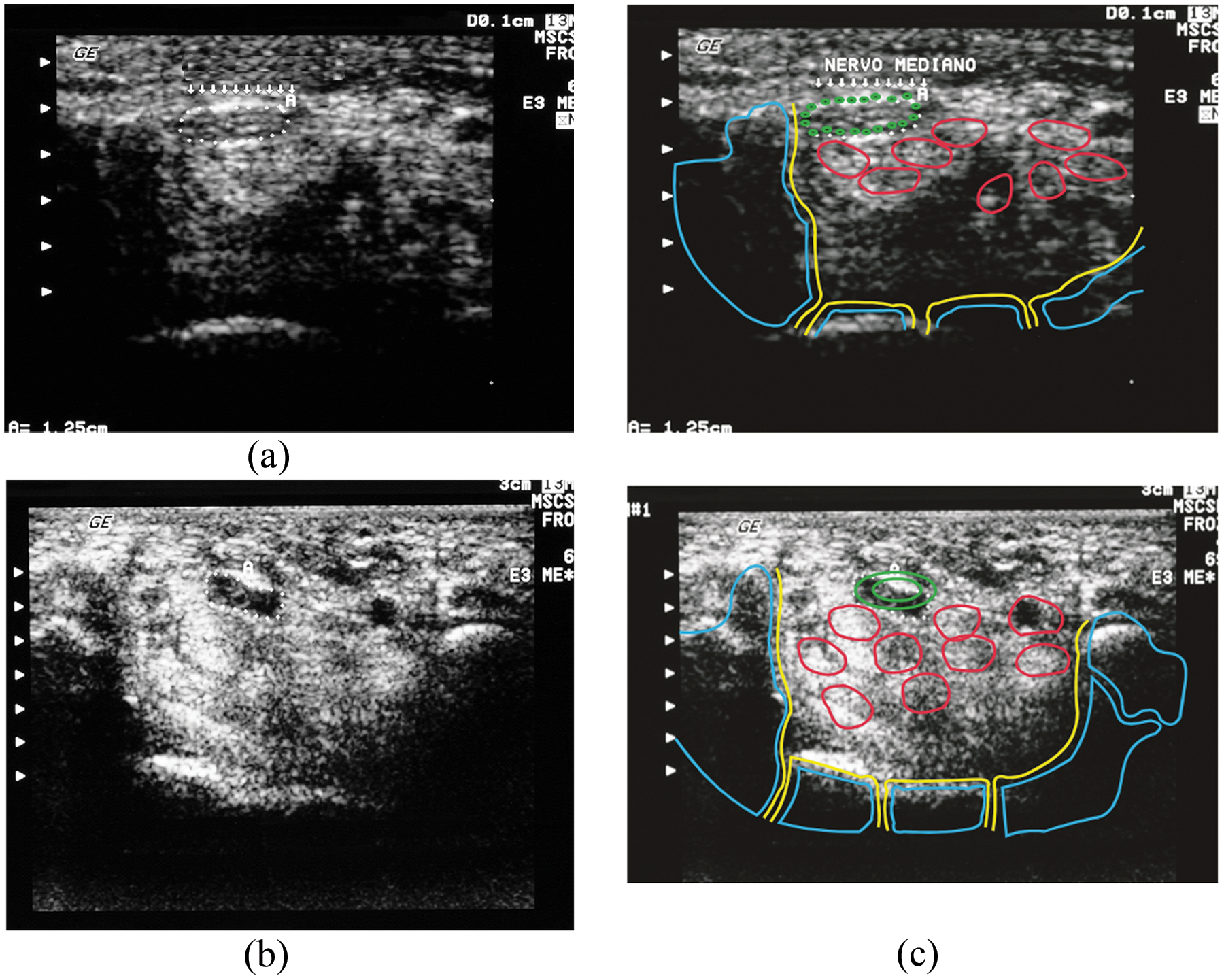
(a) Preoperative ultrasonography on patient 20. Cross-sectional area of the median nerve = 19 mm2 (dotted arrows). Transverse carpal ligament (arrows and A). (b) Ultrasonography on patient 20 at 4 weeks after surgery. Cross-sectional area of the median nerve = 17 mm2 (dotted area). (c) Graphic representation of (a) and (b), patient 20. Median nerve, green; tendons, red; scaphoid, blue, left; pisiform, blue, right.
At 4 weeks postintervention, 13 examinations showed an increase in the median nerve area compared with before surgery, likely consistent with edema. At 12 weeks after surgery, all patients exhibited a linear hypoechoic structure at the level of the transverse carpal ligament, consistent with fibrosis. This finding, along with the lack of identification of the transverse carpal ligament, was confirmatory of successful ligament release.
Of the 18 study patients, 14 had a satisfactory outcome with complete relief of symptoms and restitution of the motor strength no later than 8 weeks after intervention. Three patients failed to reach the expected outcome at 96 weeks after surgery. One patient had dystrophy of the hand as a surgical complication. Four patients complained of pain in the surgical scar early postintervention, but this symptom subsequently resolved in all four patients.
Discussion
Our results demonstrate that 4 weeks after surgery, an increase in the cross-sectional area of the median nerve can be expected. However, in the subsequent examinations (8, 12, and 96 weeks), there was a decrease in the cross-sectional area of the median nerve. The increase in the median nerve cross-sectional area at 4 weeks after surgery is likely secondary to edema resulting from postligament release and surgical intervention. In the following weeks, there was a slow resolution of this edema and initial fibrosis. This was reflected by a decrease of the cross-sectional area of the median nerve.
It has been suggested that patients with a cross-sectional area of the median nerve greater than 10 mm2 prior to surgery are more likely to be diagnosed with carpal tunnel syndrome.5,7,9,11–13,16 Duncan and colleagues 7 have shown that patients with carpal tunnel syndrome have an increased cross-sectional area of the median nerve (mean, 13 mm2) when compared with asymptomatic controls (mean, 7 mm2). All patients included in our study had a cross-sectional area of the median nerve greater than 10 mm2 (mean, 19.7 mm2). Patients with a mean cross-sectional area from 11 to 19 mm2 before surgery reached the cutoff of 10 mm2 after surgery. Although the diagnosis of carpal tunnel syndrome is basically clinical, it is crucial that the physicians be aware that a 10-mm2 parameter for the median nerve cross-sectional area by ultrasonography is only valid before open intervention.16,17 Our study showed no association between the cross-sectional area of the median nerve after surgery and clinical symptoms, contrary to what is described before intervention, in which there is a strong correlation between the median nerve area and patients’ symptoms.
Our population demonstrated a higher mean cross-sectional area of the median nerve compared with other previous studies.5,7,11 We assume this difference is related to the tertiary nature of our institution. Patients who attend our clinics typically have been under conservative treatment for many months before intervention.
The present study does have some limitations. First, the sample size is relatively small because patients were recruited from a single institution over a limited time period. Second, this may contribute to a selection bias because our institution is a reference center and patients were referred to ultrasonography by an orthopedic surgeon, possibly indicating a more advanced state of the disease. Finally, the interobserver agreement between radiologists was not assessed.
In summary, these data suggest no association between clinical symptoms and the median nerve cross-sectional area after ligament division. Following median nerve intervention, the cross-sectional area tends to increase at 4 weeks, likely due to edema, and then progressively decreases in size in follow-up examinations over a 96-week period. Compared with the nerve area before intervention, the most pronounced change in the median nerve area is seen at 12 weeks.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.