
Abstract
The usefulness of endoscopic ultrasonography (EUS) in patients who have gastric wall thickening in computed tomography (CT) is not clear. All patients referred for EUS due to thickened gastric folds on CT were included in this study. Esophagogastroduodenoscopy (EGD) followed by EUS was performed on all patients. Twenty-eight patients were enrolled in the study. The mean ± SD age was 50.8 ± 15.9 years, and 60.7% were male. Most patients (78.6%) had symptoms, and 10 patients (35.7%) were ultimately diagnosed with a gastric neoplasm. In all patients with a normal EGD (11 patients), the EUS was normal. Accuracy, specificity, sensitivity, positive predictive value, and negative predictive value of EUS for detecting a lesion in thickened wall stomach on CT were 89.3%, 88.8%, 90.0%, 81.8%, and 94.1%, respectively. In patients with a thickened gastric wall by CT, upper gastrointestinal endoscopy should be done before endoscopic ultrasonography, with ultrasonography reserved for those patients with an abnormal EGD. Endoscopic ultrasonography has good sensitivity for lesion detection in cases with an abnormal endoscopy, and the presence of gastric symptoms increases the likelihood of abnormal EUS.
Among various disorders that cause giant gastric folds, the most important are gastric lymphoma and scirrhous carcinoma.1–6 From the clinical point of view, establishment of a correct diagnosis of these disorders is important. However, making the diagnosis by computed tomography (CT) or upper gastrointestinal endoscopy (esophagogastroduodenoscopy or EGD), even including biopsy, is not always a simple task. Endoscopic ultrasonography (EUS) has been recently introduced as a useful method aiding in the diagnosis of giant gastric folds.2–6 Results of EUS in asymptomatic patients with a thickened stomach wall on computed tomography have not been well described previously and therefore warrant further investigation. The purpose of this study was to evaluate the usefulness of EUS in a consecutive series of patients with thickened gastric wall on CT.
Methods
During the two-year period from May 2008 to May 2010, a prospective study was conducted in a university referral center in Shariati Hospital of Tehran University of Medical Sciences, where approximately 1500 EUS procedures are performed annually. The study was approved by the institutional review board of the university, and written informed consent was obtained according to the university guidelines.
Patients were eligible if they were referred for EUS because of a CT performed with oral and intravenous contrast media showing thickening of the gastric wall. Those with a previous history of gastric malignancy were excluded. Patients were questioned and examined by the researchers, and the following data were recorded: age; sex; presence of generalized abdominal symptoms; presence of any more urgent symptoms such as weight loss, anorexia, anemia, hematemesis, and melena; the indication for EUS; and the results of previous imaging studies.
A single researcher blinded to the results of previous investigations performed the EGD examination. Endoscopy was performed using a standard forward-viewing video endoscope (Olympus GIF-130, Olympus America, Melville, New York). During EGD, endoscopic mucosal abnormalities and gastric distensibility were evaluated. If a mucosal lesion was seen, biopsy was performed for histopathology studies. EGD was followed by radial scanning EUS at 7.5 MHz (EG-363 DUR; Pentax Optical Co Ltd, Tokyo, Japan). The EUS examination was performed while the patient was in the left lateral decubitus position under conscious sedation. If EUS fine-needle aspiration (FNA) was required for a visualized gastric intramural lesion, it was performed immediately (Pentax FG-38UX, connected to Hitachi-E5500 ultrasound equipment [Hitachi Medical Corporation, Twinsburg, Ohio]). For clear visualization of the gastric wall and assessment of the wall layers without interference by intraluminal gas, the stomach cavity was filled with water. By EUS examination, the gastric wall was considered normal if a thorough evaluation of the wall in all regions of the stomach showed a thickness of less than or equal to 5–6 mm and no disorganization of the five-layer wall.
Eight months after the procedure, all subjects (or a family member) were contacted by phone and a standardized questionnaire was administered. The questionnaire addressed the patient’s general health status and whether any further investigation, including sonography, CT, endoscopy, or surgery, had been performed during the follow-up period. If pathology reports were available, these results were also recorded. All follow-up calls were made by a single researcher who was blinded to the EGD and EUS findings.
The primary outcome was an abnormal finding by EUS. The clinical follow-up was used to evaluate the performance characteristics of upper endoscopy and EUS. Chi-square statistics were used in contingency table analysis, and the sensitivity, specificity, positive predictive value, and negative predictive value were calculated. A P value of <.05 was used to define statistical significance. Univariable and multivariable logistic regressions were performed using Stata 8.0 (StataCorp, College Station, Texas).
Results
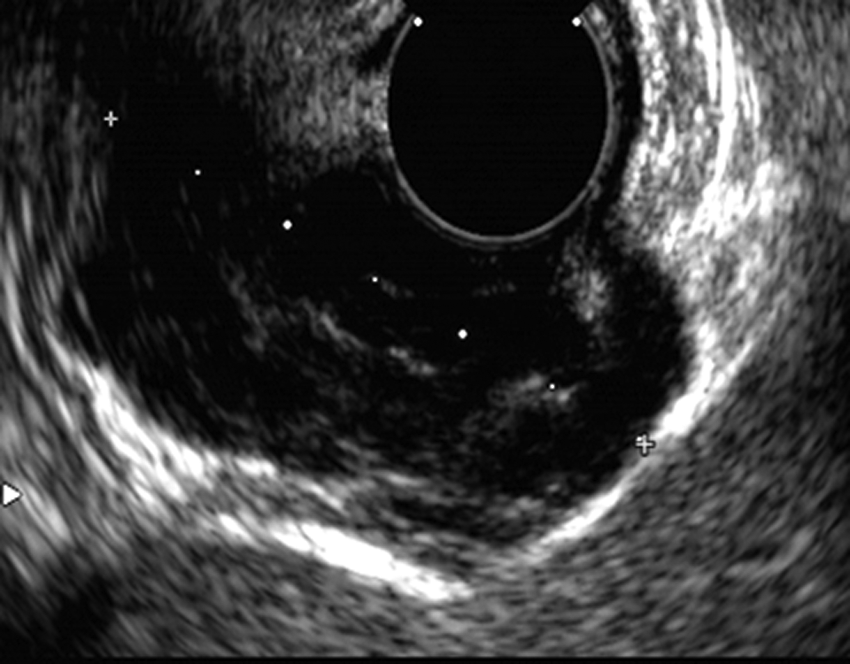
During the study period, 28 patients were referred for EGD and EUS due to thickened gastric wall seen on CT. All CT scans were performed with oral and intravenous contrast media. The imaging findings of the patients are listed in Table 1. All 28 patients completed the eight-month follow-up period. The mean ± SD age was 50.8 ± 15.9 years. The prevalence of a thickened gastric wall was higher in men than in women (60.7% vs 39.3%). Of the 28 patients, 22 (78.6%) had symptoms attributable to the gastrointestinal tract. Eleven patients (39.3%) had a normal EGD, and 18 patients (64.3%) had a normal EUS (Figure 1). Ten patients (35.7%) ultimately were diagnosed with gastric neoplasm; five were found to have adenocarcinoma (Figure 2), three had lymphoma (Figure 3), and two had a gastrointestinal stromal tumor (GIST; Figure 4). Prevalence of a neoplasm based on a thickened gastric wall by CT was 36%; prevalence based on an abnormal EGD was 59% and based on an abnormal EUS was 90%.
Imaging Findings of Patients With Gastric Wall Thickness Seen by Computed Tomography (CT)
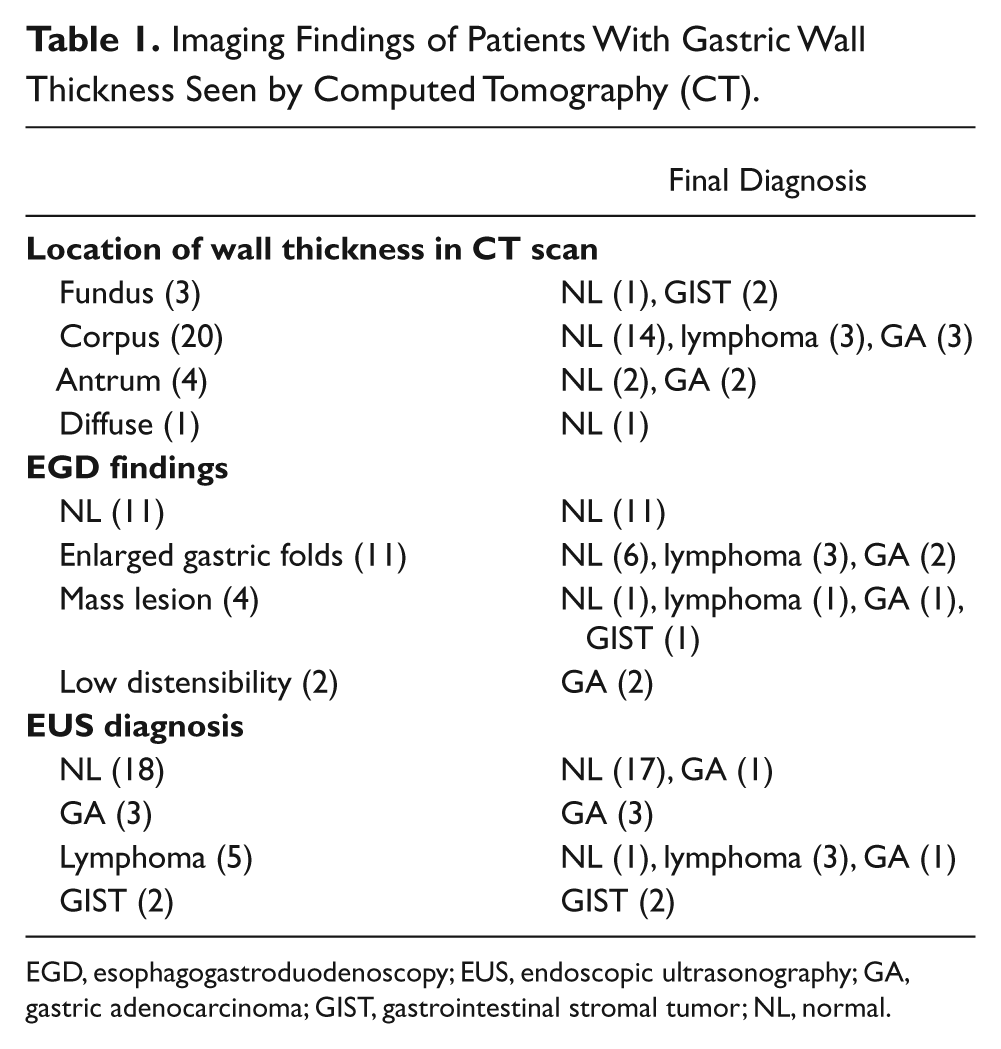
EGD, esophagogastroduodenoscopy; EUS, endoscopic ultrasonography; GA, gastric adenocarcinoma; GIST, gastrointestinal stromal tumor; NL, normal.
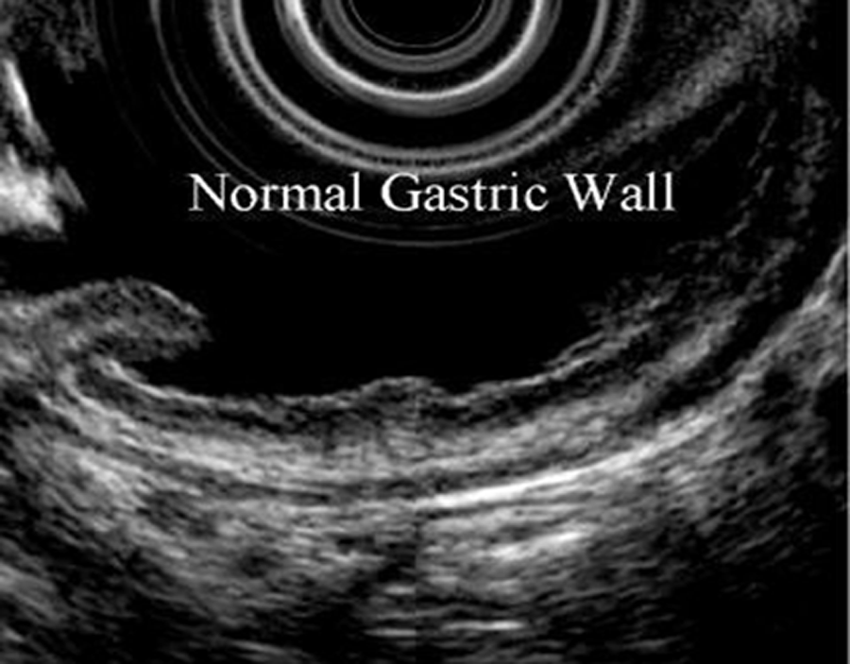
Endoscopic ultrasonography of the normal gastric wall.
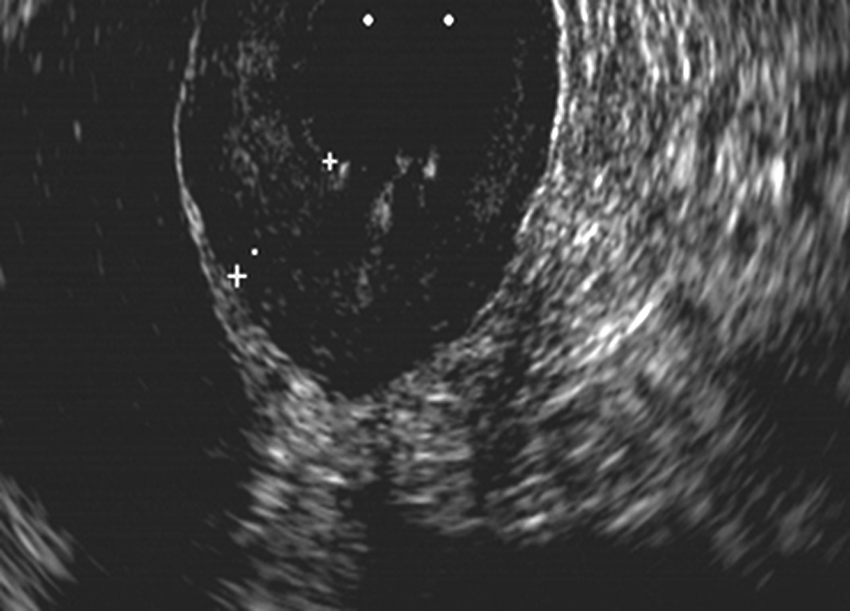
Endoscopic ultrasonography in a patient with gastric adenocarcinoma. Note the hypoechoic wall thickness originating from the epithelial layer of gastric mucosa.

Endoscopic ultrasonography in a patient with gastric lymphoma. Note the heterogeneous wall thickness originating from lamina propria layer of the gastric mucosa and the degree of similarity to the gastric adenocarcinoma shown in Figure 2.
Endoscopic ultrasonography in a patient with a gastrointestinal stromal tumor (GIST), originating from the muscularis propria layer.
Age and sex were not correlated with a malignant outcome (P = .6 and .9, respectively). The presence of dyspepsia and constitutional symptoms (including weight loss and anorexia) were correlated with the presence of a gastric abnormality. The odds ratio for having a malignancy for patients with abdominal or constitutional symptoms was 2.0 (95% confidence interval [CI], 1.3–3.0).
All patients with a normal EGD (11 patients) also had a normal EUS. Eighteen patients total had a normal EUS, with one false-negative study. When the EGD was abnormal (17 patients, 7 with normal follow-up), the EUS was abnormal in only 10 cases (58.8%) with one false-positive examination. For 10 patients with an abnormal EGD characterized by a thickened stomach wall or a subepithelial lesion, 4 (40%) had a normal EUS and an uneventful follow-up. Four patients had antral thickness noted on CT; two of these patients had gastric adenocarcinoma, and two were normal. Three patients had proximal gastric wall thickness by CT; two of these patients had GIST, and one was normal. Two patients with low distensibility seen on EGD had adenocarcinoma found in follow-up.
The overall accuracy, specificity, sensitivity, positive predictive value, and negative predictive value of EUS for detecting a lesion in patients with a thickened wall stomach on CT were 89.3%, 88.8%, 90.0%, 81.8%, and 94.1%, respectively. For comparison, the sensitivity and negative predictive value of EGD were 100%, but the positive predictive value was only 58.8%, and the specificity was 61.1%.
Discussion
The results of this prospective study showed that in most patients with abnormal gastric wall thickness on CT, the EGD examination also will be abnormal. Although studies have described the role of endoscopic ultrasonography in giant gastric folds or the role of EUS for evaluation of previously diagnosed gastric subepithelial masses and gastric lymphoma,2–10 there are no similar studies for the role of EUS in thickened wall stomach by CT with the exception of that by Lam et al. 11 Similar to the data in this article, Lam et al 11 showed that normal upper gastrointestinal endoscopy is strongly associated with a normal EUS. They further found that the presence of symptoms could not predict or increase the likelihood of an abnormal EUS; however, the present study showed that most patients with an abnormal EUS have associated abdominal or constitutional symptoms. The correlation of these symptoms with the findings of EUS/EGD emphasizes the importance of thorough history taking in these patients.
In the present study, all patients who had a normal EGD also had a normal EUS. In addition, all cases in this series with an abnormal EUS had an abnormal EGD. Another important finding during EGD was the distensibility of the stomach cavity. Two patients who had low gastric distensibility were found to have diffuse-type gastric adenocarcinoma without a localized mass lesion. These findings demonstrate the importance of doing proper EGD before EUS.
The present data strongly suggest that the CT finding of thick gastric folds is an appropriate indication for EGD, as 10 of these patients (35.7%) were diagnosed with gastric neoplasms. In addition, all lesions but one detected during EGD were detected by endoscopic ultrasonography. This finding supports the clinical practice that EUS can be the next diagnostic strategy following abnormal EGD. Moreover, with EUS, it is possible to do sonographically guided biopsy sampling for subepithelial lesions that have normal-looking mucosa. Any tumor spread and the presence of lymph node involvement can then be evaluated at the same time.
A possible limitation of EUS, as shown by the data in Table 1, is the misdiagnosis of gastric lymphoma. One patient with the EUS diagnosis of lymphoma was found to have adenocarcinoma, whereas the other one was normal. Lymphoma can originate from the lamina propria, the second gastric wall layer just adjacent to epithelial layer, or the submucosal layers. As these are also the layers in which early stage gastric adenocarcinoma may be found, differentiation of these two abnormalities by imaging may be difficult. Biopsy is the only means for reliably differentiating these two entities. The second patient, who was diagnosed by EUS with mucosa-associated lymphoid tissue (MALT) lymphoma but determined during follow-up to be normal, had mild wall thickness in the lamina propria also. This wall thickness could have been secondary to a local inflammatory process such as Helicobacter pylori infection, which was found to be present in this case. This patient was normal after two years of follow-up by repeat EGD and EUS examinations. A more significant limitation of this study is the small number of patients. Despite the fact that approximately 1500 EUS procedures are performed annually at our institution, only 28 patients were found who met study entry criteria. Expanding this study, possibly as a multi-institutional one, to include more cases would hopefully further clarify the role of EUS in this setting.
In summary, when CT shows gastric wall thickness: (a) if upper endoscopy is normal, EUS will be normal too and may not be necessary. (b) If upper endoscopy is abnormal, EUS is likely to be abnormal in nearly 60% of cases, and (c) the presence of gastric-related symptoms appears to increase the likelihood of an abnormal EUS. We conclude that in patients with thickened gastric wall on CT, doing upper gastrointestinal endoscopy before endoscopic ultrasonography is a reasonable course of action. Endoscopic ultrasonography appears to be helpful in further differentiating cases in which the EGD examination is abnormal.
Footnotes
Acknowledgements
We thank Dr. Shahin Merat and Nima Zare for their help in revising and editing this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received financial support for the research, authorship, and/or publication of this article from the Digestive Disease Research Center, Tehran University of Medical Sciences.