
Abstract
A retroaortic left renal vein (RLRV) is an uncommon condition in which the left renal vein passes posterior to the abdominal aorta and anterior to the vertebrae. Retroaortic left renal vein may lead to left renal vein hypertension syndrome, also known as the nutcracker syndrome, a condition in which extrinsic compression of the left renal vein causes hypertension within the vessel. Retroaortic left renal vein and nutcracker syndrome are vascular anomalies considered to be of clinical importance, particularly during surgical procedures involving the renal vasculature directly or, in many cases, the abdominal aorta.
The fetal development of the left renal vein coincides with the development of the inferior vena cava (IVC) as the left renal vein arises from the left kidney to eventually drain into the IVC. The IVC itself is formed from three pairs of veins, including the posterior cardinal veins, the subcardinal veins, and the supracardinal veins. The subcardinal and supracardinal veins anastamose to form a network of veins that course along the ventral and dorsal aspect of the abdominal aorta. 1 Typically, the ventral portion of the network continues as the dorsal network deteriorates, causing the ventral network to form the left renal vein coursing anterior to the abdominal aorta (Figure 1). If the dorsal network continues, then the ventral portion deteriorates and the left renal vein passes posterior to the abdominal aorta (Figures 2 and 3). When the left renal vein courses posterior to the aorta, it is referred to as a retroaortic left renal vein (RLRV). Occasionally, there may be a duplication of the left renal vein in which the vessel passes both anteriorly and posteriorly to the aorta to drain into the IVC.
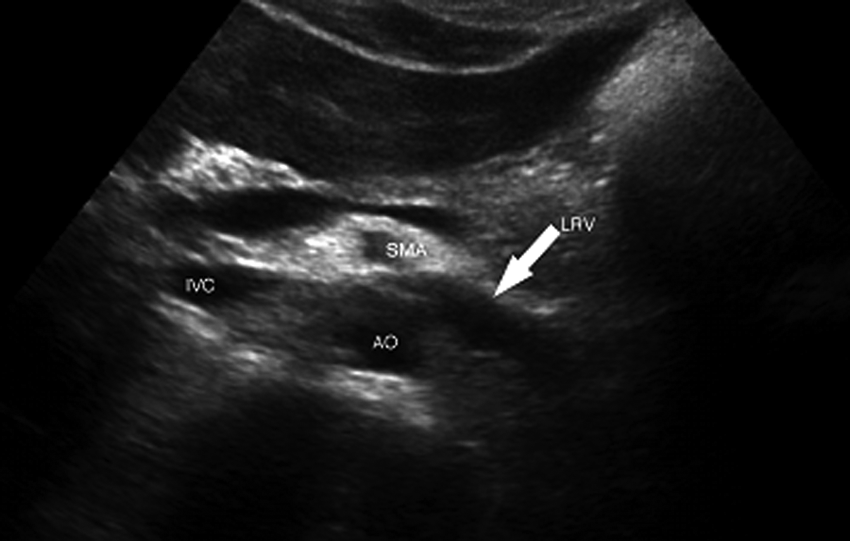
Transverse gray-scale image of the normal course of the left renal vein (arrow) anterior to the abdominal aorta (AO) and posterior to the superior mesenteric artery (SMA). IVC, inferior vena cava; LRV, left renal vein.

Transverse gray-scale image of the left renal vein (arrows) coursing posterior to the abdominal aorta (AO) and anterior to the vertebrae, draining into the inferior vena cava (IVC).
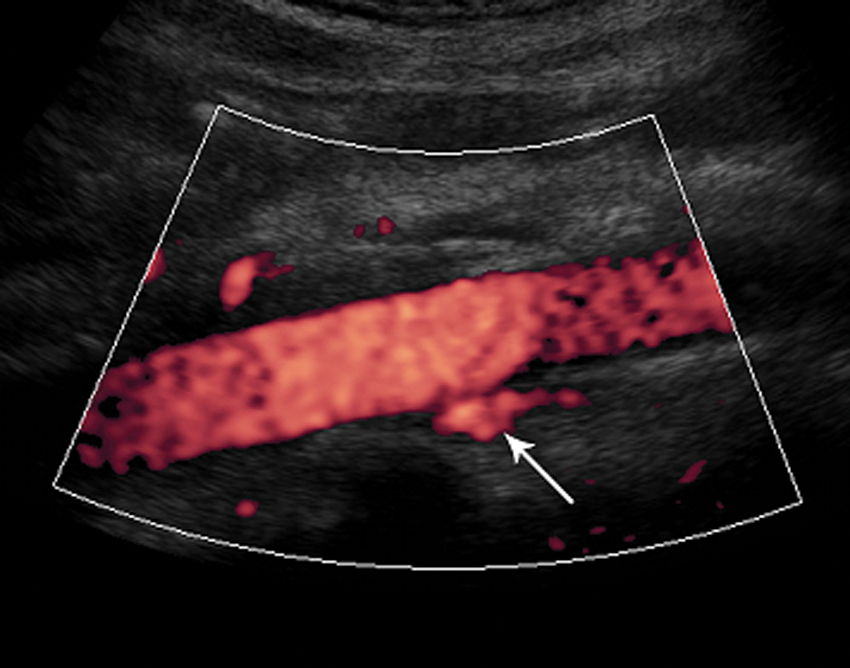
Sagittal power Doppler image showing the location of the left renal vein (arrow) posterior to the aorta.
Left renal vein hypertension syndrome, also known as the nutcracker syndrome, originally described by De Schepper 2 and noted by Grant as “the left renal vein as it lies between the aorta and the superior mesenteric artery[,] resembles a nut between the jaws of a nutcracker.” 3 The nutcracker syndrome is now more generally defined as any compression of the left renal vein leading to hypertension within the vessel. The two most common forms of the nutcracker syndrome include the anterior nutcracker phenomenon, De Schepper’s and Grant’s original description, and the posterior nutcracker phenomenon resulting from RLRV. The anterior nutcracker syndrome describes left renal vein hypertension due to compression of the vein between the superior mesenteric artery and the abdominal aorta. 4 Posterior nutcracker syndrome refers to hypertension of the left renal vein due to compression of the vein between the abdominal aorta and the vertebral column of the spine.5,6
Clinically, a patient with nutcracker syndrome may present with left flank and/or abdominal pain and hematuria (macroscopic or microscopic). The key symptom in detecting posterior nutcracker syndrome is hematuria. In females, left renal vein hypertension may also present as pelvic congestion syndrome, characterized by lower abdominal pain, dysmenorrhea, emotional distress, or varices of the lower limbs. In males, compression of the left renal vein frequently causes reflux between the left renal and gonadal veins resulting in varices of the lower limbs. 7
The etiology of nutcracker syndrome has not yet been medically proven. However, several factors may be related to the anterior form of the disorder, including inadequate stretching of the left renal vein or abnormal branching of the superior mesenteric artery (SMA). 3 Normally, the SMA originates from the aorta at a 90-degree angle and travels about 4 to 5 mm before taking a caudal descent, which typically avoids compression of the left renal vein. However, in the case of the nutcracker syndrome, the SMA branches from the aorta at a more acute angle, immediately descending caudal to the vessel, which increases the risk of compression of the vein.
Several methods can be used to diagnose compression of the left renal vein. It is important to know and remember that because of the weight of the bowel stretching the SMA caudad, compression of the left renal vein is increased if the patient is in a standing position. Therefore, compression of the vein may not be accurately diagnosed with examinations that require the patient to be in an upright or decubitus position. Duplex ultrasound is a useful method that is able to demonstrate compression of the left renal vein using both color/power and spectral Doppler 8 (Figure 4). Duplex scanning is able to detect anomalies of the left renal vein, including stenosis, flow abnormalities, and collateral pathways. 9 Evaluation of a stenosis would include the comparison between the anteroposterior diameter of the left renal vein to the left of the aorta just before draining into the IVC, at the level of the stenosis, and just beyond the hilum of the left kidney to the right of the aorta. Flow abnormalities would be evaluated by measuring the peak systolic velocity at the level of the stenosis and near the hilum of the left kidney. The main collateral pathway of the left renal vein is the gonadal vein, which should be carefully evaluated for flow characteristics and flow direction and measured. 8 The SMA should also be evaluated by duplex sonography to determine its location, angle, and the distance between the SMA and the aorta at the level of the left renal vein. Two recent reviews have shown the sensitivity of duplex sonography for detection of the nutcracker syndrome to be 70% to 90% and the specificity virtually 100%.10,11
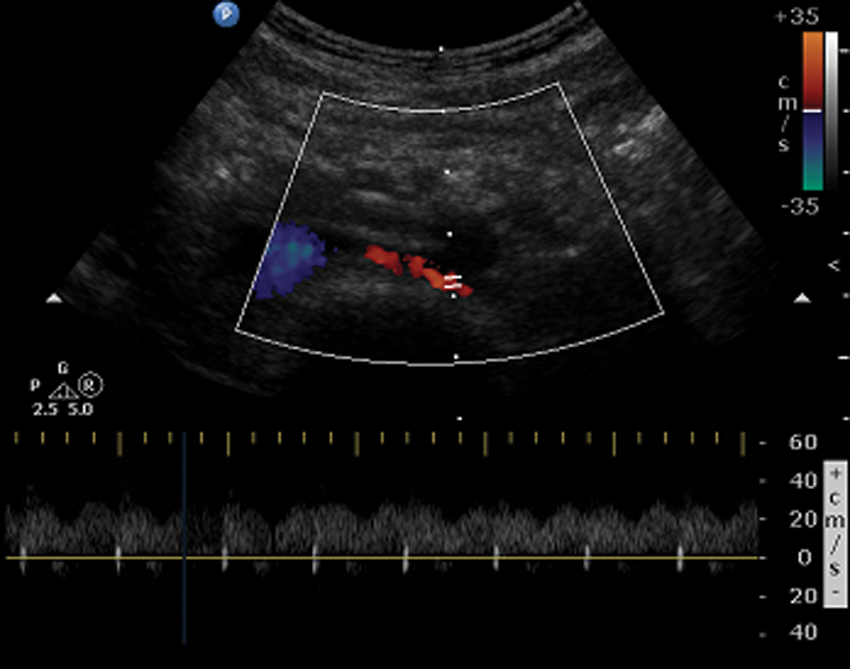
Transverse duplex ultrasound image and spectral Doppler display showing normal flow hemodynamics in the left renal vein.
Computed tomography angiography (CTA) and magnetic resonance angiography (MRA) are also useful methods in detecting compression of the left renal vein, as they both show the vein relatively clearly and indicate its relation to other structures and organs surrounding it. More invasively, phlebography and direct renal vein pressure gradient measurements can also be used to evaluate compression of the left renal vein.
Treatment of the more common anterior nutcracker syndrome depends on the severity of the disorder. Patients may be asymptomatic, in which case no treatment is recommended. Patients with severe or ongoing symptoms may undergo various surgical procedures to reduce compression, including left renal vein transposition, renal autotransplantation, or stenting of the left renal vein.9–11 Transposition of the left renal vein involves dividing the left renal vein as it intersects the IVC and repositioning the vein to a lower level than its initial junction with the IVC. 12 Renal autotransplantation involves the anastamosis of the left renal vein and artery to the common iliac vein and artery, removing the left kidney from its original position and transplanting it to another location within the left pelvic region. 13 Endovascular stenting of the left renal vein, a less invasive procedure, may be used to reduce compression of the vein and decrease the pressure gradient within the vessel to eliminate symptoms. 14 Similar techniques can be used to treat the less common posterior nutcracker syndrome as well.
Besides the symptomatic presentation of the nutcracker syndrome, renal vein anomalies can significantly affect the outcome of major retroperitoneal surgery. Severe hemorrhage and/or renal failure can result in failure to detect renal vein anomalies prior to surgical procedures. 7 The left renal vein typically is longer than the right renal vein because it travels a longer distance to drain into the IVC, which is anatomically located on the right side of the aorta (Figure 5). Because of the longer length of the left renal, vein surgeons prefer the left over the right renal vein with renal transplantation, and thus it is crucial to know the anatomic course of the left renal vein and whether it passes anterior to the aorta or whether it is retroaortic.
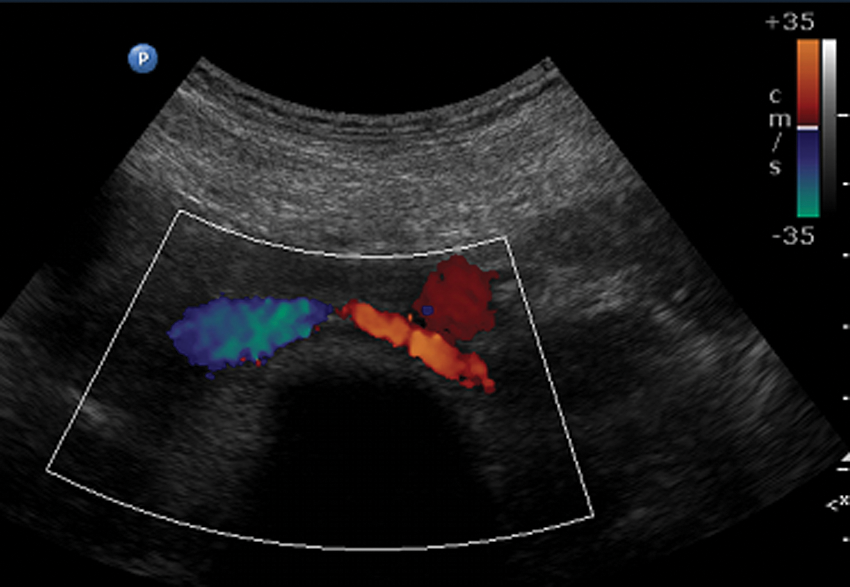
Transverse color Doppler image of the left renal vein passing between the abdominal aorta and the vertebrae, entering the inferior vena cava.
Conclusion
The left renal vein generally courses anterior to the abdominal aorta. There are instances when the left renal vein takes a different path, traveling posterior to the aorta. Retroaortic left renal vein is an anomaly of the renal vein that may cause damage to the vessel and lead to nutcracker syndrome, which results in venous hypertension. This anomaly is relatively uncommon, and most patients are asymptomatic. It is crucial to identify the course of the left renal vein so that surgical procedures of the vessel can be accurately performed. Anomalies of the renal vein are frequently overlooked, but with appropriate testing and imaging, abnormalities can be detected and properly maintained.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.