
Abstract
Aneurysms of the major veins are rare, and those involving the inferior vena cava (IVC) are extremely rare. The etiology of IVC aneurysms remains unknown, and they can have variable presentation. Although many aneurysms are found incidentally, others are diagnosed after complications develop. Thrombosis is a frequent presentation, and serious sequelae, such as lethal pulmonary embolism and Budd-Chiari syndrome, may result. Therapeutic alternatives range from watchful waiting to surgical management. Development of complications such as rupture has been described and may require surgery. In this article, we report the discovery of an IVC aneurysm in a patient who had chronic renal failure associated with renal hypoperfusion and severe cardiac insufficiency.
Case Report
A man in his late 60s was admitted to the hospital with a history of dyspnea, pain, and bilateral lower extremity swelling. The medical history was significant for chronic renal failure due to gout, treated with a long course of allopurinol. He had no history of a deep venous thrombosis (DVT). A sonogram without Doppler study, performed at another hospital, reported a large right renal cyst. On physical examination, the patient was 173 cm in height and weighed 89.9 kg, with blood pressure of 100/60 mm Hg. He was found to be anemic with hemoglobin of 7.8 g/dL and with raised blood urea nitrogen (50.0 mg/dL) and serum creatinine (2.51 mg/dL). Past medical records were not available. By transthoracic echocardiography, the estimated left ventricular ejection fraction was 29% with severe diastolic dysfunction. Ultrasonography, at our hospital, revealed echogenic kidneys with poor corticomedullary differentiation and small cortical cysts on both sides. Doppler study failed to demonstrate blood flow in the right kidney (Figure 1A), whereas in the left kidney, the blood tree and spectral tracing were depicted (Figure 1B). Incidentally, an anechoic outpouching was detected on the right wall of the inferior vena cava (IVC) at the level of the right renal vein (Figure 2A), showing a characteristic “swirling motion” within it on color Doppler interrogation (Figure 2B). The IVC appeared to terminate at the level of the aneurysm. Although a tiny echogenic line had been seen between the aneurysm and intrahepatic IVC, no Doppler signal was detected between the aneurysm and intrahepatic IVC (Figure 3). On the basis of color Doppler ultrasonography studies, our clinical impression was inferior vena cava aneurysm, so we decided to proceed with further investigation to better delineate the drainage anatomy. To avoid contrast medium nephropathy, we chose computed tomography (CT) without contrast instead of venography. For the same reason, cardiac catheterization to detect coronary atherosclerosis as the cause of heart failure was rejected.
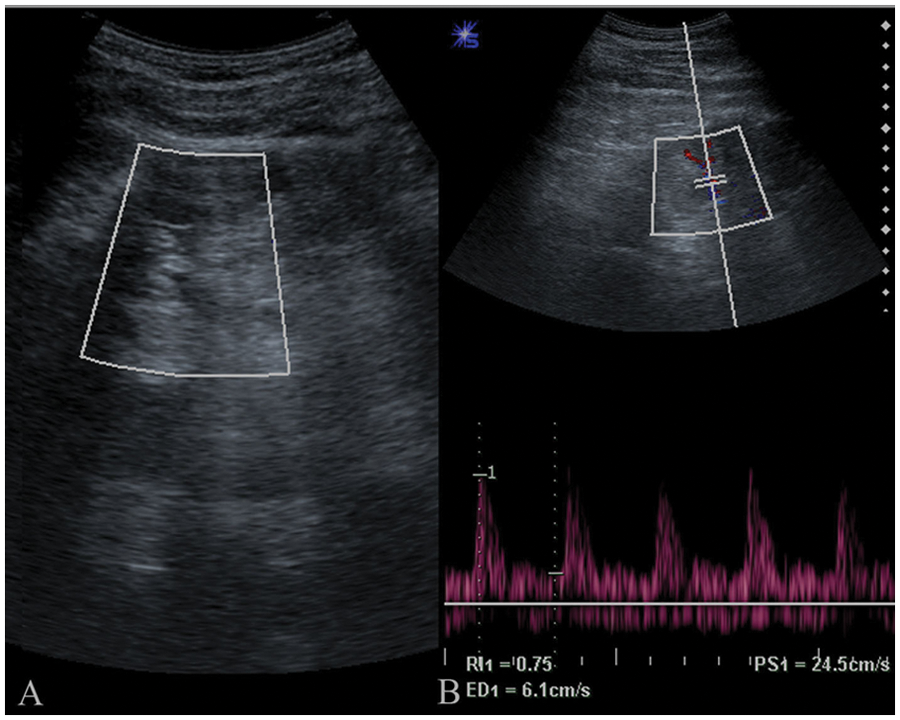
Doppler study of the kidneys. (A) A color Doppler image shows the absence of flow in the right kidney. (B) Duplex image of the left kidney depicts vascular tree and spectral tracing shows typical arterial waveform.
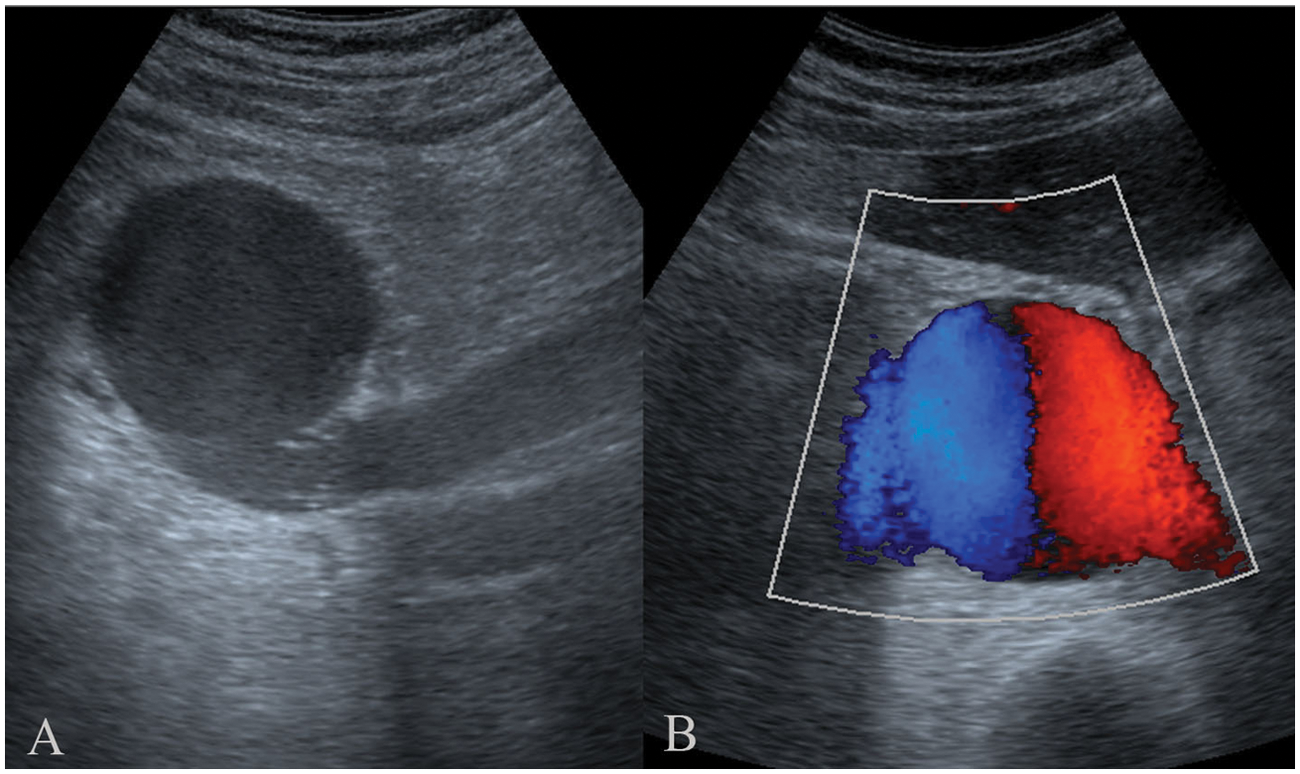
(A) Longitudinal abdominal sonogram along the right infraumbilical region showing a well-defined anechoic lesion communicating with the inferior vena cava. (B) Color Doppler imaging establishing the vascular nature of the anechoic lesion.
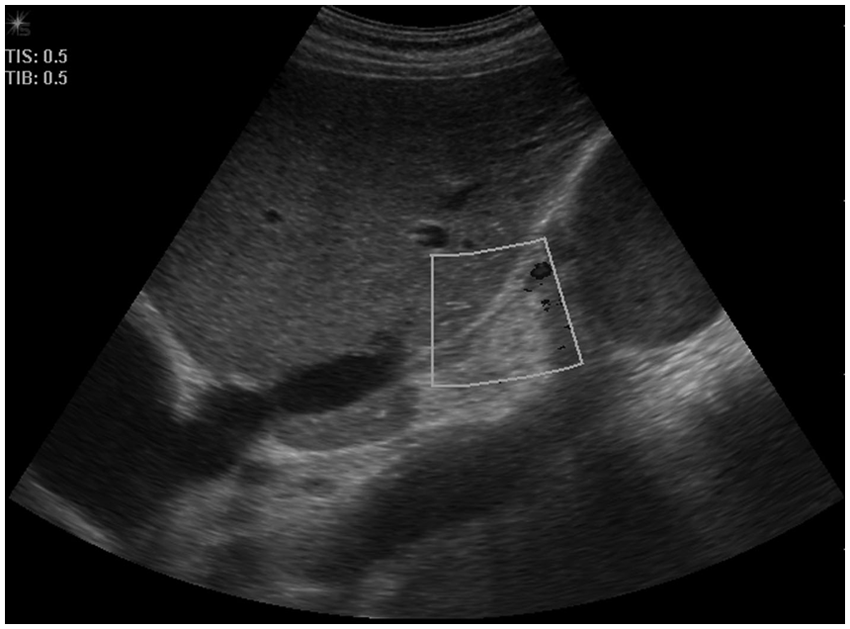
Sonogram showing atretic suprarenal segment of the inferior vena cava (IVC), with color Doppler showing the absence of flow within the IVC. The aneurysm is seen inferior to the atretic segment.
A nonenhanced computed tomography (NECT) examination was performed and showed the IVC aneurysm as a retroperitoneal mass, medial to the right kidney and abutting the lateral wall of the IVC, measuring 5.5 × 5.9 × 6.5 cm (Figure 4). Above the mass, the IVC showed a severely reduced caliber, which returned to its normal dimension in the intrahepatic portion (Figure 5). Multiple collateral vessels were observed surrounding the mass. There was also significant dilation of the azygos vein (Figure 6). There was no suggestion of intraluminal thrombus based on the appearance of both imaging studies.
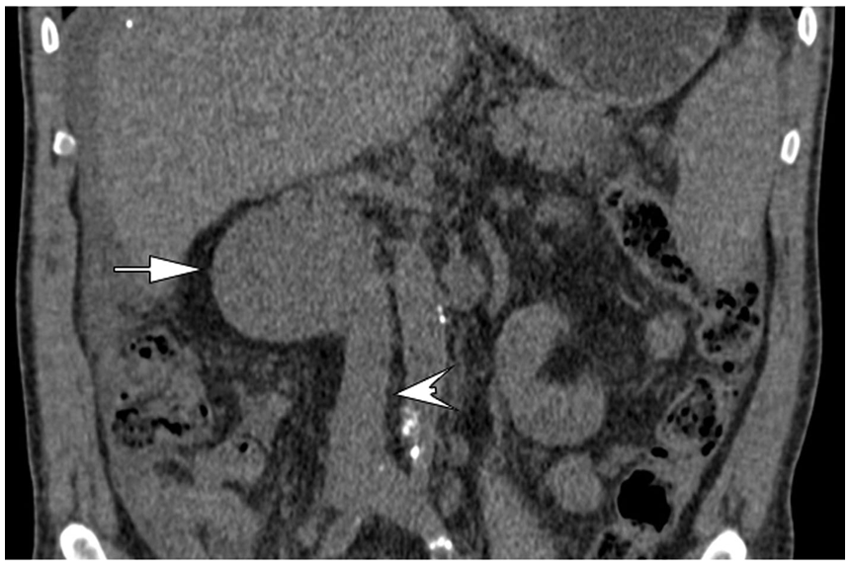
Computed tomography coronal reformation shows the aneurysm as a mass (arrow) abutting the lateral wall of the inferior vena cava (arrowhead).

Nonenhanced computed tomography sagittal refor-mation shows retroperitoneal mass (large white arrow), the inferior vena cava (IVC) with a severe reduced caliber (thin white arrow), and the normal intrahepatic IVC (black arrow).
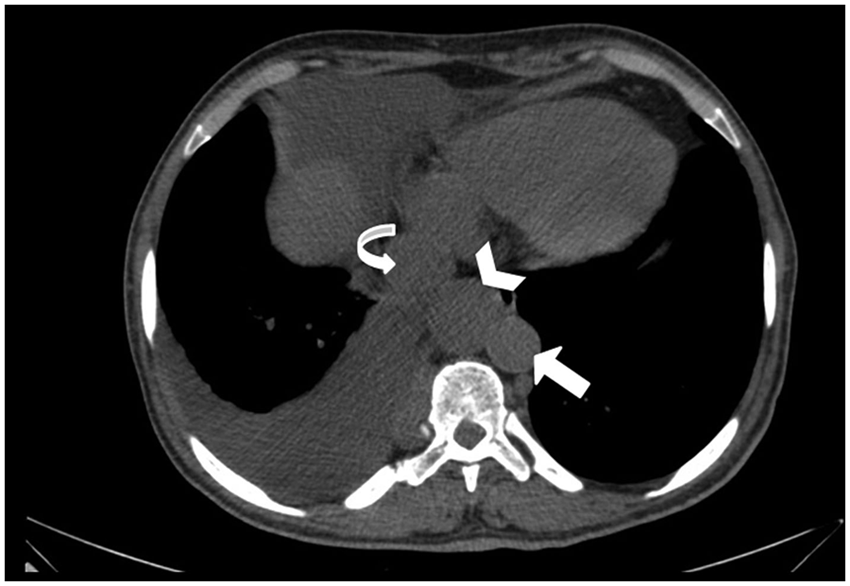
Computed tomography image above the liver and superior to the level of the aneurysm demonstrates the aorta (arrow), the inferior vena cava (curved arrow), and the enlarged azygos vein (arrowhead).
Since venous aneurysms are known to be associated with thrombotic events, oral anticoagulation was started with Coumadin to avoid it. The course during hospitalization was complicated by worsening renal failure and cardiac insufficiency that culminated with the patient’s death from cardiogenic shock.
Discussion
Aneurysms of the inferior vena cava, although rare, should be considered in the differential diagnosis of retroperitoneal masses, and the occurrence of isolated cases is a topic for publication. IVC aneurysms may be saccular or fusiform, with the saccular presentation being slightly more common.1–3 The mode of presentation does not appear to vary with either age or gender. The diagnosis of this lesion is often missed because of its rarity. The great majority are found incidentally, whether in children 4 or in adults. 5
In 1993, Gradman and Steinberg 3 suggested a useful anatomic classification for IVC aneurysms: type I, aneurysms of the suprahepatic IVC without venous obstruction; type II, aneurysm associated with interruption of the IVC above or below the hepatic veins; type III, aneurysms confined to the infrarenal IVC without associated venous anomaly; and type IV, which was described as “miscellaneous,” a left-sided IVC and an aneurysm at the junction of the left internal and external iliac veins. According to this classification system, our case, therefore, would fall into the type II category, which is associated with interruption of the IVC above or below the hepatic veins.
The etiology of venous aneurysms remains unclear, probably due in part to their infrequency. Although the origin of these aneurysms is unknown, it has been suggested that they develop due to a congenital weakness of the vein, in the anastomosis between the embryological venous systems. Concomitance with other congenital cardiovascular abnormalities further supports modifications during embryogenesis. Among the congenital anomalies of the IVC, absence of the infrahepatic segment of the IVC has been reported. 6 In our patient, the associated venous anomaly was infrahepatic IVC stenosis. Indeed, the IVC was interrupted at the infrahepatic level, as evidenced by the absence of flow in this segment of the IVC on Doppler study and severe narrowing on CT. The venous drainage from below the diaphragm in such cases is via the azygos and hemiazygos venous system to the superior vena cava. 6 Indeed, in our patient, a calibrous vessel that can only be assigned to a dilated azygous vein was seen on CT.
In this case, it is not possible to affirm to which extent the aneurysm contributed to the outcome in a patient with underlying severe comorbidities. The cause of chronic renal failure could be ascribed to gout, although this association was more common before drugs that lower uric acid levels became available. Therefore, based on the results of the Doppler study, the decreased renal function could be at least partially assigned to the aneurysm. It already as been reported that IVC aneurysms are associated with longstanding venous hypertension in cases with outflow obstruction, 7 and venous hypertension can cause a decrease in the renal arterial perfusion pressure. 8 These statements are in accordance with the findings of IVC aneurysm associated with atretic suprarenal IVC (outflow obstruction) and absent blood flow in the right kidney (decrease perfusion) on Doppler study in our patient. We are aware of two reported cases of IVC aneurysm associated with renal insufficiency. In one case, the outcome was not reported, 5 and in the second one, acute renal failure was managed successfully by hemofiltration. 4 Therefore, a reported third case should prompt us to include renal failure as one of the possible features of infrahepatic IVC aneurysm.
A diagnostic algorithm for IVC aneurysm is lacking largely due to its rarity. In reported cases, diagnostic studies included contrast venography, CT scan, ultrasonography, and magnetic resonance imaging (MRI). On gray-scale ultrasonography, IVC aneurysm was first misdiagnosed as a renal cyst. CDUS was particularly helpful in our patient. It showed the aneurysm, defined the connection between the aneurysm and the IVC, and documented the interruption of the infrahepatic IVC. CT without contrast confirmed IVC stenosis and diagnosed a dilated azygos vein. In chronic renal disease, as in our patient, in which CT contrast agents and the gadolinium MRI contrast agent are not advisable, nonenhanced CT emerges as a method to study venous drainage. Indeed, in our patient, with nonenhanced CT, we were able to visualize that the only means of venous return from the aneurysm was via collaterals emptying into the distended azygous vein.
Conclusion
In conclusion, IVC aneurysm, although rare, should be considered in the differential diagnosis of renal hilar cysts. The etiology of these aneurysms remains unclear, but most are thought to be congenital or acquired. In our case, although a sonographic examination failed to identify the aneurysm, CDUS was crucial to the diagnosis and hence is a mandatory diagnostic method. According to American Institute of Ultrasound in Medicine guidelines, specialized examinations will maximize the probability of detecting abnormalities. When contrast agents are not advisable, nonenhanced CT can make a valuable contribution to the study of venous drainage. IVC aneurysm can be associated with chronic renal failure. Awareness of this entity and of complications that can occur from IVC aneurysms will enhance patient care.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.