
Abstract
Page kidney refers to the development of secondary hypertension due to compression of the kidney by an external source, most commonly a subcapsular hematoma. Compression of the renal parenchyma results in hypoperfusion and microvascular ischemia leading to activation of the renin-angiotensin system and elevation of blood pressure. Until the last decade, Page kidney was primarily diagnosed in young men with unexplained hypertension and a history of sports-related trauma and imaging studies demonstrating a subcapsular hematoma. Treatment varies from conservative, medical management to a nephrectomy, depending on how the patient’s blood pressure responds to treatment.
Introduction
Page kidney refers to the external compression of the renal parenchyma with resultant renal ischemia and systemic hypertension. It should be suspected in young, healthy patients with a new onset of hypertension and a history of trauma. Sonography is often the initial imaging modality for evaluating patients with hypertension and Sonographers need to closely evaluate the perirenal and subcapsular space for evidence of Page kidney caused by a lesion compressing the renal parenchyma. In the majority of cases, the cause of Page kidney is a treatable form of hypertension. A case is presented demonstrating the value of sonography in the diagnosis and management of Page kidney hypertension.
Case Report
A healthy male in his midteens was noted to have hypertension, 163/98 mmHG, during a routine sports physical. The patient’s medical history was otherwise unremarkable. Routine monitoring of his blood pressure by his primary care physician over the next few months showed no response to a low-sodium diet or anti-hypertensive medication. Further workup with a retroperitoneal sonogram demonstrated a complex, subcapsular fluid collection involving the right kidney measuring 13.0 × 10.0 × 8.1 cm (Figures 1 and 2). The fluid collection was noted to be compressing the kidney medially. Doppler evaluation of the intrarenal arteries was within normal limits with a Resistive Index of 0.61. The left kidney was normal. Based on the patient’s history, the fluid collection was believed to be a hematoma from a football injury in the prior season. The combination of these findings was most consistent with the diagnosis of Page kidney induced hypertension due to compression of the renal vasculature by the hematoma. Under computed tomography (CT) guidance, a pigtail drainage catheter was placed into the subcapsular hematoma and there was a marked decrease in the size of the hematoma with the drainage of approximately 1500 ml of coffee-colored fluid (Figure 3). Over the next 6 months, the patient’s history was complicated by the development of a perinephric abscess, recurrence of the subcapsular hematoma, and continued hypertension. Surgery was required to remove the hematoma and the patient’s blood pressure returned to normal. Four months following surgery, a renal sonogram found the right kidney to be normal in size and diffusely heterogeneous in appearance, most likely representing scarring from trauma and/or surgery (Figure 4).
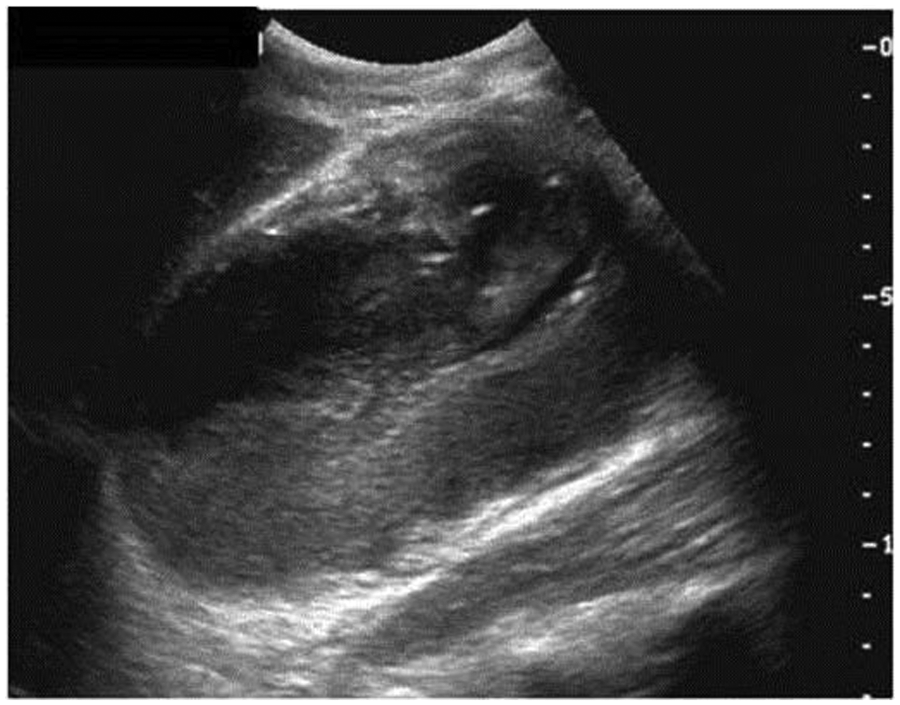
Long axis image of the right kidney demonstrating the subcapsular hematoma compressing the parenchyma.

Transverse image of the right kidney demonstrating the subcapsular hematoma compressing the parenchyma.
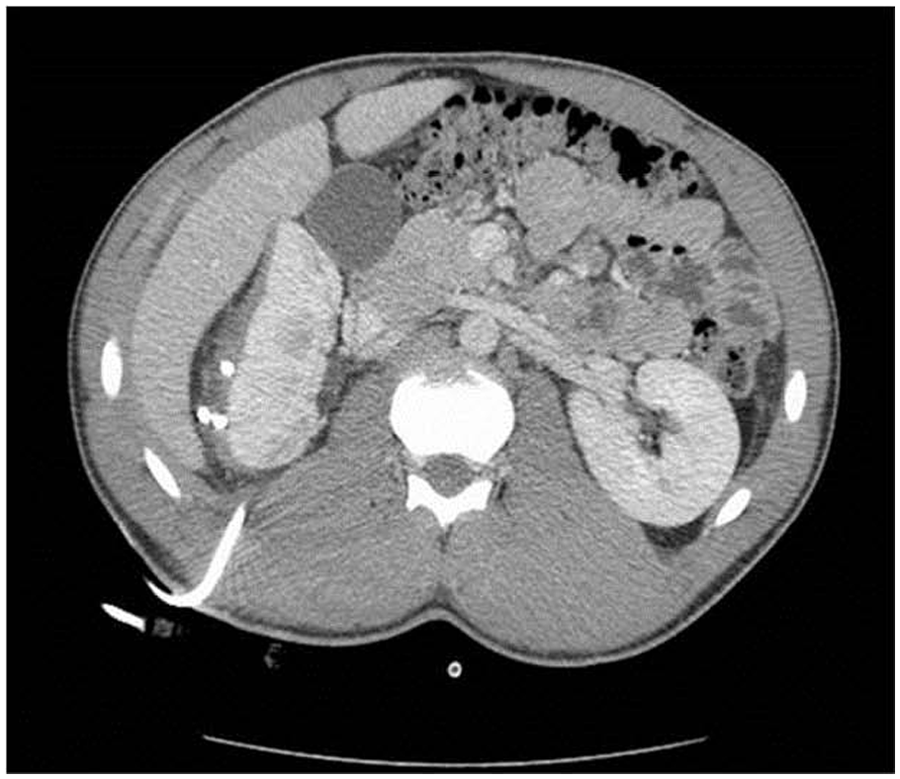
Computed tomography (CT) image showing reduction in subcapsular hematoma size post drainage catheter placement and drainage of 1500 ml of fluid.
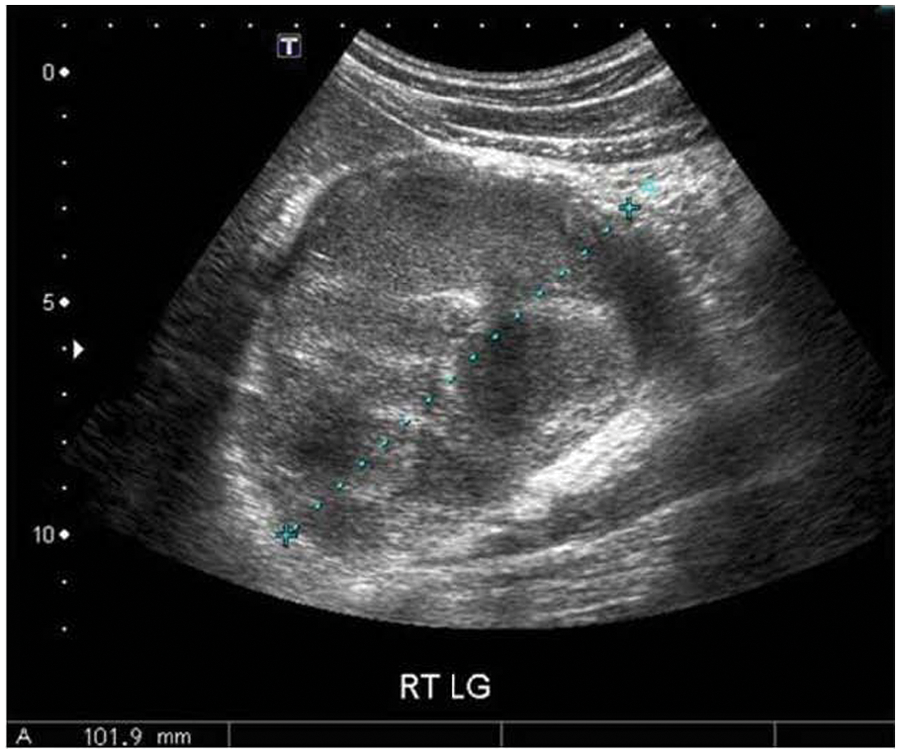
Long axis image of the right kidney following surgical removal of the subcapsular hematoma showing a normal size kidney (10.2 cm) with diffusely heterogeneous echogenicity.
Discussion
In 1934, Goldblatt et al. induced hypertension in dogs by constricting the main renal arteries with clamps and inducing renal ischemia. They showed that this led to the release of renin and the development of hypertension. 1 If the constriction process was only moderately severe in the beginning, hypertension developed without decreasing renal function. This became known as the Goldblatt kidney. In 1939, Dr. Irvin Page induced hypertension in animals by wrapping the kidneys loosely in cellophane. Within days, this would cause a tissue reaction with the formation of a constricting hull around the kidney parenchyma. The hull compressed the small parenchymal vessels, not the main renal artery, creating ischemia and renovascular hypertension. Hypertension developed whether one or both kidneys were chronically compressed. Page also documented that removal of the hull or the affected kidney eliminated the hypertension. 2 The induction of hypertension by renal compression became known as Page kidney or Page phenomenon. Page hypothesized that this hypertensive process might also occur with perirenal hematomas following trauma. In 1955, Engel and Page reported a case that supported this theory. It involved a 19-year-old male who had played high school football and had a 2-year history of hypertension. Clinical workup and pathological examination of the right kidney found a calcified subcapsular cyst compressing the kidney. A nephrectomy was performed and the patient’s blood pressure returned to normal levels. 3
Both Goldblatt and Page demonstrated that compression of the renal arteries, either major or microvascular arteries, leads to renal hypoperfusion, release of renin into the circulation, conversion of Angiotensin I to II, and the secretion of aldosterone from the adrenal glands. This is known as the renin-angiotensin system (RAS) or the renin-angiotensin-aldosterone system (RAAS). Activation of this system leads to vasoconstriction of the blood vessels and increased reabsorption of sodium and water by the renal tubules into the blood, both leading to increased blood pressure and renin-dependent hypertension. It is important to note that Page kidney is a rare complication of renal trauma. 4 There must be compression of the renal parenchyma to cause ischemia. Subcapsular hematomas, even those small in size, are more likely to produce renal compression and ischemia because they are contained than are extracapsular hemorrhages that can expand into the retroperitoneal space without compressing the kidney.3,5
The classic presentation of Page kidney is a healthy, young male athlete with a remote history of flank trauma and newly discovered hypertension. Renal function and serum creatinine levels are typically normal unless the contralateral kidney is diseased or there is a single kidney.5–9 These clinical finding are similar to the patient in our case report. Chronic, subcapsular hematoma related to contact sports was initially the most common reported etiology of Page kidney, but this has changed over time. 8 In 1991, McCune et al. reviewed the 80 published cases of Page kidney and reported the most common cause to be blunt abdominal trauma from American football (22%) and non-sports trauma (22%). In many cases, the actual cause of the trauma was presumptive, with no definitive history of renal trauma or hematuria and the time elapsed between the traumatic event and the diagnosis. 5 In 2009, Dopson et al. reviewed the 28 new cases of Page kidney that were reported between 1991 and 2009; 36% of these cases were attributed to kidney transplant biopsies. Only one case was attributed to sports-related trauma and one case to non-sports trauma. Factors possibly affecting this shift include: better protective sports gear, improved resolution and availability of imaging modalities allowing for early diagnosis of trauma, increased number of kidney transplants and biopsies, and changes in publication emphasis. 6 Dopson also noted that Page kidney in a renal transplant, where kidney function is often compromised, is a different entity than native Page kidney.
Diagnosis of suspected Page kidney requires a thorough patient history for latent, blunt abdominal trauma and imaging studies documenting a fibrous capsule or hematoma compressing the kidney. 5 Sonography and CT are the preferred modalities for demonstrating a subcapsular hematoma, but sonography has the added benefit of assessing renal vascular perfusion. 9 The sonographic appearance of a subcapsular hematoma demonstrates a fluid-filled mass compressing the renal parenchyma. The internal components of the hematoma become more complex with age. An echogenic, irregular capsule may also be noted. The subcapsular hematoma will demonstrate lack of blood flow by color Doppler imaging and spectral Doppler. Assessment of the compressed intrarenal vessels with spectral Doppler may reveal an elevated Resistive Index (RI) of >0.7; the RI in our case was normal at 0.61. Additional benefits to sonographic assessment include low cost, lack of ionizing radiation, and its use for patient follow-up. Sonography is limited by operator experience. CT offers improved resolution for imaging small subcapsular hematomas and the retroperitoneum in cases of perinephric hematomas. Magnetic resonance imaging (MRI) has the added benefit of estimating the age of the hematoma.5,9
The goal of treatment is to relieve compression of the kidney, restore normal perfusion, and return the patient to a normotensive state. 9 There is no single accepted standard treatment for Page kidney, but there is a trend toward less invasive methods. Medical management with oral medications that block the renin-angiotensin-aldosterone system may be effective and allow time for the hematoma to spontaneously resolve.5,7,9–11 Persistent hypertension requires percutaneous drainage of the hematoma, but reaccumulation of fluid may occur. Surgical management options for Page kidney include capsulectomy, hematoma evacuation, and radical nephrectomy. 6 The age of the subcapsular hematoma does seem to affect the treatment outcome, with more invasive methods required as the hematoma ages.9,11,12
Conclusion
The phenomenon of Page kidney is due to external compression of the renal parenchyma, typically by a traumatic subcapsular hematoma, which leads to decreased renal perfusion and renin-dependent hypertension. Although it is rare, sonographers should recognize the classic medical history of a healthy male with unexplained hypertension and possible past episode of abdominal trauma. Sonography is often the initial imaging modality used to evaluate these patients and careful imaging of the kidneys and perinephric area for a subcapsular hematoma is imperative for a correct diagnosis. Secondary hypertension from Page kidney is a curable form of hypertension.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.