
Abstract
This case study describes a newborn male infant with cat eye syndrome, found to have a rare constellation of congenital defects, which included an interrupted aortic arch, type B2 (with aberrant right subclavian artery), aortic valve atresia, aorto-pulmonary window, left coronary artery to pulmonary artery fistula, ventricular septal defect, atrial septal defect, and a restrictive patent ductus arteriosus.
Keywords
Introduction
Approximately 1% of all births each year in the United States have congenital heart disease. 1 It is also estimated that 1 out of every 74,000 (.001) babies are born with cat eye syndrome, a relatively rare genetic abnormality that presents with a variety of congenital anomalies. 2 Echocardiography plays a key role in identifying congenital heart defects. The following case describes an extremely rare constellation of complex congenital heart lesions in a newborn infant also diagnosed with cat eye syndrome. A literature search yielded only 12 cases of interrupted aortic arch (IAA) with aortic valve atresia; however, none of these reports noted cat eye syndrome.
Case History
A term baby was admitted to the neonatal intensive care unit (NICU) following cesarean delivery for surgical evaluation of imperforate anus. Prenatal history was notable for polyhydramnios and maternal obesity. Maternal social history was negative for drug and alcohol use. There was no family history of congenital heart disease or genetic syndromes. Apgar scores at birth were 6 and 9. Vital signs upon arrival were heart rate of 168 bpm, blood pressure of 72/45 mmHg, respirations of 46, and O2 saturation 93%. Physical examination showed external auricle pits bilaterally and a skin tag on the left ear in addition to an imperforate anus with no appreciable fistula (common findings in cat eye syndrome). There was a grade II/VI long systolic murmur at the left sternal border. The infant was noted to have normal tone, moro reflex (startle reflex), grasp, and suck. There were no extremity deformities.
Following arrival to the NICU, cardiology was consulted to evaluate the cardiac anatomy. An echocardiogram was performed with a Philips iE33 (Bothell, WA) with findings of an interrupted aortic arch type B2 (with aberrant right subclavian artery, Figure 1), aortic valve atresia (Figure 2), aorto-pulmonary (AP) window (Figure 3), left coronary artery (LCA) to pulmonary artery (PA) fistula (Figures 4 and 5), ventricular septal defect (VSD), atrial septal defect (ASD), and restrictive patent ductus arteriosus (PDA) (Figure 6). The infant was subsequently started on prostaglandins and underwent a colostomy as further surgical options were assessed.
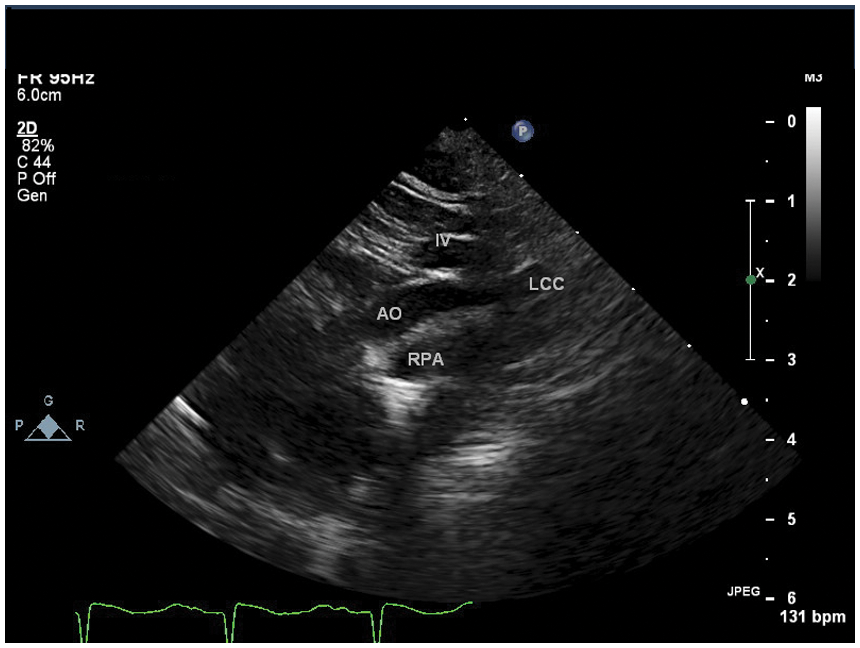
Suprasternal notch view of the interrupted aortic arch (IAA). The ascending aorta courses superiorly showing the carotid artery take off without the normal continuity of the transverse arch and descending aorta
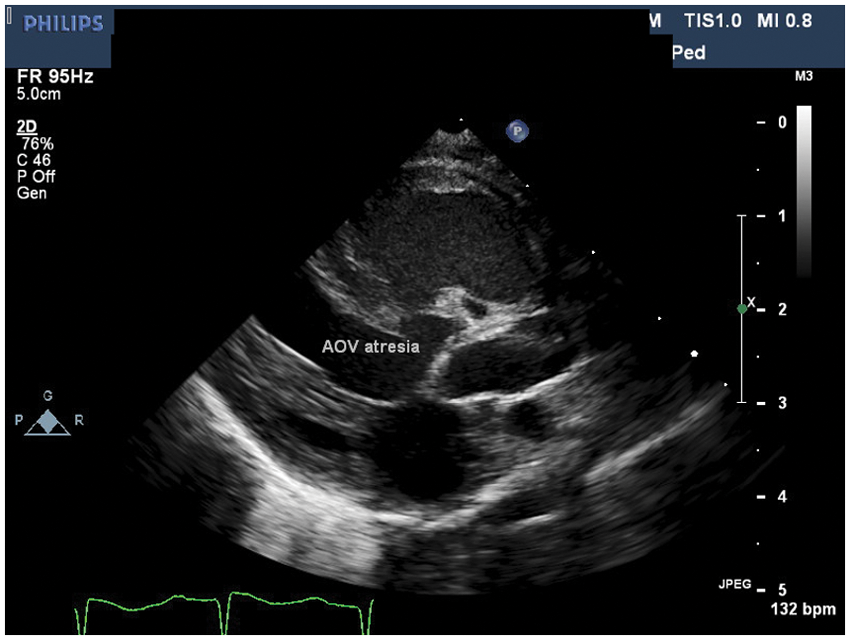
Parasternal long axis view demonstrating aortic valve atresia and perimembranous VSD with posterior malalignment
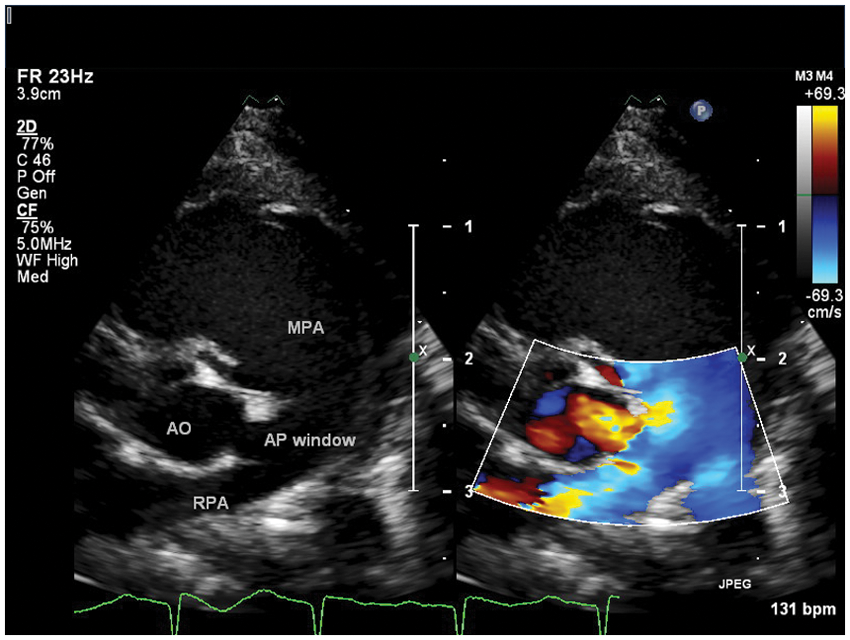
Parasternal short-axis view just above the level of the coronary arteries demonstrating an AP window at the junction of the main pulmonary artery and right pulmonary artery with right to left shunting (shunting from the pulmonary artery through the AP window into the ascending aorta)
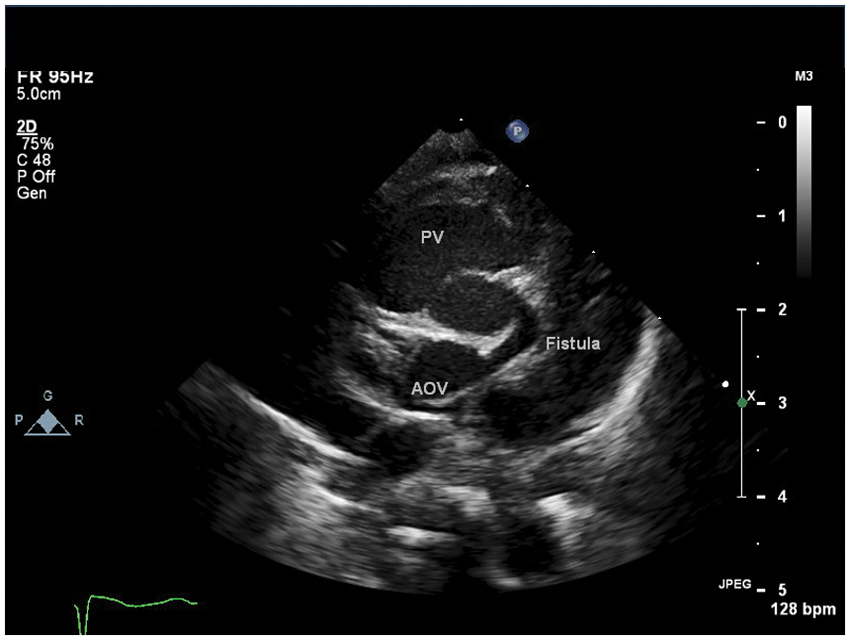
Parasternal short axis view at the level of the coronary arteries showing the fistulous connection of the left coronary artery to the main pulmonary artery
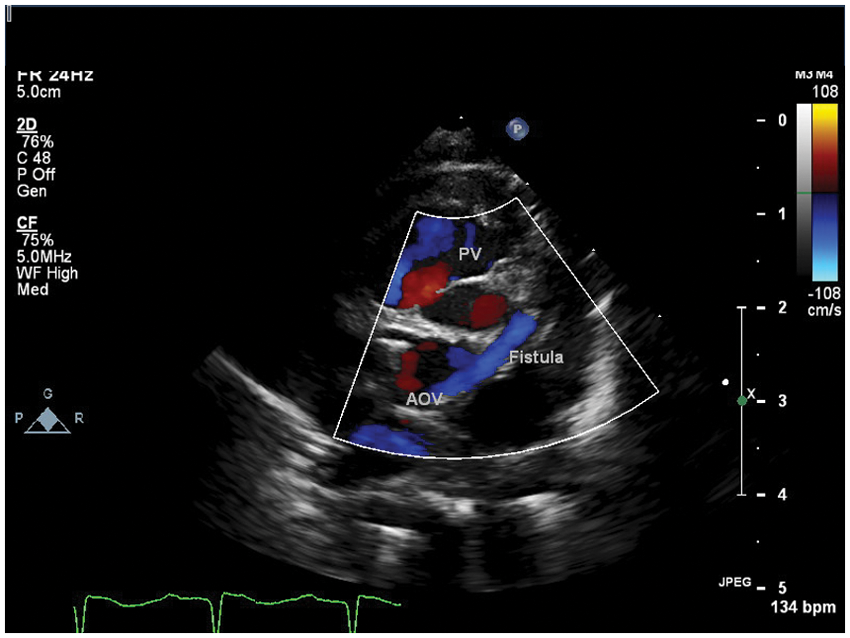
Parasternal short axis view demonstrating the right to left shunting (from the pulmonary artery to the aorta, blue flow) through the fistula
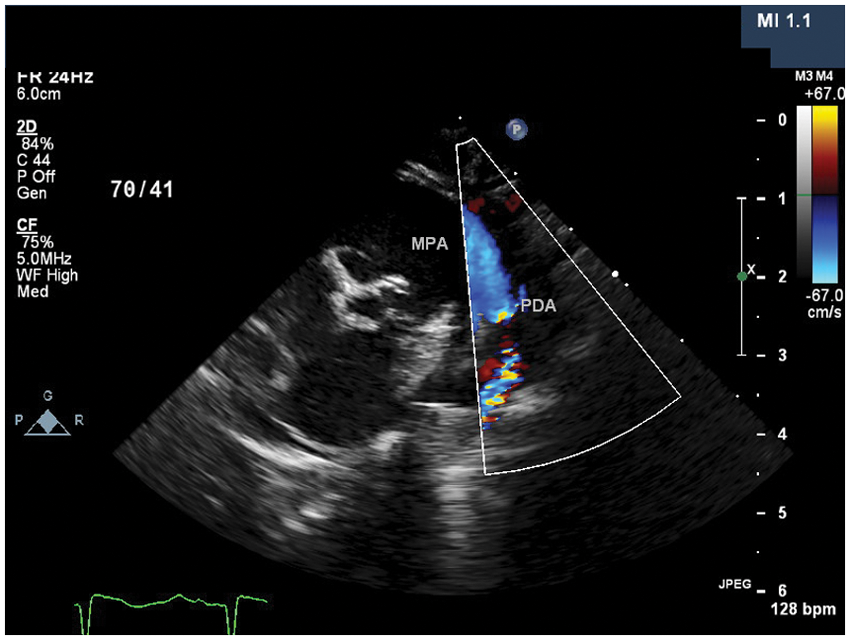
Suprasternal sagittal view demonstrating the restrictive ductus arteriosus with right to left shunting (shunting from the pulmonary artery into the descending aorta)
The neonate was subsequently found to have left hydronephrosis, a complex septated hepatic cyst, and a small intraventricular hemorrhage. Genetic testing confirmed a diagnosis of cat eye syndrome. Due to the complexity of the intracardiac anatomy there was significant discussion regarding the surgical options. Once the baby had clinically stabilized, a Norwood procedure (connecting the main pulmonary artery to the aorta) with a modified Blalock-Taussig shunt (a Goretex® tube connecting the innominate artery to the right pulmonary artery to supply blood flow to the pulmonary arteries), IAA repair, main PA division, and repair of the AP window were performed, with the goal of an eventual biventricular repair.
Discussion
Interrupted aortic arch is a rare congenital defect that accounts for only approximately 1% of all congenital cardiac defects. 3 Type B IAA is the most common, occurring in 60% to 70% of cases, and results in a complete interruption between the left common carotid artery and the left subclavian artery. The patient in this case study also had an aberrant right subclavian artery arising from the descending aorta instead of the transverse aortic arch, which occurs in approximately 50% of type B IAAs (and is referred to as type B2 IAA). 4 The ascending aorta in this case supplied blood flow to the head via the left and right common carotid arteries. In addition, this patient had a PDA that provided blood flow to the arms and lower body. Had the PDA closed, this infant would have gone into cardiogenic shock if left untreated. 5
IAA with aortic valve atresia would not have been compatible with life without the presence of additional blood flow to the ascending aorta, which in this patient was provided by an AP window as well as a coronary artery fistula. There was right to left shunting across the AP window, and the LCA to PA fistula supplied retrograde blood flow to the ascending aorta, coronary arteries, and head and neck vessels. One interesting factor in this case was the presence of both an AP window and an LCA to PA fistula. One could postulate that the AP window (3 mm) was of inadequate size to supply sufficient blood flow to the coronary arteries and head and neck vessels. Therefore, additional blood flow from the coronary fistula, albeit minor, could have aided to provide additional blood supply. As discussed by Yew et al., the source of blood supply to the ascending aorta is variable in patients with IAA and aortic valve atresia, with AP windows being the most common. 6
There is almost always a VSD present in IAA, with an incidence of 94% to 100%. 4 Due to the aortic valve atresia, the large muscular VSD with outlet extension, in which the defect extends into the outlet portion of the ventricular septum, in this infant served as the outlet for the left side of the heart. This allowed the blood on the left side of the heart to cross the ventricular septum and exit the heart via the pulmonary artery.
In addition to the complex heart anomalies previously described, this infant was found to have cat eye syndrome. Cat eye syndrome is a rare genetic syndrome with a variable pattern of congenital anomalies. Some of these characteristic features include ocular coloboma, craniofacial and skeletal anomalies, pre-auricular pits or tags, anal anomalies, congenital heart defects, renal malformations, and in some cases, mental retardation.7–9 Genetically, cat eye syndrome is a result of multiple duplications, typically trisomy or tetrasomy, of the short arm and a small region of the long arm of chromosome 22. In patients with cat eye syndrome, at least one third are found to have a congenital cardiac defect. 10
Conclusion
Cat eye syndrome is associated with cardiac defects ranging from simple septal defects to complex conotruncal abnormalities, as described previously. Echocardiography plays a key role in identifying congenital heart defects (CHD) and can reduce the morbidity and mortality of some cardiac diseases. The complex cardiac defects found in this child are extremely rare and required extensive analysis and discussion regarding medical and surgical management.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support for the research and/or authorship of this article.