
Abstract
A case report is presented of a sonographic examination at 39 weeks’ gestation that showed a nonvascular fetal oral mass. The patient was transferred to a tertiary referral hospital where an ex utero intrapartum treatment (EXIT) procedure was planned; however, delivery was subsequently completed without the need of this procedure. The neonate underwent marsupialization of the mass with the final diagnosis of a ranula or lymphangioma. This case report emphasizes identification of a fetal oral mass, appropriate diagnostic tools to evaluate oral masses, and treatment options for these patients.
Nonvascular soft tissue masses of the fetal oral cavity are rare, with a reported incidence of 1.7 to 13.5 per 100,000 live births. 1 The differential diagnosis includes ranula/lymphangioma, foregut duplication cyst, frontal cephalocele, dermoid or teratoma, myoblastoma, cystic hygroma, hemangioma, macroglossia, and neurofibroma. 2 These are important to diagnose and treat because isolated fetal oral cavity masses can cause obstetric complications such as polyhydramnios and delivery complications such as impairment of the fetal airway, possible hypoxia, and even death at birth. Sonography particularly can be a useful tool to identify fetal oral masses, and the use of both traditional 2D sonography and newer 3D modalities is helpful in the diagnosis and planning for fetal delivery.
Case Report
A patient with uncomplicated antenatal care at 39 weeks’ gestation (G2P1001) was transferred to a tertiary referral hospital following an incidental sonographic finding of a fetal oral cavity mass during a routine labor evaluation. The oral mass had not been seen previously during any routine prenatal sonographic studies. Upon arrival to the hospital, a sonographic examination was performed using a Philips IU22 with a C5-1 curved-array transducer. Sonography showed a fetus with a 3.0 × 2.1 × 2.0-cm cystic mass (volume of 6.6 cc) within the fetal oral cavity (Figure 1) and a small 5-mm pericardial effusion, with otherwise normal anatomy. The oral cystic mass was unilocular and midline, and it had no solid components and demonstrated no acoustic shadows. The cyst wall was well demarcated and limited to the oral cavity. The interior of the cyst was homogeneous, anechoic, and without excrescences. There was no vascular flashing within the cyst when using color Doppler. 3D sonographic imaging was then done using a 6-2 broadband curved transducer to further clarify these findings (Figure 2). The 3D images demonstrated a structure within the oral cavity that did not extend past or involve the visible lips. There were no apparent facial deformities, and the mouth was seen to be open. It appeared from fluid in the stomach that the fetus was swallowing appropriately. The patient was admitted for observation overnight and for consultations with a pediatric ear, nose, and throat (ENT) physician; a maternal fetal medicine physician; and a neonatologist. After full evaluation by these team members, an ex utero intrapartum treatment (EXIT) procedure was planned via cesarean section the following morning.
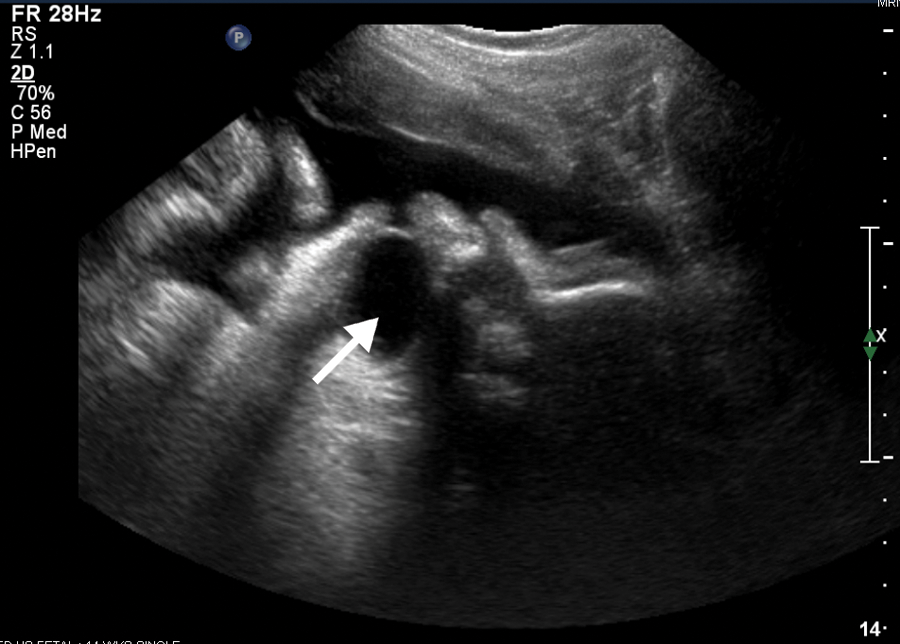
2D image of 3.0 × 2.1 × 2.0-cm (6.6-cc) cystic mass within the fetal oral cavity (arrow).

3D image of the cystic mass showing no involvement of the visible lips.
A primary low-transverse cesarean delivery was performed under general anesthesia with an anesthesiologist, obstetricians, neonatologist, and pediatric ENT all present at the time of delivery. Upon delivery of the fetal face, the pediatric ENT inspected the infant and determined that it appeared safe to complete the delivery without the need for intubation before delivery based on the baby’s ability to immediately breathe and the size of the oral mass. A 3200-g male infant was delivered with Apgar scores of 5 and 7 at one and five minutes, respectively, and cord pH of 7.29. Upon further inspection, the infant was found to have a cystic sublingual mass. This mass was aspirated in the operating room, and 20 mL of amber-colored cloudy fluid was obtained that appeared benign in nature. The baby was then intubated under general anesthesia, and laryngoscopy and bronchoscopy showed no laryngeal involvement of the mass. A marsupialization procedure of the mass was then performed. The baby was transferred to the neonatal intensive care unit (NICU) and extubated the following day without complications. Over the course of the next several days, the mass reaccumulated with fluid beginning to obstruct the infant’s airway. Neonatal magnetic resonance imaging (MRI) was used to better visualize the mass, which showed a sublingual cystic mass (Figure 3). The patient was taken to the operating room for a primary resection of the mass (Figure 4), which was believed to be a lymphangioma. Pathology later confirmed the diagnosis of lymphangioma, also known as a ranula, with no evidence of malignancy. A neonatal echo was performed, and no abnormal pericardial fluid collection was found. The infant was eventually discharged home after appropriate feeding was achieved without any further complications.
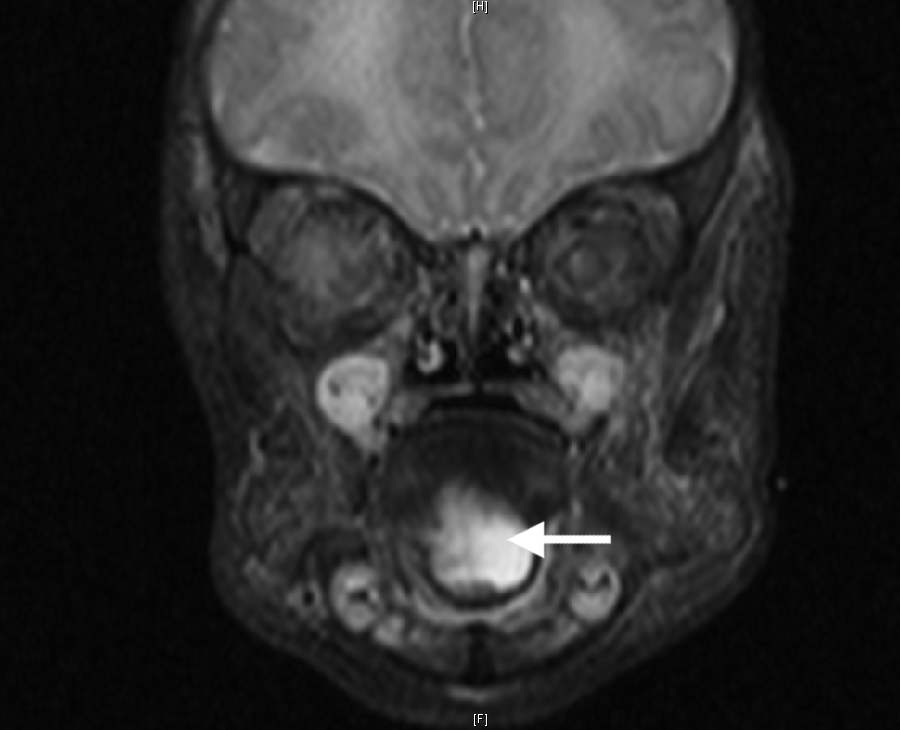
Neonatal magnetic resonance imaging showing the recurrent sublingual cystic mass (arrow).

Photograph of recurrence of the cystic mass several days after delivery and aspiration, just prior to surgical resection.
Discussion
Appropriate fetal diagnostic tests antenatally are important in identifying and characterizing a mass and planning for fetal delivery. The most common and least invasive imaging is traditional 2D ultrasonography. 3D surface rendering can allow for more details of what involvement of the fetal face is seen.3–5 It can also help distinguish if any other abnormal facial features are present in conjunction with the mass, including a cleft lip or an oral abnormality. In addition, Doppler sonography can be used to evaluate both blood flow and vessel formation. The disadvantages of using sonographic imaging are that it is operator dependent, has a relatively small field of view, can be affected by fetal position, and provides only limited soft tissue and bone acoustic contrast such that body habitus and amniotic fluid both influence the image. MRI, another imaging modality that can be used antenatally, allows excellent detail of soft tissues. It provides multiplanar capabilities, does not use ionizing radiation, and has a large field of view.6,7 The disadvantages of MRI are that it is relatively expensive, has less spatial resolution, is not sensitive to fetal motion, is not available in all locations, and is stressful for mothers with claustrophobia. Computed tomography (CT) scanners can also be used antenatally for fetal imaging.6,8,9 The advantages of using CT scanning are that it can help recognize bone involvement with oral masses and can be used when MRI is contraindicated, such as when mothers have pacemakers or metallic foreign bodies. The disadvantages of CT scans include exposure to radiation, cost, and lack of ready availability in some hospital settings.
Delivery of a fetus with an oral mass can be problematic because of potential airway involvement. An EXIT procedure (also known as operation on placental support [OOPS] procedure) allows for environmental controlled delivery to avoid hypoxia, brain injury, and death. 10 This differs from a standard cesarean delivery because the EXIT procedure allows the uterus to achieve a state of hypotonia, which helps prevent placental abruption. The procedure uses deep anesthesia while maintaining blood pressure and achieves a state of fetal anesthesia without cardiac depression to allow evaluation and possible surgery immediately after delivery. The key is to make a uterine incision while avoiding the placenta to avoid hemorrhage, with the associated use of tocolytics to allow uterine hypotonia. Immediately after delivery, reversal of the hypotonia is necessary to prevent maternal hemorrhage.10,11 The fetus can then be taken for evaluation using laryngoscopy, bronchoscopy, or tracheostomy and possibly surgery if necessary. 10 Once a fetal oral mass has been identified sonographically in the antenatal period, the appropriate team members must be consulted and need to communicate to ensure a safe infant delivery. This team includes an obstetrician, perinatologist, neonatologist, pediatric surgeon, and anesthesiologist. Each team member plays an important role in ensuring that the infant has a successful delivery and outcome after delivery.
A ranula, also known as a lymphangioma, is a pseudocyst that is associated with sublingual and submandibular ducts. 12 The incidence of this mass is rare and occurs in only 2 per 100,000 births.13–15 It can cause improper drainage of the glands, resulting in mucous invading surrounding tissue and forming a cystic mass structure. The appearance of a ranula is usually blue to translucent in color and usually is unilateral in the mouth. The mass can displace the tongue superiorly and medially and does not blanch when compressed. Ranulas are classified into two different types, oral or cervical, depending on their location. An oral ranula is found with mucous pools located superior to the mylohyoid muscle, and a cervical ranula is elevated along the facial plane of the neck. Ranulas are usually asymptomatic, although if large in size, the mass can obstruct airways and restrict respiration as well as swallowing, speech, and mastication. 12 They are found more commonly in females, with a male-to-female ratio of 1:1.4. These masses typically present in the second decade of life, but they can appear at any stage of life from the antenatal period until death. Treatment of a ranula is complete excision, which may or may not include excision of the sublingual gland. If the mass cannot be completely excised, a marsupialization procedure, suturing the cyst wall to the mucosa of the mouth, can be performed.
Conclusion
A case of a fetal oral mass seen prenatally with the final diagnosis of a ranula is presented. Although fetal oral masses are rare, many differential diagnoses need to be considered and ruled out, including foregut duplication cyst, frontal cephalocele, dermoid tumor, myoblastoma, cystic hygroma, hemangioma, macroglossia, and neurofibroma. Using prenatal imaging techniques (including ultrasonography), preparing intrapartum for delivery, and promptly performing any necessary treatment of the newborn are all important steps in having a healthy infant who is born with one of these conditions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.