
Abstract
Larsen syndrome is a rare inherited disorder of collagen formation with multiple joint dislocations, cardiac abnormalities, short stature, talipes equinovarus, short and broad fingertips, spatula-like thumbs, supernumerary ossification center in the calcaneus, hearing loss, neurologic impairment, cryptorchidism, and characteristic craniofacial abnormalities. The sonographic prenatal findings in a case of Larsen syndrome at 26 weeks’ gestation, which demonstrated joint dislocations, hypertelorism, frontal bossing, micrognathia, and upper and lower limb shortening and confirmed at both 29 and 30 weeks’ gestation, are presented and discussed. When evaluating patients with a positive family history of Larsen syndrome, sonographers should carefully scan and meticulously assess the fetal extremities for signs of dislocation and the face for signs of flat features, hypertelorism, micrognathia, and depressed nasal bridge, distinctive features of the syndrome.
Larsen syndrome is a skeletal dysplasia that is characterized by multiple fetal anomalies with an incidence of approximately 1 in 100,000 births 1 and a female predominance. 2 It was first reported by Larsen et al. 1 in 1950. Since then, few cases that were diagnosed prenatally have been reported.3–8 A case of Larsen syndrome is presented in which its associated anomalies of characteristic joint dislocations and facial features and abnormalities enabled a prenatal diagnosis of this rare entity to be made.
Case Report
A woman in her mid-30s, G4P3, was referred to our affiliated hospital for a sonographic examination at 26 weeks. The patient’s physical examination was unremarkable. Her past obstetrical history was significant for a healthy child and two children diagnosed with Larsen syndrome. She denied consanguinity and any history of exposure to teratogenic agents or chemotherapy.
Sonographic examination of the fetus using 3-MHz curvilinear array transducer (128XP; Acuson, Mountain View, California) revealed a single female fetus in a cephalic presentation with a normal fetal head biometry, consistent with date, and normal amniotic fluid. The femur length measurement was 4.1 cm, corresponding to 23 weeks and 1 day and consistent with being small for the gestational age.
Because of her positive history of children with Larsen syndrome and the syndrome’s known features, detailed and targeted evaluation of the fetal limbs and face was performed. The fetal evaluation showed dislocation of both hips and knees (Figure 1A,B) and bilateral shortening of the upper extremities (Figure 2A,B) without successful determination of elbow dislocation. Real-time sonography allowed the exclusion of joint stiffness and muscle wasting, which are associated with other skeletal dysplasia syndromes. In addition, fetal anatomic evaluation demonstrated frontal bossing, micrognathia, depressed nasal bone (Figure 3), and hypertelorism (Figure 4). Based on the obstetric history and the sonographic findings, a definitive prenatal diagnosis of Larsen syndrome was made. An amniocentesis revealed a normal karyotype of 46, XX.
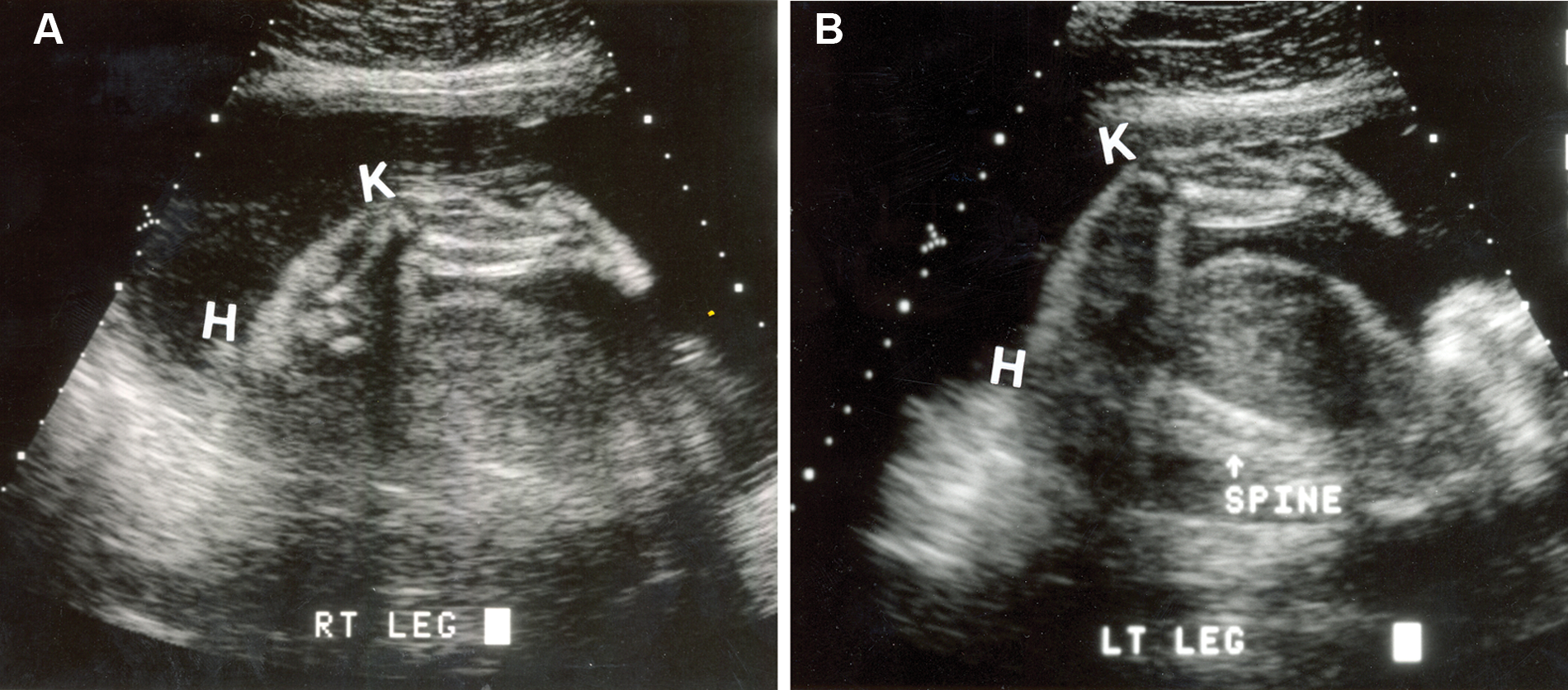
A 2D sagittal image of the (A) right lower extremity and (B) left lower extremity shows dislocation of the hip (H) and knee (K).
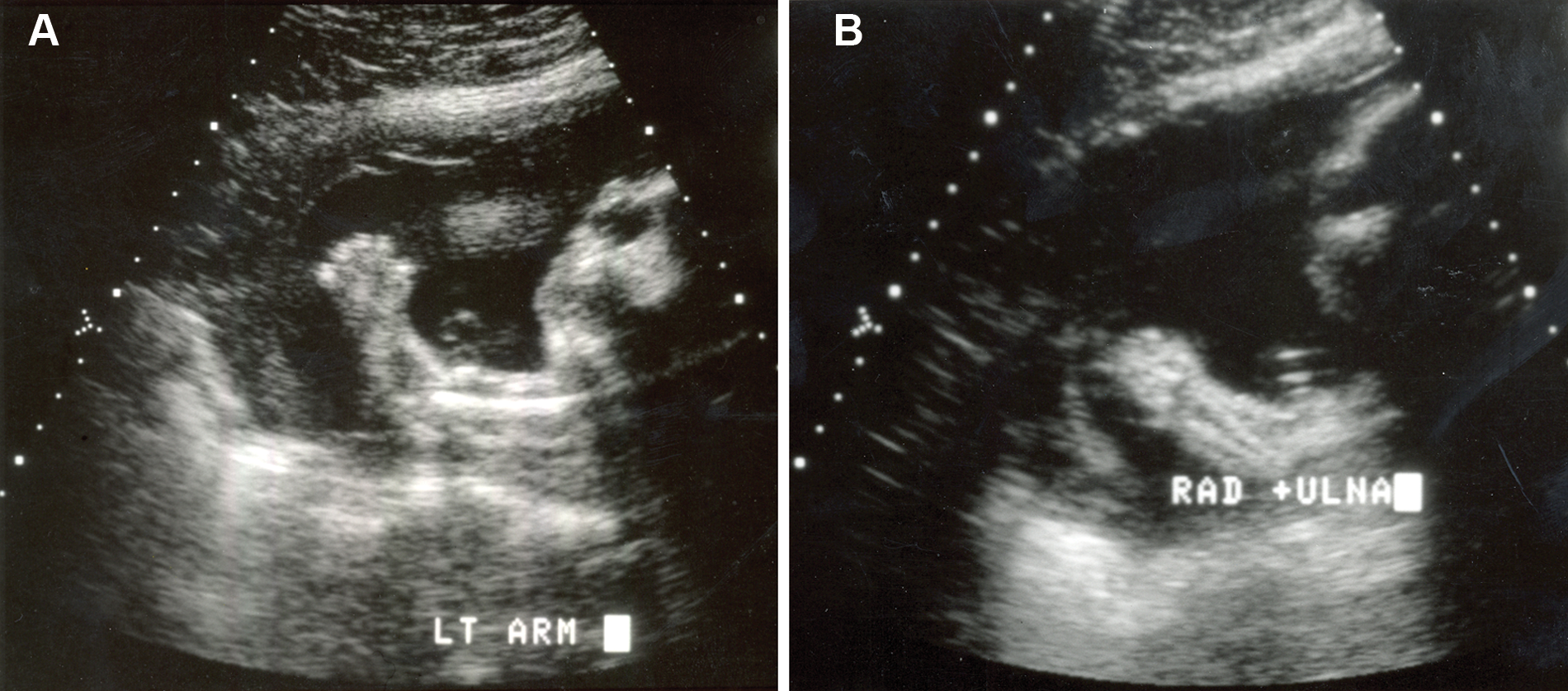
(A) A sagittal view of the left upper extremity demonstrates short extremity without proper determination of elbow dislocation. (B) A sagittal view of the right upper extremity shows short radius and ulna without proper determination of elbow dislocation.
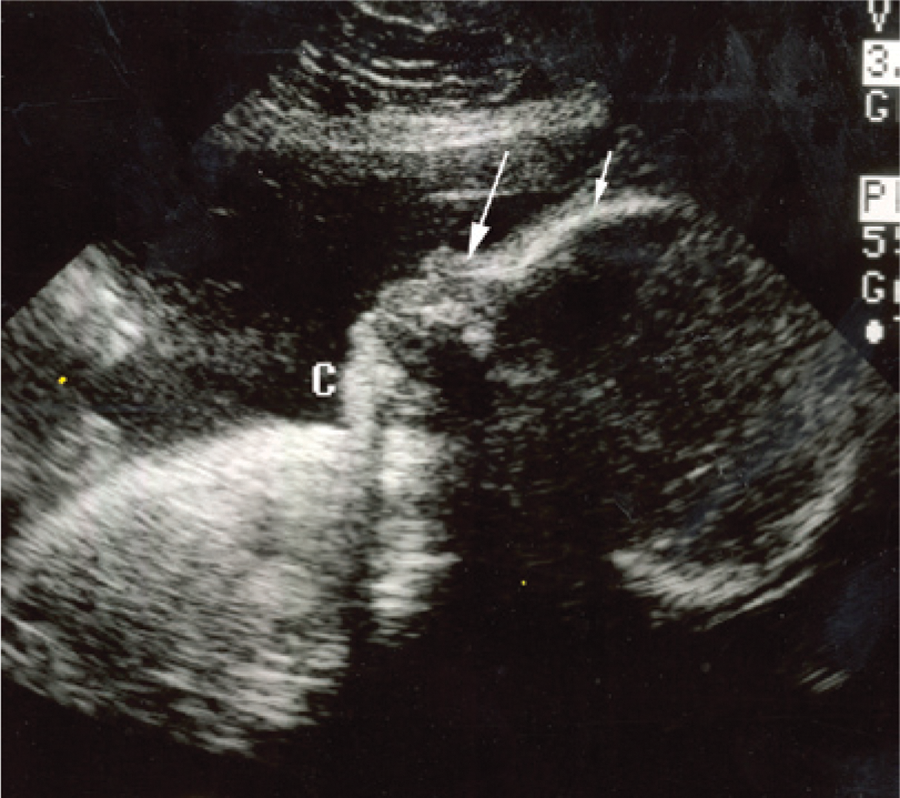
A fetal profile sonogram demonstrates micrognathia (c), frontal bossing (short arrow), and low root nasal bone (long arrow).
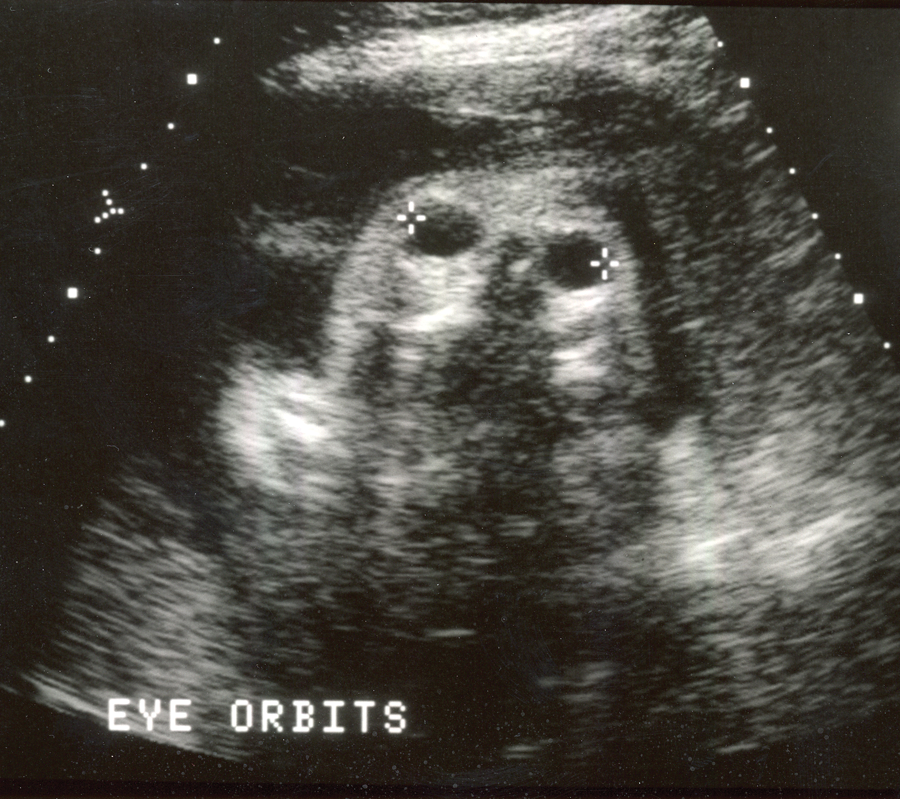
An axial sonogram through the orbits demonstrates hypertelorism.
Serial sonographic examinations at 29 and 30 weeks confirmed the previous findings and revealed normal fetal growth. The patient elected to seek further counseling and obstetric management at a high-risk obstetric institution. At a later time, the patient underwent an elective cesarean section, and the diagnosis of Larsen syndrome was confirmed.
Discussion
Larsen syndrome is a rare genetic disorder that can be transmitted by either dominant or recessive traits.9–12 It is characterized by multiple joint dislocations, severe joint laxity, facial dysmorphia, short stature, and syndactyly.1,13–17 In addition, talipes equinovarus, 2 short and broad distal phalanges, 2 cardiovascular anomalies,2,18,19 hearing loss, 20 hydrocephalus, 21 instability of the cervical spine,2,16,22,23 neonatal tracheomalacia and pulmonary hypoplasia,3,4 neurologic abnormalities, 24 oligohydramnios, 25 and psychomotor retardation 26 have also been reported. Moreover, uncommon abnormalities such as additional pair of ribs, agenesis of the corpus callosum, colpocephaly, pachygyria, and iris heterochromia have been documented. 24
Although there are no definitive genetic biomarkers for this syndrome and its diagnosis is dependent on typical phenotypic characteristics, mutations in the LAR1 gene at locus 3p21.1.25 and filamin B (a cytoplasmic protein that regulates the structure and organization of F-actin and controls and guides proper skeletal development) located at chromosome 3p14.3 have been reported as possible etiologies.27–30
The use of imaging modalities such as 2D and 3D sonography has enhanced the prenatal diagnosis of Larsen syndrome.3–5,7,8,15,24 Many of the features that have been documented and reported prenatally include prominent forehead, flattened faces, micrognathia, hypertelorism, depressed nasal bone and cleft palate,3–5,7,8,31 club feet, 2 and dislocations of the hips, elbows, and knees (anterior luxation).3–8,15,17,24,31 Other prenatal sonographic findings such as hydrocephalus, oligohydramnios, ventricular septal defects, and agenesis of the corpus callosum have also been reported.21,24,25 Even though, in this case, the prenatal diagnosis of Larsen syndrome was suspected by the utilization of 2D sonography, the use of 3D sonography would have allowed a better visualization of the fetal facial features as well as a more detailed view of the limb defects and enhanced the diagnosis.
Although sonography has improved the prenatal diagnosis of Larsen syndrome, in some cases, a definitive diagnosis can be uncertain because of the numerous sonographic findings shared with other skeletal dysplasia disorders such as arthrogryposis multiplex congenita, Ehler-Danlos syndrome, and otopalatodigital syndrome.2,4,6,8,32 However, in this case, the prenatal diagnosis of Larsen syndrome was suspected based on the presence of hip and knee dislocations (joint laxity), the absence of extreme stiffness of joints and muscle dystrophy, micrognathia, hypertelorism, frontal bossing, and prior positive family history. Most authors believe that the anterior dislocation of the knees can be considered the cardinal feature of this syndrome, which correlates with the findings in this case.3,5–7,12,16,31,33
Postnatally, children with Larsen syndrome may require aggressive orthopedic management 7 ; may have frequent respiratory complications, hypotonia, and epilepsy (due to focal cortical dysplasia)7,24; or may lead productive lives with normal fertility. 8 Death has also been reported in neonates with this syndrome due to cardiopulmonary arrest resulting from cervical spine instability. 7 The prognosis of this syndrome is variable and depends on the severity of the abnormalities. Many authors believe that the prognosis becomes poor when tracheomalacia, pulmonary insufficiency (lung hypoplasia), and collagen fiber dysmaturity are present.34,35
Conclusion
Given the sonographic imaging technology currently available, direct visualization of the fetal skeletal system is now possible. The diagnosis of Larsen syndrome can be straightforward on sonography when joint dislocations, micrognathia, hypertelorism, depressed nasal bridge, and frontal bossing are identified and correlated with a prior positive family history such as in this case.
Prenatal recognition of Larsen syndrome is significant not only because of the important distinction from other skeletal dysplasia abnormalities but also because identification and characterization of the disease may have implications for the optimal mode of delivery. The prenatal diagnosis may also help in providing parents with the option of pregnancy termination, if the parents desire; appropriate obstetrical management and planning; surgical and medical treatment; or adequate counseling about the long-term prognosis of the disease.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.