
Abstract
A Sister Mary Joseph nodule (SMJN) is a malignancy located in the periumbilical region. Often misinterpreted as a simple hernia, it is associated with advanced metastatic cancer. First reported in 1846, its primary sources include the gastrointestinal system and female reproductive sites. The most common origins include gastrointestinal (52%), gynecologic (28%), stomach (23%), and ovarian (16%). The presence of SMJN usually indicates widespread disease and is associated with a poor prognosis and complex therapeutic implications, with average patient survival of only 10 to 11 months after diagnosis. This report demonstrates the capability of sonography to evaluate soft tissue periumbilical masses, describes their sonographic appearance, and evaluates the utility of sonography to accurately locate the SMJN for biopsy.
On a routine abdominal sonogram, a solid vascular mass was discovered in the umbilical region. The prior computed tomography (CT) studies reported this as a simple hernia. A surgical consult also reported this as an “umbilical protuberance, most likely due to increased intra-abdominal pressure.” Despite these reports, the gastroenterologist suspected the mass was a Sister Mary Joseph nodule (SMJN). A biopsy was performed, which resulted in a diagnosis of malignant epithelioid mesothelioma. This case contradicted the common perception that all umbilical masses were only simple hernias. Greater care needs to be taken when interrogating the umbilical region to separate the benign (hernia) from the malignant mass.
The discovery of a metastatic mesothelioma in the umbilical region prompted this cohort study, collecting data on all new or suspected umbilical masses. Prior studies have been written on SMJN, but most have a limited number of patients, often reporting only one or two cases.
CT imaging has long been used to obtain images of patients’ internal structures. However, it does lack the ability to image small structures with detail. This can result in false-negative results. The most striking of these is that not all masses protruding through the abdominal wall are hernias.
This study was conducted to show that sonography, in conjunction with CT or alone, can evaluate soft tissue abdominal paraumbilical masses to determine if the suspected hernia is in fact a metastatic implant. The sonographic appearance of actual SMJNs was compared with that of other modalities. The study also evaluated the utility of sonography to accurately locate the SMJN for biopsy and determine whether the addition of sonographic imaging would have a positive impact differentiating a simple hernia from that of a metastatic mass.
Materials and Methods
This study was conducted starting in August 2003 on all patients with a solid mass herniating through the umbilicus or mass in the periumbilical region. The study was limited to patients who presented to the radiology department and had a CT and/or sonographic study performed. Patients with known umbilical hernias were excluded. When a suspected SMJN was seen in one modality, the records were searched for all previous imaging records that pertained to this condition. This extended the dates back to August 2000 and resulted in a total of 13 patients (male, n = 3; female, n = 10) evaluated retrospectively. The patients ranged in age from 57 to 89 with an average age of 71. Two new patients presented during the course of preparing the manuscript, and their data have been included in the analysis as well, giving a total of 15 (male, n = 4; female, n = 11). This extended the dates of the study from May 2000 to March 2011. The patients’ age range also increased, from 52 to 89 years, with a mean age of 72.
To comply with Health Insurance Portability and Accountability Act (HIPAA) regulations, approval for this study was obtained from the director of patient care services and the hospital radiology committee to perform this study. Approval was granted such that the author was the sole reviewer of the imaging and medical chart information. To ensure anonymity, all patient information was removed from the collected imaging files and chart data. A case study number was then assigned to each patient, eliminating all patient information from the compiled information.
Equipment
All sonographic examinations were performed by staff sonographers. All procedures were performed using available sonographic equipment, including the following: Acuson 128 XP/10 (Mountain View, California), Sequoia (Mountain View, California), GE LOGIQ 9 (General Electric, Waukesha, Wisconsin), and Phillips IU22 (Bothell, Washington). A high-frequency (7–12 MHz) broadband linear array transducer was used to obtain most of the superficial images. To obtain images from deeper structures, a lower frequency (3–5 MHz) curve linear transducer was used.
Procedure
Information was obtained from the review of the medical record and medical imaging studies of patients having a suspected umbilical lesion on either CT or sonographic studies. The CT and sonogram findings were separated into eight categories (Table 1).
Distribution of Primary Lesions to the Umbilical Region
In the CT findings category, only those with known history of cancer or imaging evidence of a lesion were included. In the sonographic category, only those suspicious for tumor were included. The medical records were reviewed for all patients with a suspected tumor on CT to determine if a sonogram was performed.
The location of the suspected SMJN was meticulously scanned with a broadband linear transducer using the highest frequency possible. When the lesion was large, it was necessary to use a curved linear transducer with a lower frequency to image the entire nodule. Normal gray-scale imaging along with color or power Doppler and tissue harmonics were used to better delineate the sonographic appearance of the nodule. Care was taken to vary the position and angle of the transducer while imaging in attempt to obtain the best image possible.
When CT images were available, they were reviewed to determine the general location of the nodule prior to sonographic imaging. This is especially helpful when external signs such as swelling or redness were not present. When suspected mesenteric implants were seen on CT, their location was determined and attempts were made to image them sonographically (Figure 1A,B).
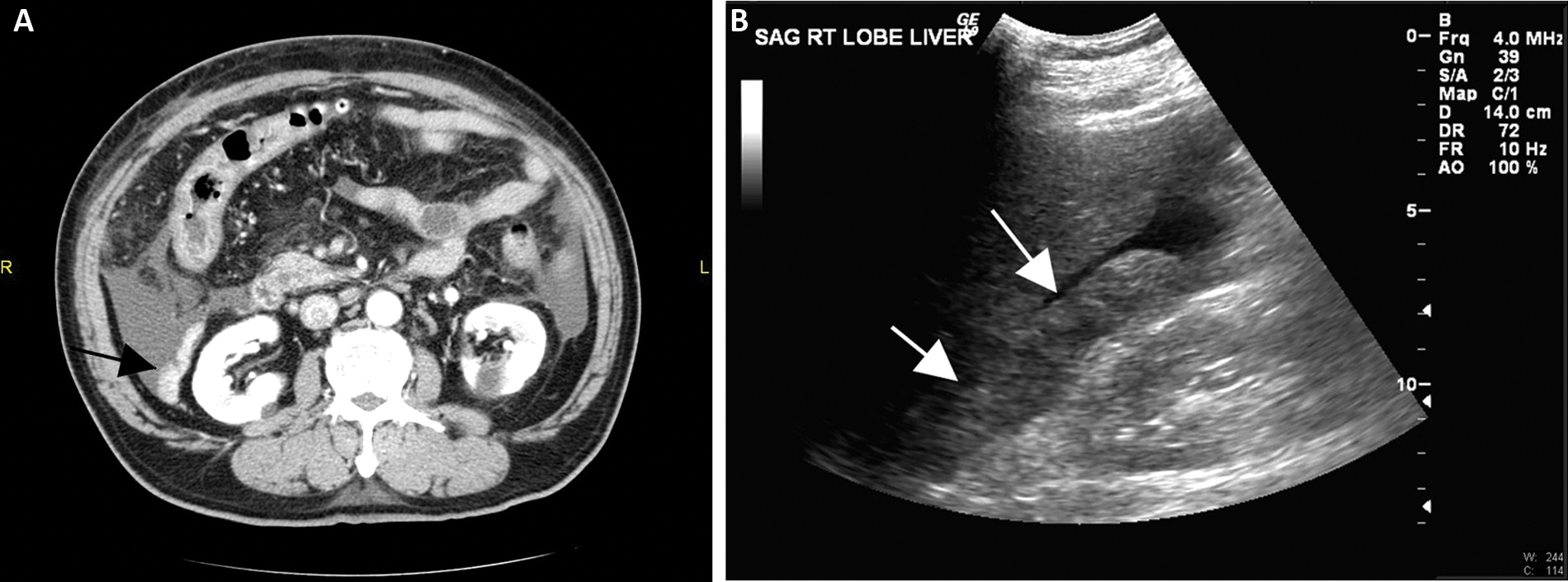
(A) Computed tomography image of a mesenteric implant adjacent to the right kidney. (B) Sonographic image of the same mesenteric implant located between the liver and right kidney.
Core biopsies were performed when possible to confirm the presence of a malignant metastasis. Fine-needle aspirations could also be performed, but this requires a cytopathologist; either method can provide results with minimal risk to the patient.1,2 When large intra-abdominal masses were present along with a suspected SMJN, only the superficial lesion was biopsied (five of six cases in this study). This decreased the risk of complications to the patient.
Results
Fifteen patients with a suspicious umbilical mass were found. There were 4 male and 11 female patients ranging in age from 52 to 89 years, with a mean age of 72 (Table 2). Of the 15 cases, all had CT imaging, whereas sonographic imaging was performed on 13. Six of the 15 had a biopsy performed on the nodule, and pathology results were available. Biopsies were not performed on the remainder for various reasons, including patient demise, known history of cancer and the family felt no need for the additional test, or the patient was transferred to hospice prior to biopsy.
Summary of All Patients in the Study
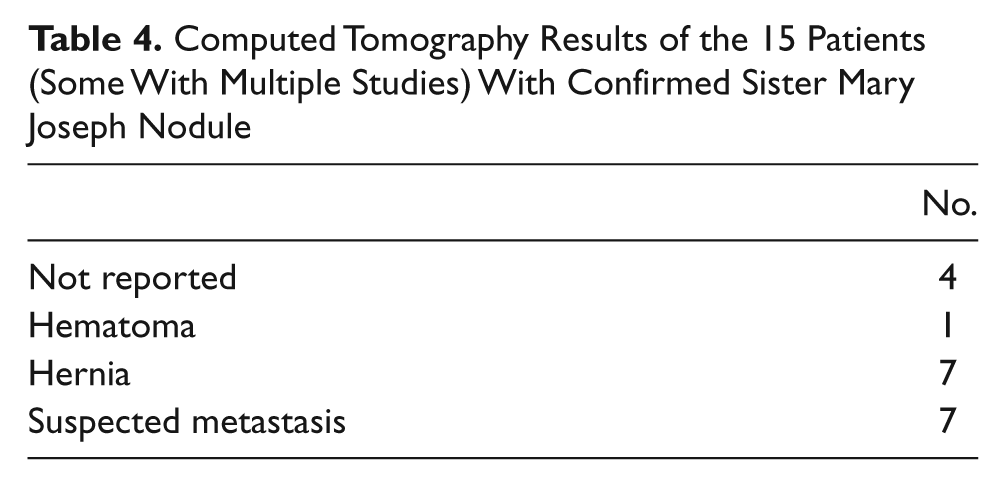
Sonograms were performed in 3 of the 15 cases as the first imaging modality. CT was obtained in 7 of the 15 cases as the first imaging modality and the only imaging modality in 2 cases. In the remaining 3 cases, CT and sonographic imaging were performed on the same day (Table 3). Thirteen of 15 patients had both sonogram and CT examinations performed. One patient not having sonography was transferred to another facility and lost to follow-up. The second patient who did not have sonography had a history of colon cancer; he elected to have no additional treatment and was transferred to hospice. Of the 15 patients in which CT was performed, seven CT scans were reported as simple hernia, four did not report the mass, and one was reported as likely/possible hematoma (Table 4). CT ultimately suggested a mass in 7 of the 15 patients. Of the 13 patients in whom a sonogram was performed, all were reported as a mass with biopsy performed or suggested.
Sequence and Number of Examinations Performed
Computed Tomography Results of the 15 Patients (Some With Multiple Studies) With Confirmed Sister Mary Joseph Nodule
Discussion
A Sister Mary Joseph nodule is a malignancy located in the periumbilical region. It often presents as a firm, indurated umbilical nodule. When present, it is associated with advanced metastatic cancer and generally indicates a poor prognosis. 3
Origin of the Name and Condition
The first published report of cancer involving the umbilicus was in 1846, 4 when the first case of umbilical metastasis originating from the stomach was reported. 5 The rarity of umbilical metastasis was later described by William J. Mayo of the Mayo Clinic in 1928, referring to it as a “pants-button umbilicus.” 6 In 1949, Sir Hamilton Bailey used the phrase “Sister Mary Joseph’s nodule” in his book Demonstrations of Physical Signs in Clinical Surgery to describe all metastatic lesions of the umbilicus, and this term remains in current use today.7,8
Sister Mary Joseph (1856–1939), born as Julia Demsey, 9 worked at St Mary’s Hospital in Rochester, Minnesota, beginning in 1889 and was made superintendent there in 1892. As a surgical assistant for Dr Mayo, Sister Mary Joseph was responsible for prepping patients scheduled for surgery. It was while performing this task she first identified the clinical signs that bear her name. She noted that some patients discovered to have diffuse intra-abdominal cancer at surgery had unusual nodules located around the umbilicus. 3
Anatomy and Circulation of the Umbilical Region
Embryologic Development
The umbilicus is a complex structure located on the abdominal wall between the peritoneum and transversalis fascia appearing as an invaginated scar. After birth, the fetal umbilical cord structures develop into ligaments or peritoneum folds. The median umbilical ligament results from the obliterated urachus. The umbilical arteries become the medial umbilical ligaments, and the left umbilical vein becomes the ligamentum teres continuing on to form the falciform ligament in the liver. Inferior epigastric vessels and, sometimes, a vestigial vitelline duct connecting the umbilicus to the ileum can be recognized on the lateral umbilical folds. 10
Arterial Circulation
The umbilical region shows a rich arterial supply that includes the inferior epigastric and deep circumflex iliac branches of the external iliac artery, as well as the superior epigastric branch of the internal mammary artery.10–15
Venous Circulation
A network of vessels that drain to three main regions accomplishes venous drainage from the umbilical region. The superficial epigastric vein drains caudally into the femoral vein. The internal mammary veins accept a network of small vessels and continue cranially, emptying into the axillary vein.11–15 Finally, small veins are connected to the portal system by way of the ligamentum teres. 10
Lymphatic System
Lymphatic drainage of the umbilical region often follows the venous system. The lymphatic system drains the umbilical region to the axillary, inguinal, and para-aortic lymph nodes. It can be further separated into superficial and deep systems. The superficial system connects and drains into the axillary nodes from above the umbilicus and the inguinal nodes from below the umbilicus. The deeper lymphatic network connects to and drains into the internal thoracic nodes and courses to the nodes around the external iliac arteries and/or abdominal para-aortic nodes. Other branches pass along the falciform ligament, piercing the diaphragm and entering the anterior mediastinum.16–19
Ligaments that connect with the umbilicus are remnants from embryologic development. These include the ligamentum teres and median umbilical ligament. The remnant of the vitelline duct, which connected the yolk sac to the midgut, is sometimes present connecting the umbilicus to the ileum. It is this vast network of arterial, venous, lymphatic communications as well as ligamental attachments that results in metastasis to the umbilical region and may account for the variety of cancers that metastasize to this region.11,16
Physical Examination Findings
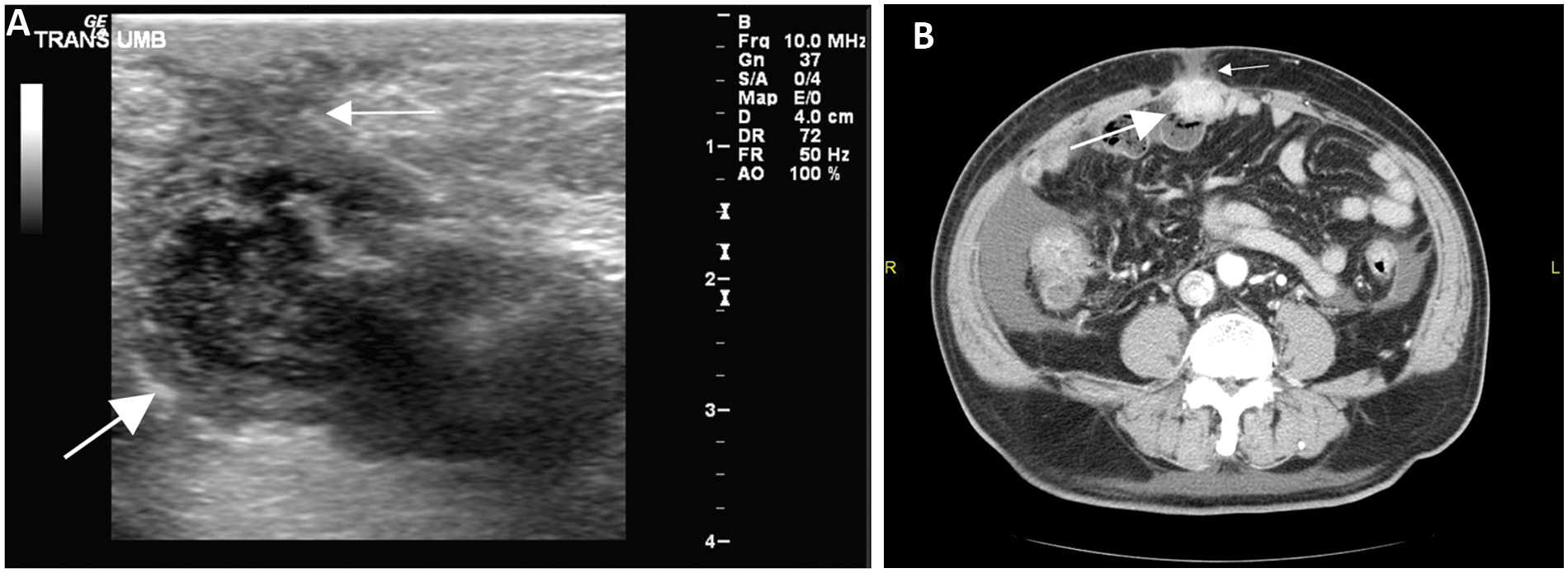
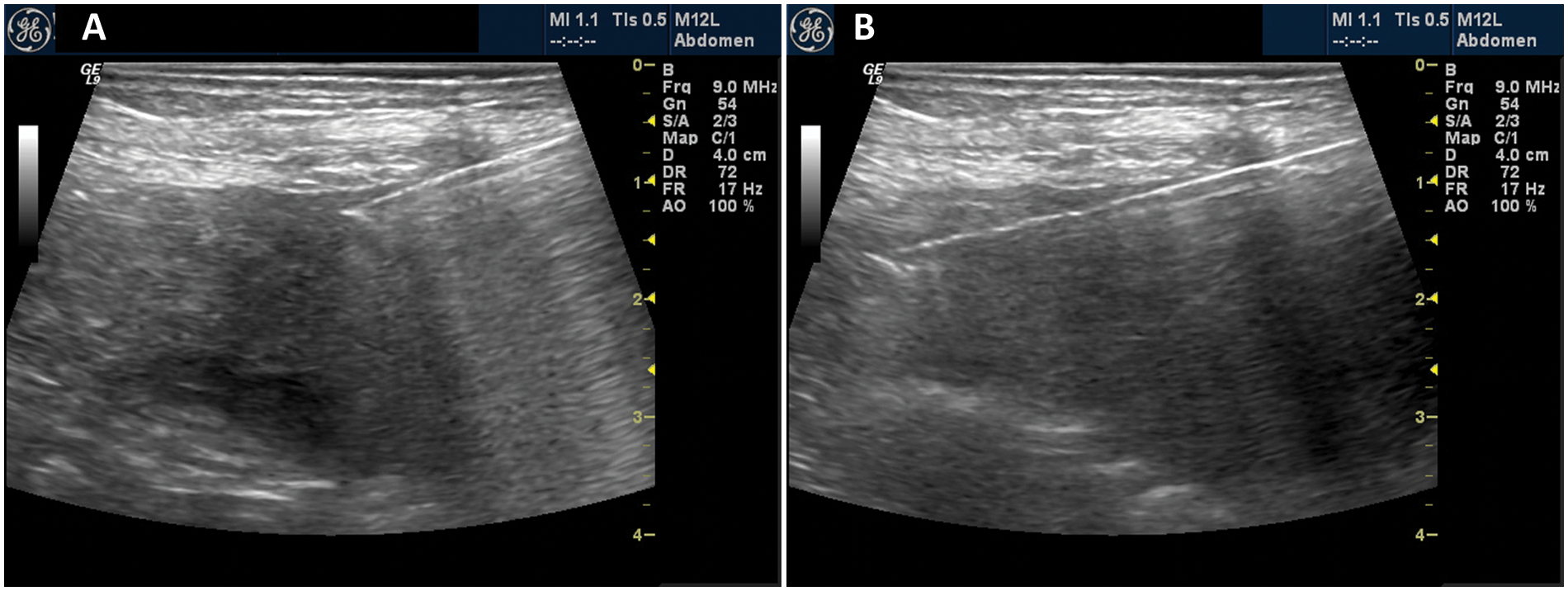
A palpable periumbilical nodule may be the earliest clinical manifestation of an underlying malignancy. 11 During the initial abdominal sonogram for occult malignancy that led to this study, the sonographer’s arm brushed across the region of the umbilicus and noted a hard nodule. Thinking this was a simple hernia, the sonographer then obtained images of the umbilical region (Figure 2). A firm, highly vascular mass was noted and a subsequent biopsy determined it to be a rare malignant mesothelioma.
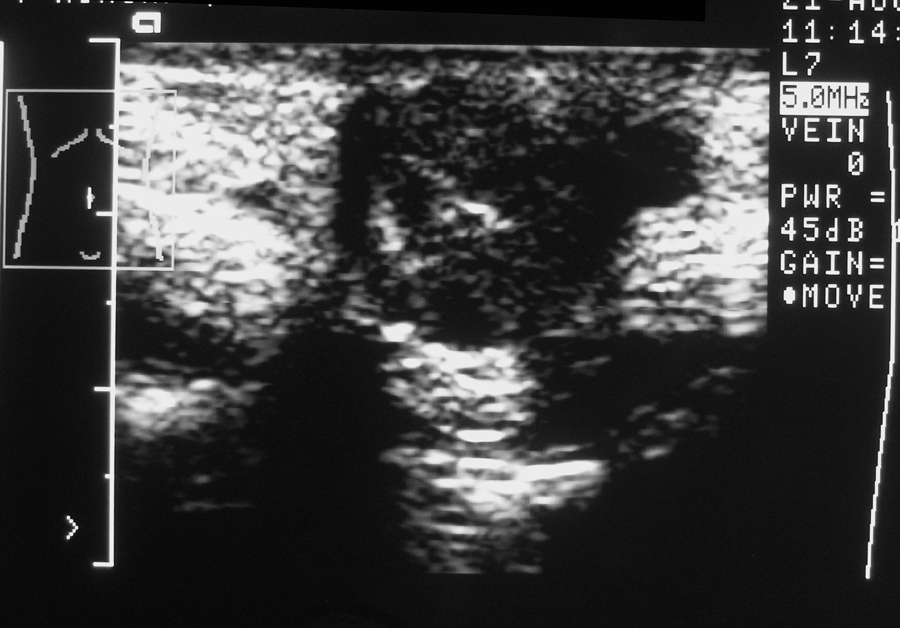
Image of firm periumbilical nodule found while performing routine abdominal imaging.
Although a firm nodule is the most common physical finding, SMJN may also present as skin-fold thickening or inflammation of overlying skin resembling the appearance of cellulitis (Figure 3). The nodule is usually irregular and painless when palpated. The region may appear fissured and ulcerated.3,20 The nodule may appear white, bluish violet, or brownish red. 21 A bloody, mucinous, serous, or purulent discharge may also be present.12,13 It is typically less than 5 cm in diameter but occasionally enlarges enough to form a protruding tumor. 9
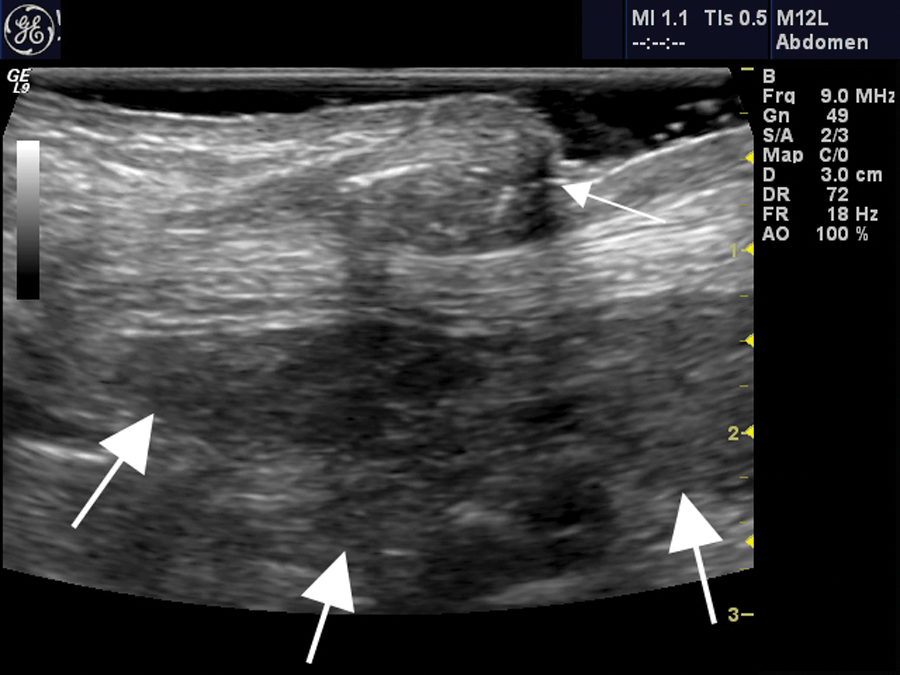
Note the distinct fold skin-fold thickening that, on physical examination, resembled the appearance of cellulitis (small arrow). The large arrows represent the peritoneal implants adjacent to the umbilicus in this patient with adenocarcinoma consistent with an origin from the pancreatic or biliary system.
Fill et al 14 reported a case in which the patient noticed a red, pressure-sensitive lesion with a diameter of 2 cm on her umbilicus. No additional investigation of the lesion was performed, believing it to be harmless. Twenty-four weeks later, the enlarging lesion was finally diagnosed as metastatic gastric cancer. This is similar to the seminal case in this study in which a surgeon diagnosed a small umbilical hernia that was later determined to be a metastatic lesion.
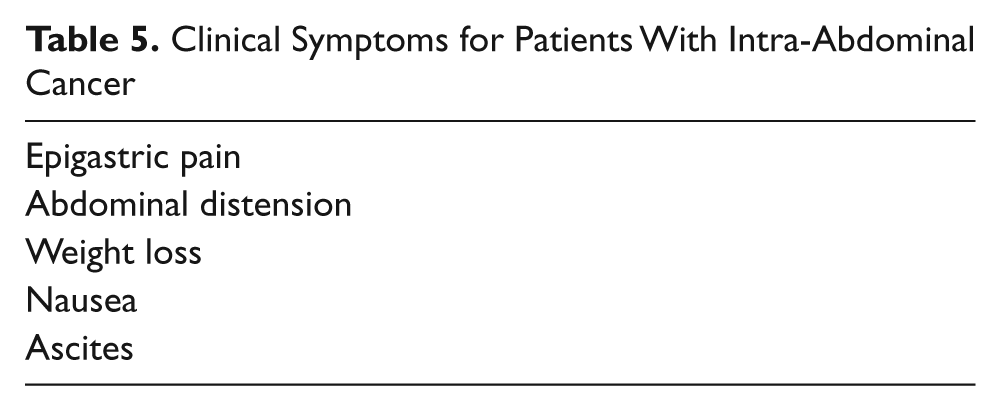
Although these findings may be evident on routine physical examination, they can easily be overlooked in mild or severely obese patients. 20 In some patients, however, there may be no other clinical signs or symptoms for cancer other than the metastatic umbilical nodule (Table 5). 9
Clinical Symptoms for Patients With Intra-Abdominal Cancer
Primary Sources
Of all the umbilical tumors, 57% are benign and 43% malignant, of which 83% are metastatic lesions. 3 Most cases are metastatic adenocarcinoma. The more common primary sites are from the gastrointestinal tract and female reproductive sites. 22 Umbilicus invasion by mesothelioma is rare, with only one reported case of peritoneal mesothelioma presenting as an umbilical tumor. 15
Other authors have reported that if these nodules are secondary tumor deposits, then the source of the primary tumor may be from the gastrointestinal (35%–65%) and genitourinary (12%–35%) tracts. In 3% to 6% of cases, it may originate from hematological malignancies or lung and breast cancers. Some authors also have reported that the primary site for the SMJN was unknown in 15% to 30% of patients.20,23,24
In an extensive literature review, Shetty 25 found 265 reported cases of SMJN from 1830 to 1989. Stomach cancer accounted for the highest percentage (25%). An extensive list of other primary sources was also determined (Table 6). Other authors have reported similar findings.1,26 In a review of the literature, lymphoma rarely presented with deposits in the umbilical area, and mesothelioma presenting as SMJN is extremely rare.22,27 However, this study includes both of these rare findings. The first was a 52-year-old male patient with diffuse large B cell lymphoma diagnosed by core biopsy. A subsequent therapeutic paracentesis demonstrated chylous ascites (Figure 4). The second case, a mesothelioma, was the seminal case that inspired this study. Authors have described the incident of peritoneal mesothelioma to be only one to two cases per million with calcific concretions (psammoma bodies) seen in approximately 30% of these tumors.28,29 Boyde and Attanoos 30 “reviewed post mortem reports over a 24 year period from the Office of the United Kingdom’s Health and Safety Executive Register, and identified only three cases of malignant peritoneal mesothelioma that had presented with unrelated symptoms or with symptoms attributable to an umbilical nodule.”

(A) Chylous ascites (large arrow) adjacent to a mesenteric component of a Sister Mary Joseph nodule. Also note the direct extension from the mesenteric mass through the umbilicus enlarging to the subcutaneous mass (small arrows). (B) Large subcutaneous umbilical mass demonstrating color flow. Later biopsy revealed the mass to be metastatic mesothelioma. (C) Computed tomography image of the mesothelioma first reported as a hernia.
In Shetty’s review, 25 the primary site was unknown in 20% of cases. This is consistent with other authors who have reported an unknown primary site ranging from 20% to 30%.1,26 Of the 15 cases in this study, 2 had unknown primary sites (13%). However, in both cases, the family or patient elected not to have a biopsy performed. In one case, the family transferred the patient to a hospice because they did not want to subject her to an invasive procedure due to her grave condition. The second patient was transferred to another facility where a biopsy was not performed. In each of these cases, the patient had a history of cancer, so it was felt that a biopsy was unnecessary. This decision not to obtain a tissue diagnosis may be why other authors have reported a high incidence of unknown primary site.
Routes of Metastasis
In most cases of SMJN, the route of metastasis is unclear. 2 However, the most common routes for metastatic lesions involving the umbilicus area are thought to be arterial circulation, venous circulation, or direct extension. 15 Lymphatic spread also occurs through one of four sets of lymphatic ducts that pass through this region. 3
Direct extension is believed to occur from ligaments of embryonic origin: the median umbilical ligament of the urachus, the vitellointestinal duct remnant, the obliterated vitelline artery, and the round ligament of the liver. 24 Powell et al 31 believed that the contiguous extension from the anterior peritoneal surface is probably the most important route of umbilical metastases (Figure 5). Other authors agree that metastatic seeding to the umbilical region is most likely the result of direct extension or contiguous spread. 13
(A) Paraumbilical mass proven to be metastatic lung cancer. Note the mesenteric component of the mass (large arrow) extending through the umbilical region to the subcutaneous fascia (small arrow). (B) Computed tomography image of the same mass demonstrating contrast enhancement of the mesenteric component of the mass (large arrow) as well as its extension through the umbilical region to the subcutaneous fascia (small arrow).
Direct extension of the tumor through the peritoneum is thought to be the preferred route for gastrointestinal tumors. 10 For female reproductive systems, however, hematogenous, venous, and lymphatic spread all represent mechanisms of tumor metastasis.18,32
Gender Distribution
If SMJN is present in a male patient, the most common site of the primary neoplasm is from the gastrointestinal tract (55%), followed by stomach, colon, rectum, small bowel, and pancreas.31,33–36
In females, however, gynecological neoplasms are the most common primary site, of which serous papillary cystadenocarcinoma (34%) is the most frequent, followed by endometrial and cervical carcinoma.31,36
Diagnosis
To determine the root cause of an umbilical mass, physicians have used various imaging modalities, including sonograms, CT, and magnetic resonance imaging (MRI).
MRI has been used, but its high cost and limited availability in some facilities may prohibit its routine use. CT imaging is often the first modality used to evaluate this lesion as it provides a global look within the body. The disadvantage to CT is increased radiation exposure to the patient.
Sonography has been shown to be efficacious and less expensive than CT imaging and lacks the problem of radiation exposure. High-resolution sonographic imaging helps to clarify the clinical findings. It is able to demonstrate solid umbilical nodules even when clinical diagnosis is difficult. 10 The widespread availability and low cost of sonographic equipment make it a good choice for determining the presence of SMJN. Another advantage is the ability to dynamically observe the needle throughout any biopsy process.
Sonographic Identification
Review of prior imaging results can assist the sonographer in targeting the specific region to image. Review of the CT images can provide the sonographer with a detailed roadmap as to where to start the imaging process. It can also demonstrate possible peritoneal implants that should be evaluated (Figure 6). A review of the patient’s chart should be helpful to determine if there was any history of cancer, pertinent laboratory tests (tumor marker studies), and recent physical examinations (Table 7).
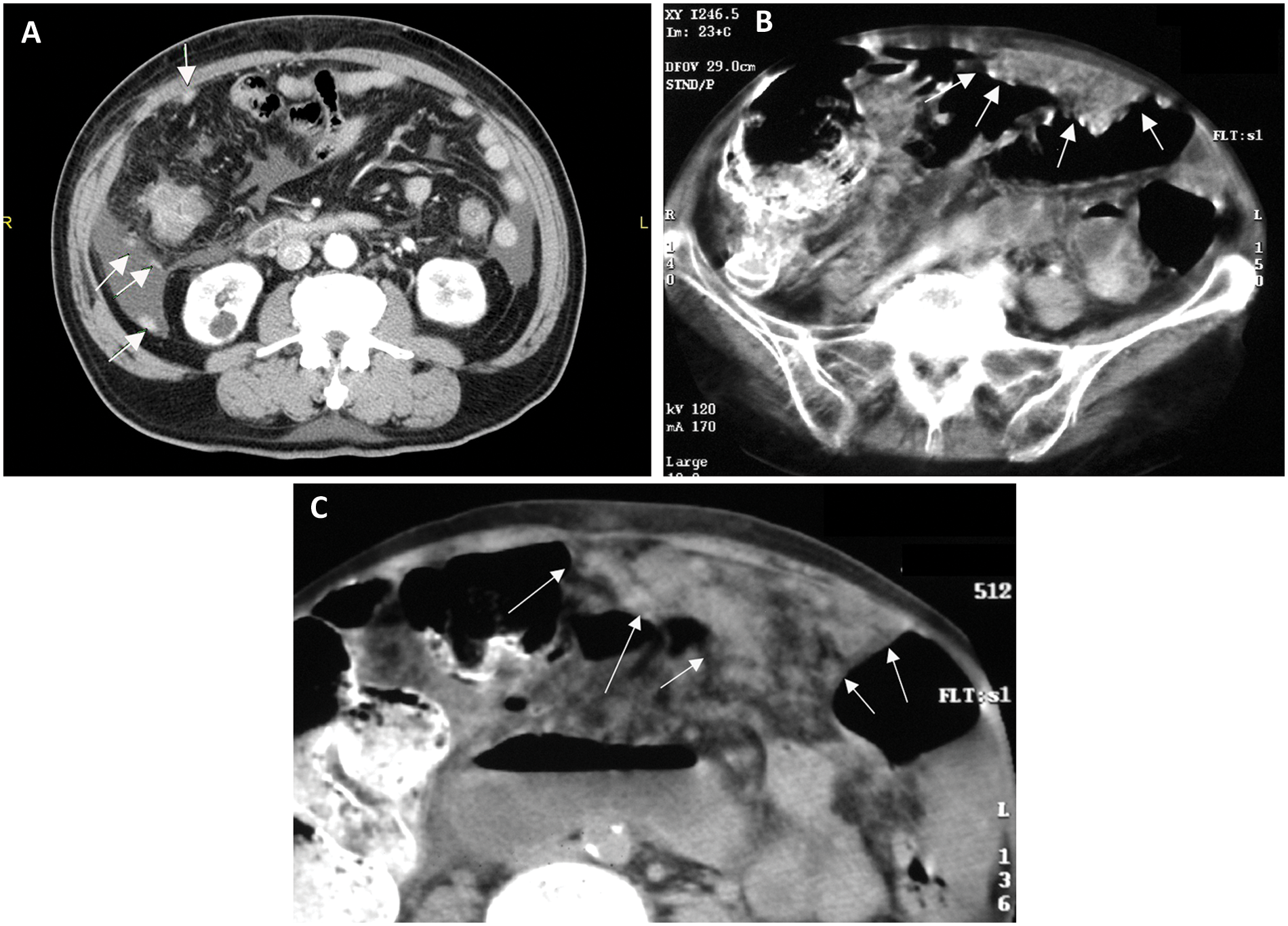
(A) Computed tomography image demonstrating multiple small metastatic implants (arrows). (B) Note the thickened anterior abdominal wall from mesenteric implants. (C) Enlarged view of the anterior abdominal wall demonstrating the mesenteric implants.
Common Blood Tests Used to Diagnose Cancer Types 18
Current Technology
As new equipment became available during this study, improved image quality and resolution were obtained because of the availability of higher frequency transducers. Improvements were also observed using tissue harmonics, speckle reduction, and crossbeam imaging. Along with higher frequency, the improved color Doppler and power Doppler capabilities were helpful in evaluating the vascularity of these lesions. All of these options provided an improvement over normal imaging parameters and, on most occasions, improved their resolution.
Biopsy Methods and Imaging Modalities: Localization
Although imaging may suggest the presence of a cancerous lesion in the periumbilical umbilicus, a biopsy is required for a definitive diagnosis. This can be obtained safely through a fine-needle aspiration (FNA) or core biopsy and can expedite patient management.
FNA is a rapid, cost-effective diagnostic method that can minimize unnecessary surgery and obtain a definitive diagnosis.1,2 Fleming and Oertel 2 performed 20,000 aspirations, with 8 involving umbilical malignancies. There were no complications even when the needle penetrated the intestinal wall. Although this supports the use of FNA for diagnosis, it requires the availability of a cytopathologist.
Like FNA, core biopsies are a rapid, cost-effective method that can minimize unnecessary surgery and provide a definitive diagnosis. 1 Often these types of biopsies are obtained with imaging guidance. CT guidance can be used with good results. Sonographic guidance performs equally as well but at a lower cost and without the radiation risk. A distinct advantage with sonographic guidance is the ability to watch the needle in real time as it enters the lesion and throughout the biopsy process (Figure 7A,B).
(A) Image of a patient with metastatic pancreatic cancer to the umbilicus demonstrating the biopsy needle inserted into the mass. (B) Needle position immediately after the biopsy was obtained, confirming that the entire specimen was within the lesion.
Clinical Significance
The presence of SMJN usually indicates widespread disease and is associated with a poor prognosis and complex therapeutic implications.7,8,37 Fleming and Oertel 2 reported on eight cases in which the average survival was 10 to 11 months after diagnosis. Ishrat et al 38 reported that after a positive histologic diagnosis of metastatic carcinoma (from SMJN), the mean survival time was 10 months, 38 and many other authors have reported similar results.12,21,23,39–43
Management of these cases is controversial, with some clinicians advocating aggressive surgery and adjuvant therapy.21,26,35 Recent studies have demonstrated that there is a better survival (21 months) for patients if they are treated with a combination of surgery and adjuvant therapy instead of surgery alone (7.4 months) or chemotherapy alone (10.3 months).18,23,27,43 Despite increasing patient survival by 11 to 13 months, some authors still propose only palliative treatment because of the poor long-term prognosis.12,20,44
Early diagnosis is imperative for successful cancer treatment. With SMJN, however, patients are often asymptomatic, resulting in a delay in their diagnosis. Maconi et al 39 have reported a mean delay, from first symptoms to final diagnosis, of 29 weeks in young patients without significant symptoms. Often patients with gastric cancer are asymptomatic in its early stage. Koh et al 40 reported initial delayed diagnosis in patients with early stage gastric cancer because as many as 80% were asymptomatic.
In this study, 7 of the 15 patients had a delay in diagnosis because the initial CT scan reported the SMJN as a simple hernia. There was only a one-day delay in 5 patients. With 2 patients, however, the delays in diagnosis were 8 and 12 months, respectively.
Limitations
Sonography can be very effective in evaluating a patient for the presence of an umbilical hernia. However, there are some limitations in distinguishing it from a metastatic SMJN.
One limitation is the knowledge and experience of the operator. Many sonographers equate all umbilical protrusions as a hernia. With proper understanding of this condition, SMJN when imaged can readily be differentiated from that of a hernia. Reviewing the patient’s records for a history of cancer can be helpful to differentiate SMJN from a hernia. With positive laboratory (tumor markers) results, SMJN should also be suspected.
The second limitation is persevering to make a definitive diagnosis. In case 1 of this series, the surgeon refused to do a surgical biopsy on the patient because he felt it was a hernia and of no significance. Both sonography and CT imaging demonstrated the mass. However, the physicians failed to see it as a potential SMJN. It was not until the patient was transferred to another facility that the biopsy was performed, confirming it to be a malignant SMJN. Had it not been for the insistence of a gastroenterologist, this too would have been missed.
The final limitation is the low number of documented SMJN (15 cases over a 10-year period) in this report. However, in an extensive literature review conducted for SMJN, Shetty 25 found 265 reported cases from 1830 to 1989. This at least raises the question that if at one small community hospital, 15 documented cases can be found, why is the reported number so low?
Summary
A Sister Mary Joseph nodule may be the first or only indication of an underlying occult cancer. It can indicate recurrence of previously treated malignancy. The mere presence of SMJN suggests an advanced metastatic process characterized by poor prognosis.7,37 Diagnosis is often delayed, with clinicians treating them as a simple hernia or other condition. In this series of 15 patients, a total of 20 CT scans were performed. Seven were reported as a simple hernia, and four masses were not reported at all. The literature reports cases masquerading as umbilical hernias finally turning out to be metastatic deposits. 41 Thus, although the literature reports SMJN to be rather rare, it may be more common than previously reported due to misdiagnosis.
Histology of the metastatic umbilical tumor usually reveals adenocarcinoma, but rare reports of umbilical metastasis from sarcomas, mesotheliomas, and melanomas have also been seen.3,27,42 The inability to locate the primary site has been reported to be as high as 30%. 26 If SMJN is suspected, an FNA or core biopsy can be performed to obtain definitive diagnosis.1,2 In most cases of SMJN, the route of metastasis is unclear. 2 However, the most common routes include direct extension from ligamental attachments, arterial or venous circulation, or through one of four sets of lymphatic sites that pass through this region.3,15 A firm nodule is the most common physical finding.3,11
Footnotes
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author received no financial support for the research, authorship, and/or publication of this article.