
Abstract
On January 24, 2009, newly sworn-in President Obama uttered a bold promise: “To lower health care cost, cut medical errors, and improve care, we’ll computerize the nation’s health records in five years, saving billions of dollars in health care costs and countless lives” (http://www.healthmu.org/radiology/index.php). It’s those words that marked the beginning of health care reform. In February 2009, the American Recovery and Reinvestment Act was passed. Within this bill was the HITECH (Health Information Technology for Economic and Clinical Health) Act. With it came a large number of dollars to incentivize the move toward electronic health records and the use of health information technology. The Continuing Extension Act of 2010 included language that removed outpatient from the hospital-based category in terms of the fee schedule that Medicare uses to determine the place of service. This moved most interpreting physicians into the eligible professional category. Along with moving interpreting physicians into the eligible professional category, these bills have affected the future role of the sonographer. Sonographers will be required to increase their responsibilities in delivering health care to aid the interpreting physicians to meet meaningful use measures.
There is a shift beginning in the paradigm of health care that will continually redefine the role of the sonographer for many years to come. Health care reform is presenting new regulations that are redefining the roles of health care workers, including sonographers. The health care industry is rapidly taking on a new face. Sonographers must be willing to adapt to change not only in the industry but also in their work environment. One area that will bring changes to the role of the sonographer is meaningful use.
Meaningful use regulations are based on rulings of the Office of the National Coordinator for Health Information Technology (ONC for HIT) and Centers for Medicare & Medicaid Services (CMS), which are both part of the U.S. Department of Health and Human Services (DHHS), the federal agency that oversees meaningful use. The CMS regulates providers or eligible professionals. The ONC for HIT regulates technology and has set the rules for the criteria that vendors need to meet to have their software comply with meaningful use (see Figure 1).
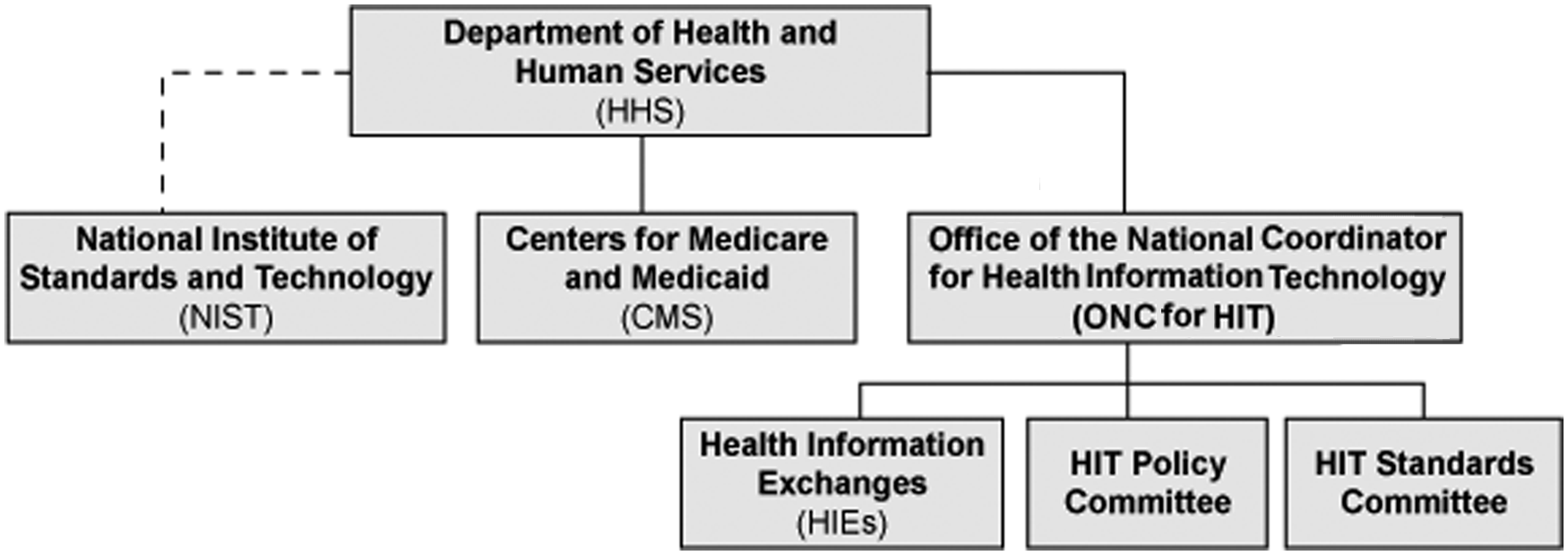
Department of Health and Human Services and related organizations.
The ONC is responsible for coordinating with the Department of Commerce’s National Institute of Standards and Technology (NIST) on the specifications for the Nationwide Health Information Network standards.
The HIT Policy and HIT Standards Committees are the working groups that advise the ONC on what to put in the standards.
The NIST is responsible for coming up with the test materials (assertions, procedures, methods, tools, data, etc.) that will be used to certify working systems. 1
These two agencies set criteria and objectives for meaningful use in three stages. “Stage 1 focuses on standardizing the format of captured health information, tracking key clinical conditions, communicating information, implementing clinical decision support tools, and reporting clinical quality measures and public health information.” 2 Stage 2, which takes effect in 2013, focuses on continuing quality improvement and structured information exchange. Stage 3 further promotes improvements in quality, safety, and efficiency, including decision support for national high-priority conditions, as well as patient self-management tools, access to comprehensive patient data, and population health improvement. 2
The American College of Radiology (ACR), in conjunction with the Radiological Society of North America, the American Board of Radiology, and the Society for Imaging Informatics in Medicine, submitted a collective response to each of the meaningful use criteria and proposed a set of unique radiology-centric criteria that encompasses functionality applicable to eligible interpreting physicians. The proposed criteria focused on six key areas that harmonize with current radiology information technology (IT) practices: physician order entry, decision support, image management, image interpretation, communication management, and quality and safety. This collective response emphasized areas in which radiology has particular domain expertise (order entry, decision support, and image sharing). 3
With many interpreting physicians moving toward compliance of meaningful use to take advantage of the incentives and avoid financial penalties, the role of the sonographer will be redefined. No longer will sonographers be responsible for just performing sonograms. They will potentially be responsible for a more in-depth history-taking process, tracking multiple items in the patient’s continuum of care, as well as reports regarding patient testing and outcomes, just to name a few.
So what does this mean for sonographers? Diagnoses and/or an indication that no clinical problems have been identified for the patient need to be tracked for 80% of the patients seen. This fulfills the requirement of two core measures. 4 Since the sonographer is typically the first medical professional who comes in contact with the patient after registration, this information will become his or her responsibility. History taking will soon take on a more important role as physicians, group practices, and hospitals strive to comply with meaningful use.
For example, when a patient enters the examination room, sonographers will no longer just be asked to verify patient identification and confirm the indication for the study. They will have the added responsibility to document any allergies, record and chart vital signs such as blood pressure, document smoking status, and document any recent laboratory results that are available. They will be required to record demographics such as preferred language, gender, race, ethnicity, and date of birth.
For sonograms with a recommendation for follow-up visits, such as breast, thyroid, liver masses, and kidney cysts, and preventive screenings such as for the abdominal aorta, a patient reminder letter must be generated and sent. Sonographers will most likely become responsible for using their Radiology–Hospital Information Systems (R-HIS/PACS) to send these patient reminders. They will also have to keep a closer watch on examinations that are not dictated within a timely manner since a requirement will be that at least 10% of patients are provided with timely electronic access to their health information such as radiology reports. Sonographers will be responsible for providing patient-specific educational resources to at least 10% of the patients, as determined by the interpreting physician. Patients have the right to request a summary-of-care record for their visit(s), which could be paper based, by DICOM CD/DVD, or by direct electronic transfer to another physician that the patient may see. 4
All of these measures are time-consuming and will significantly add to the nonimaging responsibilities of the sonographer. Scheduled examination times will have to be lengthened to compensate for the additional history taking and education of the patient. If a sonography department does not employ an imaging associate or the equivalent, it will become the sonographer’s responsibility to prepare the summary-of-care information for the patient.
If sonography departments are to stay profitable and continue to run efficiently, a closer look at the new role of the sonographer with regard to meaningful use and clinical workflow will be necessary. Not only will additional training be needed in new software systems that meet the meaningful use criteria, but also education in time management, history taking, and workflow will have to be implemented and monitored.
Before one takes a totally negative approach to all of this mandated documentation, one should keep in mind that implementing these measures will provide the collection of more clinical data. Ultimately, this will improve overall patient care as well as medical imaging billing performance because reimbursement is often tied to documented clinical indications, not the “rule-out” type indication that interpreting physicians often receive in their current practices. 2
The CMS set forth 25 measures and objectives to determine meaningful use compliance. However, because of the efforts of the ACR and other affected medical organizations, the CMS has decided that exclusion criteria can be involved with both the core set, of which there are 15, and the menu set, of which there are 10. The menu set has always been 5 out of 10, so 5 are always optional. Looking at the exclusions within both sets, interpreting physicians are now excluded for up to 14 of the 25 measures.4,5
The ONC has 33 criteria to determine certified technology, of which 25 are functional and 8 are privacy and security issues. Currently, any technology that is certified must meet all 33 criteria. There is some flexibility in terms of modular certification. The stance that the ACR has taken is that since radiology is mostly excluded from much of the required criteria, it is not necessary to implement but only “possess” certified electronic health record (EHR) technology. Much of the current R-HIS/PACS software will already track the necessary criteria that radiologists are not excluded from.4,5
R-HIS/PACS systems can be either modular (meets any single criterion or multiple criteria) or completely certified. It is permissible to combine modular certified products to achieve meaningful use. If your practice setting uses modular certified products, one needs to be certain that they cover your meaningful use measures requirements. If the EHR module approach is selected, a certified radiology health care IT product would include a list of all medications being taken by a patient, confirmation that drug-drug and drug-allergy interactions have been checked, and there is a field for known medication allergies of a patient. 5 This would meet three of the core requirements. Although many R-HIS software programs have the capability of tracking this information, they have not yet received certification.
Participating interpreting physicians will need to implement and track at least one clinical decision support rule. Interpreting physicians can define any clinical decision support rule to track and meet this requirement. They will also need to test the exchange of “key clinical information” with other health care providers. The final rule gives interpreting physicians the authority to define which clinical information is considered “key.” 4 Proof of maintaining secure data by conducting security risk analyses and implementing security updates is required.
The criteria of eligibility have been redefined so that the majority of interpreting physicians now qualify to participate in the incentive program. Unless their practice is over 90% inpatient and emergency department, interpreting physicians are considered an eligible professional (EP) according to the Continuing Extension Act of 2010. This places most interpreting physicians into the EP category. “CMS estimates that 86% of all Medicare participating physicians will now be eligible under the new criteria.” 6
Meaningful use compliance will be rewarded through a graded payment scale. If the measures and criteria are adopted by October 2012, interpreting physicians will be able to collect the total incentives over a 5-year period, which amounts to $44,000. But if they have not complied by 2012, each year they delay, their potential incentives decrease. By 2015, noncompliance begins to incur penalties. One major key is that only 90 consecutive days of use are required in the first year.
If sonography is to remain marketable and competitive with other radiology modalities, all of this will require that a new mind-set to be adopted. As reimbursement becomes more difficult to obtain, the field of sonography, sonographers, and interpreting physicians all have the golden opportunity to capitalize on its cost-efficient examinations. There are many new areas of sonography being developed and enhanced, such as musculoskeletal, sonography of the cancer patient, breast screening, preventive vascular screenings (carotid artery disease, aorta), and in-depth thyroid sonograms, to name a few. New technologies have also been developed by many of the sonography equipment manufacturers, such as elastography, contrast-enhanced sonography, 3D-4D sonography, and improved transducers that help to provide better diagnostic examinations. Interpreting physicians and sonographers who take a positive approach to these changes, despite increased workflow and responsibilities, will remain competitive and marketable and have a better chance of surviving in this era of health care reform.
Footnotes
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author received no financial support for the research, authorship, and/or publication of this article.