
Abstract
Nonalcoholic fatty liver disease (NAFLD) is an accumulation of extra fat in the liver cells not caused by alcohol consumption. This disease is an increasingly common condition and the most common cause of abnormal liver function tests among adults. NAFLD is an array of liver diseases ranging from simple hepatic steatosis (fatty liver) to nonalcoholic steatohepatitis (NASH). A liver biopsy is the gold standard for determining hepatic fat content and staging fibrosis. However, the invasiveness of this approach can be a contraindication in certain patients. Noninvasive imaging modalities such as ultrasound, computed tomography (CT), and magnetic resonance (MR) can also detect hepatic fat content.
Case Description
A male patient in his mid-60s presented to his primary care physician for a yearly preventative screening. The patient’s medical history included hypertension and type 2 diabetes mellitus. A computed tomography (CT) scan performed five years prior showed a liver low in attenuation, compatible with fatty infiltration. A complete screening abdominal sonogram was ordered.
Sonographic images were acquired with a Phillips iU22 (Bothell, Washington) sonography system using a C5-2 transducer. The liver was documented to have a markedly atypical echotexture with serpiginous hypodense areas throughout the parenchyma (Figures 1–3). Blood tests revealed normal liver functions and a normal white blood cell count. Because of the abnormal liver appearance on sonography, a CT was ordered five days later for further evaluation. Follow-up CT revealed a slightly fatty liver (Figure 4). Because of the grossly abnormal liver appearance on the sonogram, a follow-up sonogram was performed two months later, and images demonstrated no change in the liver parenchyma when compared to the prior sonogram (Figures 5 and 6). The same day, magnetic resonance (MR) revealed a signal intensity of the liver to be very minimally heterogeneous on the in-phase images (Figure 7). On the out-of-phase images where fat signal intensity should drop out, the liver became much more heterogeneous, therefore confirming the very abnormal echotexture by sonography and being consistent with abnormal serpiginous fatty infiltration (Figure 8). Imaging results were discussed with the patient immediately following the examinations, and the patient was recommended for a six-month follow-up.

Longitudinal sonographic image of the left lobe of the liver.

Transverse sonographic image of the right lobe of the liver.

Longitudinal sonographic image of the right lobe of the liver.
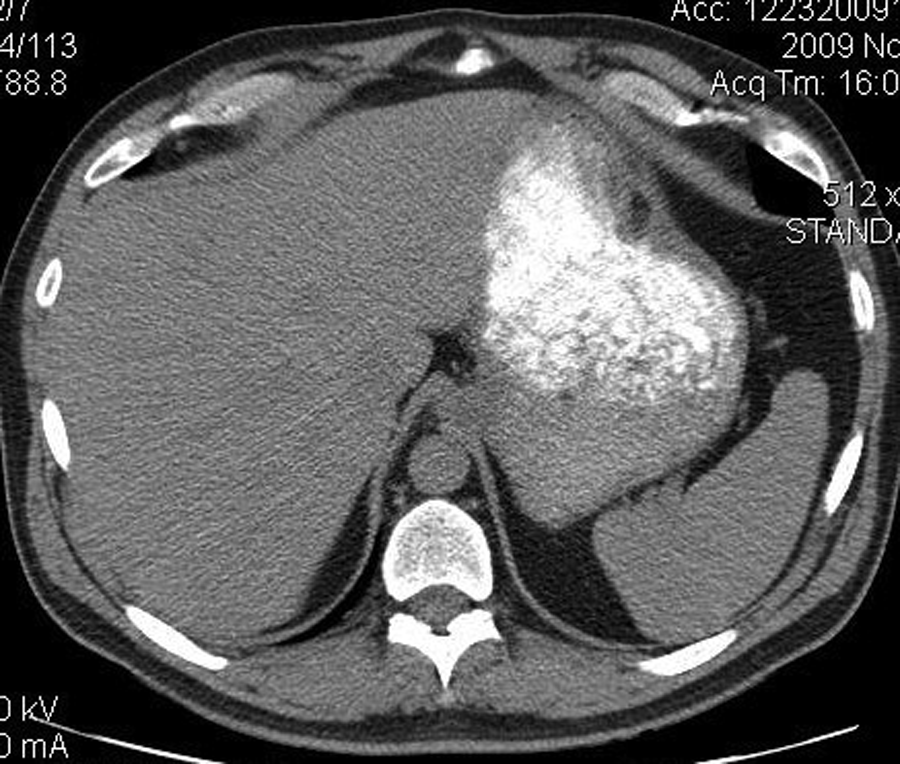
Noncontrast coronal computed tomography image through the liver.
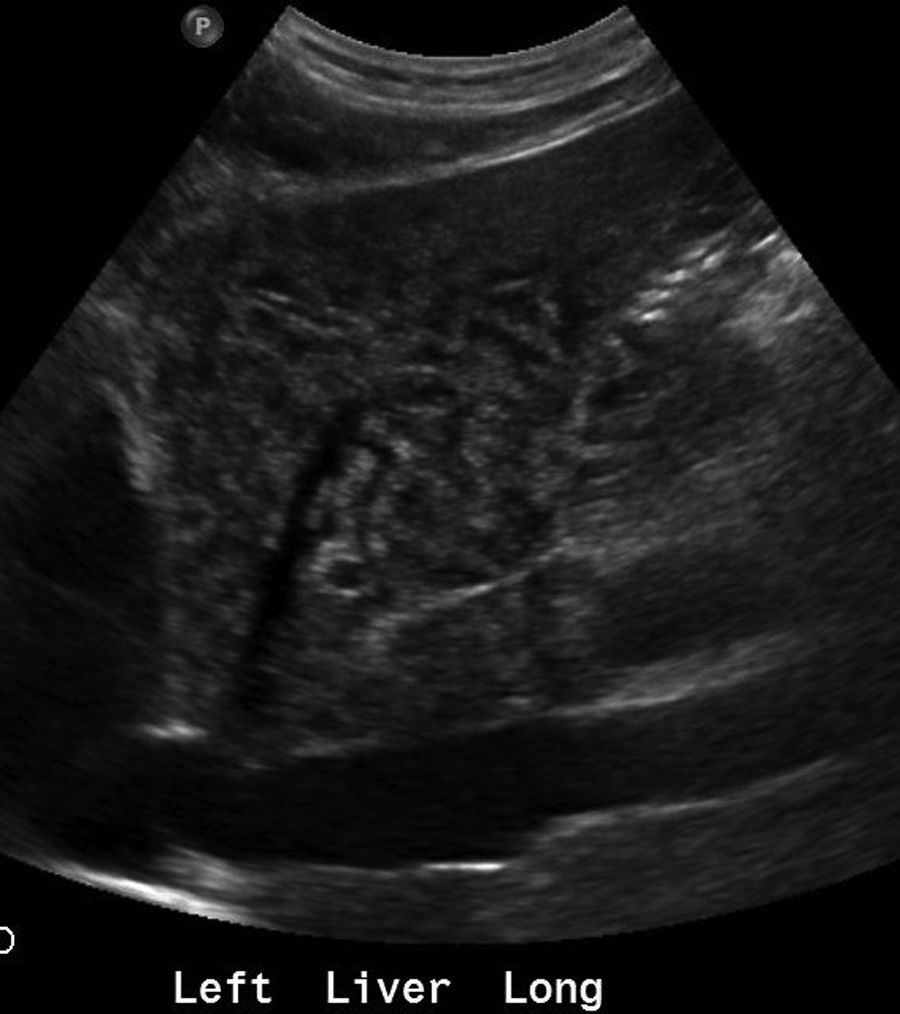
Longitudinal sonographic image of the left lobe of the liver.

Transverse sonographic image of the right lobe of the liver.
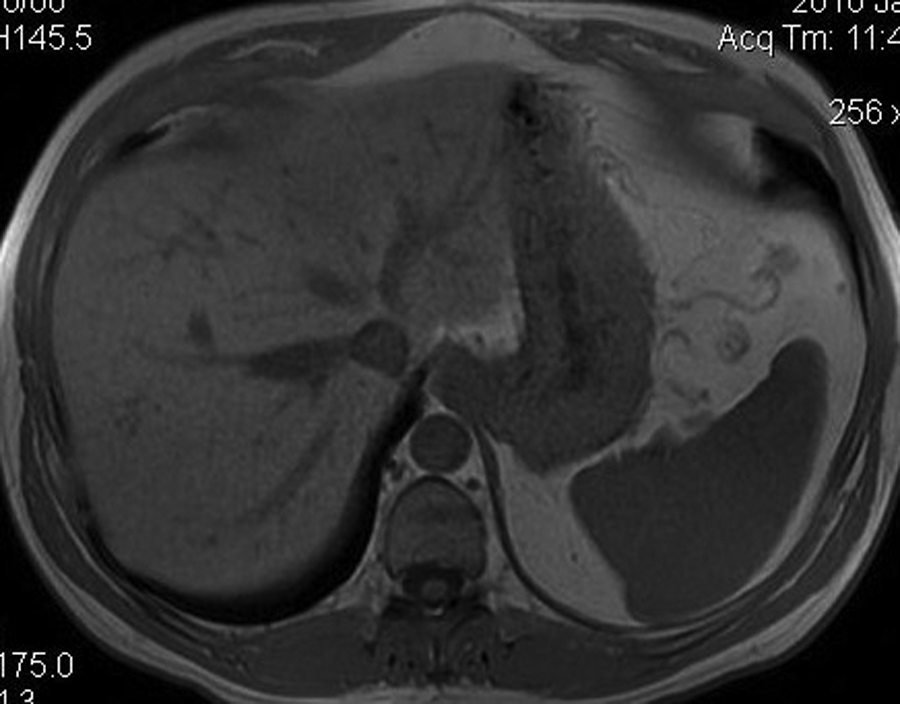
Coronal in-phase magnetic resonance imaging through the liver.
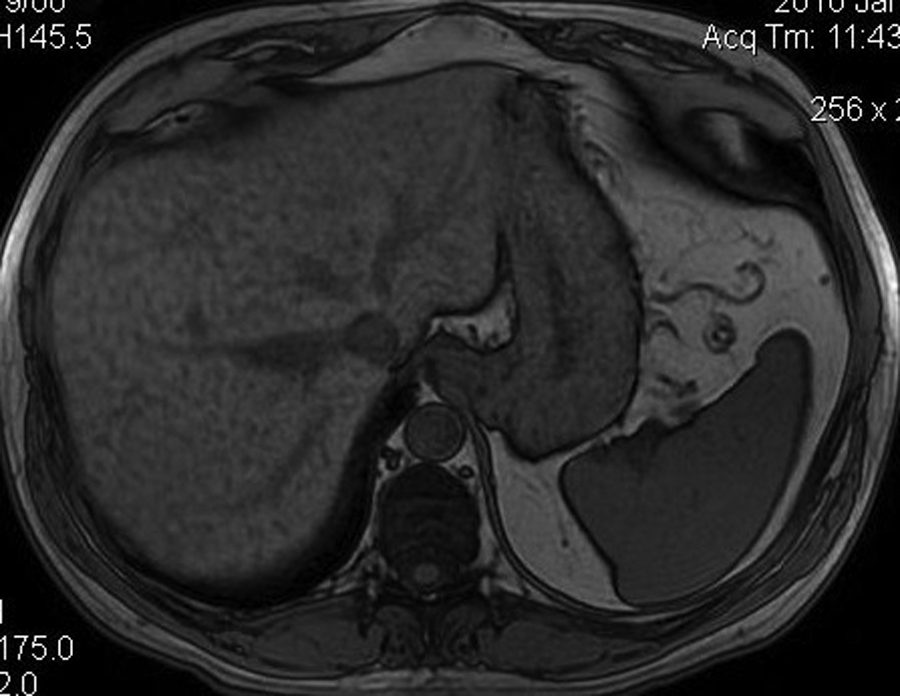
Coronal out-of-phase magnetic resonance imaging through the liver.
Discussion
Fatty liver is a condition in which excessive fat accumulates in the liver. This condition is usually found incidentally and is initially suspected with increased liver enzymes. Fatty liver commonly presents with no symptoms or with nonspecific symptoms such as fatigue, malaise, and right upper quadrant discomfort. 5 Fatty liver is a common, benign, and reversible condition that affects 20% to 30% of the adult population in the Western world.1,3 Fatty liver can consequently lead to NASH, a more severe liver condition that can lead to cirrhosis, end-stage liver disease, or even hepatocellular carcinoma.2,5–7 NAFLD can be associated with numerous conditions, some of which include obesity, hyperlipidemia, type 2 diabetes mellitus, rapid weight loss, malnutrition, jaundice, insulin resistance, hepatitis, and hyperuricemia.1–3,5–7
Imaging Techniques
A liver biopsy is the gold standard for determining hepatic fat content and staging fibrosis.1,3–6,8,9 However, the invasiveness of this approach is often a contraindication in certain patients. Noninvasive imaging modalities such as sonography, CT, and MR can also detect hepatic fat content.
Sonography is commonly used for detecting fatty infiltration of the liver. By sonography, increased amounts of hepatic fat will cause an increased echogenicity of the liver. 6 Because of this, the liver appears more echogenic when compared to the ipsilateral kidney cortex. Fatty infiltration of the liver can be diffuse or focal, or it may also present with an overall fatty liver with certain areas of the liver being spared. Because of these differences, multiple studies have shown that the sensitivity and specificity of detecting hepatic fat by sonography range from 60% to 94% and 84% to 95%, respectively, with the sensitivity increasing as the severity of fat content increases. 4 For example, a sonogram has a sensitivity of 55% when hepatic fat content is 10% to 19%, compared to a sensitivity of 80% when the presence of fat is >30%. 1 However, patient obesity and the detection of smaller amounts of hepatic fat reduce sonography’s sensitivity. 1 Unfortunately, sonography is also not able to grade the amount of fat content, and its subjectivity is highly operator dependent. 1
A non-contrast-enhanced CT scan is the most accurate noninvasive CT technique for characterizing fatty infiltration of the liver.1,4 Determination of fatty liver is made by measuring the attenuation differences in Hounsfield units between the liver and the spleen. A fatty liver has a lower attenuation value than the spleen and will appear darker.4,6 The disadvantages of a CT for determining fatty infiltration of the liver are the use of ionizing radiation and its inability to qualitatively diagnose fatty infiltration of less than 30%. 4
MR uses the phenomenon of chemical shifts to produce images that occur because different nuclei in unrelated chemical environments experience slightly different magnetic field strengths. 1 These differences in resonance frequency of water and fat are used by MR imaging to differentiate tissues containing water from those containing both water and fat. 1 When applying this principle for MR imaging of a fatty liver, there is a notable loss of signal intensity on the out-of-phase images (because opposing signals from water and fat tend to cancel each other out) and a less appreciable increase in signal intensity on the in-phase images. 6 MR images of a normal, nonfatty liver show no change in the signal intensity of the liver parenchyma of an out-of-phase to an in-phase image. It is now clinically useful to use this method of comparing in-phase to out-of-phase images, known as the Dixon method, for detecting and quantifying fatty infiltration of the liver. The disadvantages of an MR for determining fatty infiltration of the liver is that image quality is affected by respiration and motion, and it is time-consuming and also expensive. 1
Sonography, CT, and MR can all identify fat within the liver if the fat content is greater than 33%. However, none of these noninvasive modalities is completely sensitive, nor can they distinguish between simple fatty infiltration and NASH.2,5,6
Nonalcoholic fatty liver disease (NAFLD) is a general term used to describe a variety of liver diseases that refers to excess fat within the liver in the absence of alcohol consumption.7,10 NAFLD is the most common cause of chronic liver disease, and its incidence is likely to increase with the predicted increase in obesity and type 2 diabetes. 1
There is discrepancy in the ability to consistently determine fat content in a liver. The noninvasive imaging techniques available for the detection of hepatic fat content include sonography, CT, and MR, but all have shown to have a low sensitivity when hepatic fat infiltration is <30%.2,6 However, the sensitivity of each modality improves with increasing degrees of fatty infiltration.
Liver transplant is the primary surgical treatment for NAFLD, but there are steps to help prevent or reverse this condition. 7 Lifestyle modifications, such as dietary changes and exercise to encourage weight loss, are the best measures to help prevent NAFLD. 1
Conclusion
Fatty liver infiltration is commonly detected by sonography. Sonographic characteristics include an increased echogenicity of the liver. This increased echogenicity causes the liver to be more echogenic when compared to the ipsilateral kidney cortex. Fatty infiltration of the liver can be diffuse or focal, or it can also present with an overall fatty liver with certain areas of the liver being spared. There are no medical treatments for fatty liver, but certain lifestyle changes, such as exercise and diet, can help prevent NAFLD.
Footnotes
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The authors received no financial support for the research and/or authorship of this article.