
Abstract
Patient satisfaction with obstetric sonography may indicate the quality of services rendered in the sonographic suite. A comparative assessment of the quality of services between government and missionary hospitals in southeastern Nigeria is not known. The aim of this study was to compare the satisfaction rating during obstetric sonography between government and missionary hospitals in Nigeria. Seven hundred pregnant mothers who had obstetric sonography at least twice in both missionary and government hospitals were recruited for the study between January and June 2010. Questionnaires completed by patients were designed to obtain information on demographic variables, as well as patient satisfaction ratings of some indices of satisfaction that the sonographer and the managers of health institutions could modulate. The variables were friendliness of sonographers with the patients, patient waiting time, patient comfort within the waiting area and in the scanning suits, patient safety, sonographer-patient communication, and protection of patient privacy. Patients undergoing obstetric sonography were moderately satisfied with the services rendered to them in missionary hospitals but moderately dissatisfied with the services in government hospitals.
Satisfaction can be defined as the extent of an individual’s experience compared with his or her expectations. 1 Patient satisfaction is related to the extent to which general health care needs and condition-specific needs are met. 2 Assessment of the extent to which patients are satisfied with health services is clinically relevant because satisfied patients are more likely to comply with treatment, 3 take an active role in their own care, 4 continue using medical care services, and stay with a health provider (when there are other choices) and maintain a specific system. 5 In addition, health professionals and managers of health institutions may benefit from satisfaction surveys that identify potential areas for service improvement, and health expenditure may be optimized through patient-guided planning and evaluation. 6
The modern approach to health care seeks to engage the attention of patients, health care professionals, and the public in developing health care services and equity of access. 2 In view of the above assertion, assessment of patient satisfaction is important if service improvement is to be translated into outcomes meaningful to patients, especially improved quality of life.7,8 Patient perception and satisfaction of care are an indicator of the quality of care and frequently included in health care planning and evaluations. 9
Over recent years, national health insurance scheme management has set up an inquiry to ascertain how well the services to patients are being delivered at a local level by obtaining the experience and perception of patients and the community. Patient satisfaction is now deemed an important outcome measure for health services.10,11 For service providers to meaningfully ascertain the experience and perception of patients and the community, research must first be conducted to identify the way and terms in which those patients perceive and evaluate that service. 11 Over the years, a reform in the health care sector in Nigeria has placed emphasis on health care delivery based on the quality of services provided. This has compelled all sectors of health institutions to enhance cost-effective services by ensuring that the efficacy and values of the services rendered are as high as possible.
Pregnant women are usually in both physical and emotional stress, worrying about the state of the fetus and the duration of labor. Dealing effectively with such clinical situations involves many abilities. Investigators studying patient satisfaction showed that the mode of medical care delivery appears to be more important to patients than the care itself. 11 Obstetric sonography is often a standard part of prenatal care as it yields a variety of information regarding the health of the fetus as well as the progress of the pregnancy. Many patients undergoing obstetric sonography are usually apparently healthy and in a good state of mind to judge and assess services provided, and this group was chosen to provide a satisfaction rating of services provided to them in imaging departments in two groups of hospitals.
A certain approach to health care delivery could be influenced or modulated by the sonographer and managers of health institutions/facilities. Some of these variables include patient waiting time, sonographer-patient interaction or communication, patient safety, protection of patients’ privacy, and patients’ comfort within the scanning suite. The aim of this study was to compare the satisfaction of patients in missionary hospitals with those in government hospitals within southeastern Nigeria based on the variables that the sonographer could modulate.
Methods
This study was conducted between January and June 2010 among the missionary and government hospitals in southeastern Nigeria.
Seven hundred pregnant women who had obstetric sonographic scans in both missionary and government hospitals were selected for the study; 326 were selected from government hospitals, and 322 were selected from missionary hospitals. Ethical approval for the study was obtained from Ebonyi State University Teaching Hospital, and patient consent was obtained. A validated self-completion questionnaire was designed and copies given to the enlisted patients to provide the needed information and opinions during at least their second visit. The questionnaires were given to the patients immediately after they were given the results of the examination. Results of the examination were given to the patients on the same day of the examination. The questionnaires were designed to obtain both qualitative and quantitative data, as well as factual and attitudinal information. It contained 18 questions divided into three sections. Section A contained questions about patients’ demographic data, such as age, sex, occupation qualification, and so on. Section B contained questions about patients’ ratings and satisfaction with the tested indices of satisfaction. Section C included open-ended questions and contained questions about patients’ views and opinions on what should be done to increase their satisfaction during obstetric sonography. This section allowed patients to rate their overall satisfaction with obstetric sonography in the hospital using a 4-point Likert scale, with 1 = highly dissatisfied, 2 = moderately dissatisfied, 3 = moderately satisfied, and 4 = highly satisfied.
The data were analyzed using the Statistical Package for the Social Sciences (SPSS) Version 14.0 (SPSS, Inc., an IBM Company, Chicago, Illinois). Data were two-tailed, and P < .05 was chosen as the level of significance. Descriptive statistics were used to obtain the mean value of the rating. Pearson’s correlation analysis was used to assess the relationship between the test indices and patients’ overall satisfaction.
Results
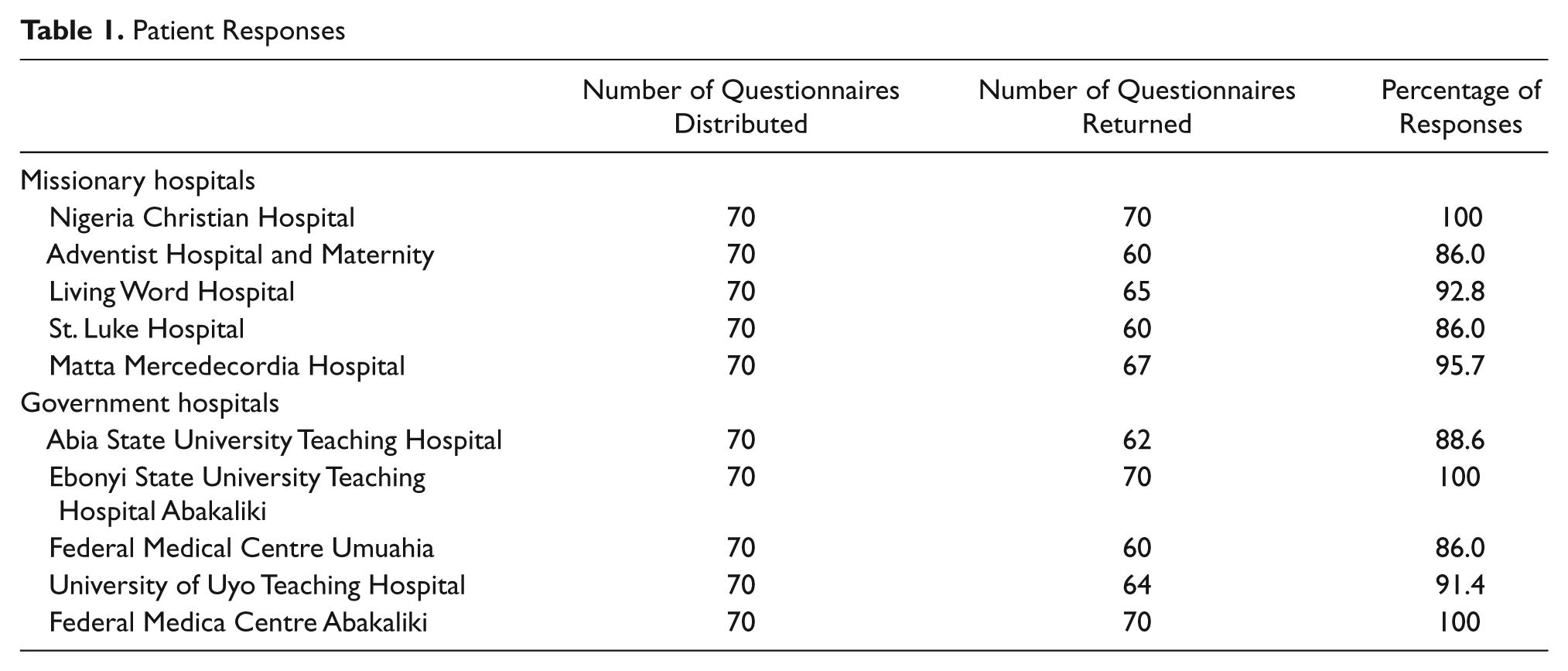
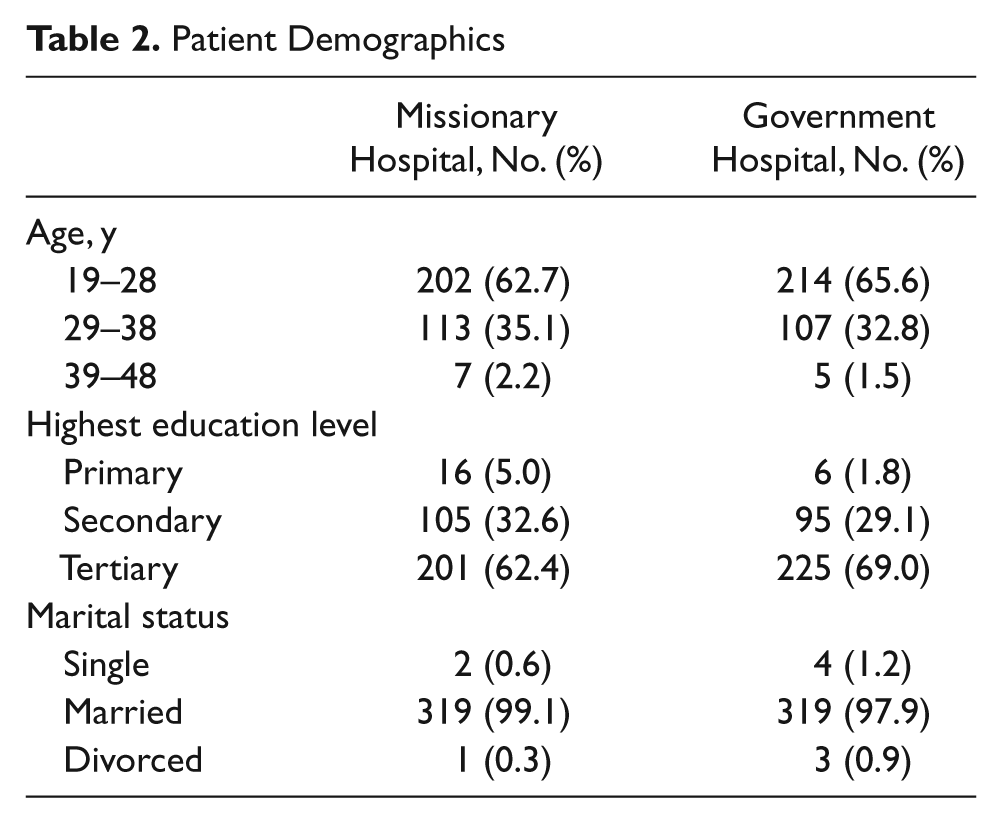
Of 700 questionnaires distributed to the selected pregnant women, 648 were returned and properly answered, for a response rate of 92.6%. Table 1 shows the response rate of mothers from the various hospitals. Table 2 displays the demographics of the patients. Table 3 is a profile of patient satisfaction with the tested indices of satisfaction, whereas Table 4 shows the correlation of the various indices with overall satisfaction.
Patient Responses
Patient Demographics
Patient Satisfaction Ratings of the Variables in the Two Groups of Hospitals
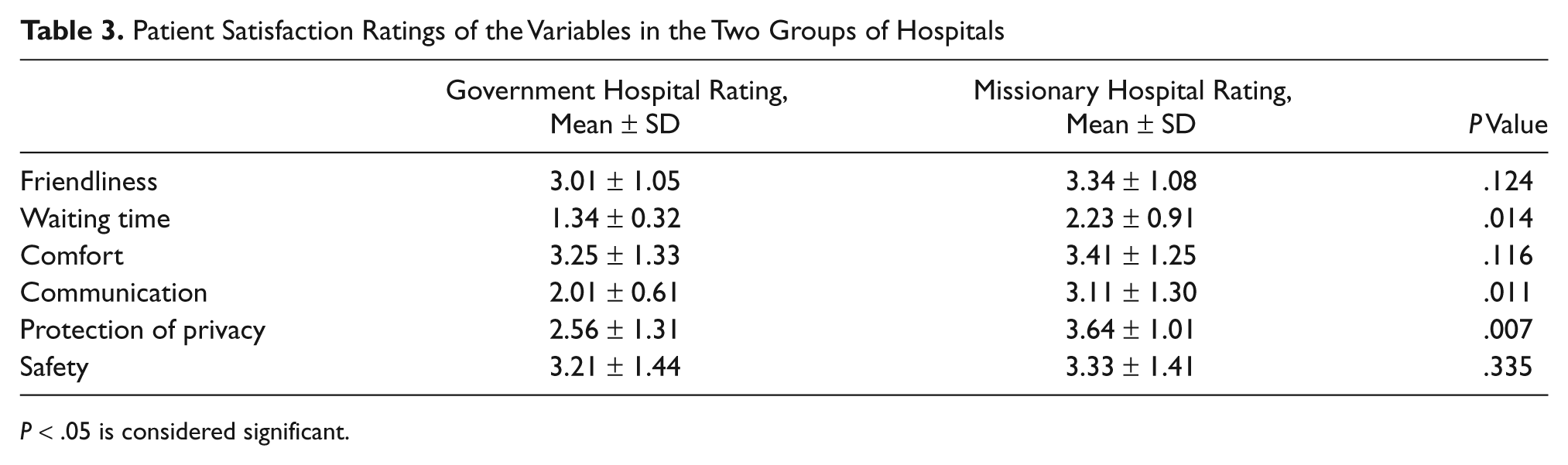
P < .05 is considered significant.
Correlation of the Various Indices of Satisfaction With Overall Satisfaction

P < .05.
Age and educational level had a negative but significant correlation with satisfaction with waiting time (P < .003). Older patients and patients with a tertiary level of education had less patience with waiting time. Section C demonstrates that 98.7% of the patients believed that patient waiting time should be reduced, and 27.4% believed that comfort in the waiting area and within the sonography suite as well as sonographer-patient communication should be improved.
Discussion
This study sought to compare the satisfaction ratings of patients undergoing obstetric sonography in government hospitals with those in missionary hospitals in Nigeria. Table 1 shows a good response rate of the patients from the hospitals. Patient satisfaction ratings of the six factors that sonographers and managers of health institutions could modulate were assessed in this study and shown in Table 3.
Friendliness
Patients were moderately satisfied with the friendly attitude of the sonographers in both government and missionary hospitals (3.01 ± 1.05 and 3.34 ± 1.08, respectively; P = .124). The first contact with the patient should reveal a professional attitude and a smiling facial expression, giving the patient a feeling of welcome. Friendly attitude can also be displayed in the way the sonographer addresses the patient. All patients should be addressed as Mrs. or Dr. according to the information given on the patient’s card. 12 The temptation to use diminutives must be avoided as they detract from the patients’ dignity and individuality. Sonographers must avoid displaying aggressive attitudes because this demonstrates the possibility of serious hostility and actual physical violence. In their study of doctor-patient interaction and patient satisfaction, Korsch et al. 13 noted that patients expect a friendly and kind attitude from their doctors and other medical professionals.
Patients’ Waiting Time
This study shows that obstetric sonography patients were moderately dissatisfied with the waiting time in both groups of hospitals (government hospitals: 1.34 ± 0.32; missionary hospitals: 2.23 ± 0.90; P = .014). According to Pauline Culmer, 13 “The patient charter has led to the introduction of a minimum waiting time standard in many departments.” Pregnant women coming to imaging departments for obstetric sonography are usually anxious of the state of the fetus and the general conditions of the pregnancy.
This anxiety is likely to be exacerbated if waiting time is prolonged. Special attention should be paid to the waiting area during the design of imaging departments. Magazines, journals, and television should be provided in the waiting area to make the waiting period a little easier. More imaging suites and machines should be provided, and more sonographers should be trained and employed for imaging in both hospitals. The examination room could be set up beforehand with all necessary equipment and accessories so that the patient’s actual examination time is minimized. More important, increased education and experience of the sonographer would help reduce examination time. It should also be noted that prolonged waiting time could increase anxiety in patients who worry about the results or findings, how long the examination will last, whether the examination will hurt, how soon things will improve, and when they will go home. Prolonged waiting times also may result in boredom. Boredom may be a problem whenever people have nothing to relieve their forced inactivity. Sonographers should not assume that pregnant women cannot be both bored and anxious at the same time. One state does not necessarily exclude the other; in fact, boredom can exacerbate anxiety. 12
Patient Comfort/Sonographer-Patient Communication
Patients were moderately satisfied with the level of comfort received in both groups of hospitals (government hospitals: 3.25 ± 1.33; missionary hospitals: 3.41 ± 1.25; P = .116). This study also shows that the mothers were moderately dissatisfied with the level of communication they received from sonographers in government hospitals (2.01 ± 0.61) but were moderately satisfied with the communication from sonographers in missionary hospitals (3.11 ± 1.30). This may be because the government hospitals are sometimes quite busy, and attention may not be paid to communication. It is only through communication with the patients throughout the examination that sonographers can assess the patients’ condition, thereby providing the best care for them while in the imaging suite. As Dwane 14 puts it, “The end products of every examination should include a happy, comfortable patient who leaves the department feeling she had been treated well and who remembers the experience as something good and positive.” Sonographers should make time to care for the patients and avoid the temptation to brand some patients “difficult.” Attention to the patients’ condition through constant communication and observation is important both for general patient care and for the health and safety of the patients. A balance, however, must be found between caring for the patient who is being examined in the imaging room and not keeping other patients waiting too long.
Protection of Patients’ Privacy
Patients who had obstetric sonography in government hospitals were moderately dissatisfied with the protection of their privacy (2.56 ± 1.31), whereas those who had obstetric sonography in missionary hospitals were moderately satisfied with the protection of their privacy (3.64 ± 1.01). This may be because most government hospitals, especially the teaching hospitals in Nigeria, have students on clinical postings, and a significant number of these students can be seen in the sonography rooms watching examinations or even participating in some of them. The protection of the patients’ privacy may be poor in these cases. Sonographers should treat their patients with the same kind of concern that they would appreciate if they were the patients themselves.
Patients’ Safety
Patients were moderately satisfied with the level of safety they experienced in both groups of hospitals (government hospitals: 3.21 ± 1.44; missionary hospitals: 3.33 ± 1.41; P = .335). Safety in this context does not mean freedom from danger and absence of risk. There is no known scientifically proven biological danger from medical sonography. Other imaging modalities such as radiography have a certain inherent risk. Apart from the imaging modalities, some other conditions of the imaging suites could present a certain degree of risk to pregnant women, who may not be as agile as nonpregnant subjects. In this case, some questions need to be addressed about the safety of the sonography suites: Is the lighting in good or poor condition? Is the floor covering slippery? Do the stairways have handrails? Are there good signposting and directional aids? What sonographers can do for their patients is minimize the risks that are unavoidable and eliminate those risks that can be removed. Sonographers must ask not only how they can ensure the safety of their patients but also how they can reduce the risks to the patients. This should be the concern of all sonographers.
Correlation analysis shows that there is no significant correlation between age, educational qualifications, or occupation with the satisfaction of the tested variables. Table 4 shows that waiting time, sonographer patient communication, and friendly attitude of sonographers to their patients had a significant strong positive correlation with the overall satisfaction with obstetric sonography. Content analysis of section C in the questionnaire shows that overall patient satisfaction during obstetric sonography was 3.01 ± 0.13 in missionary hospitals and 2.33 ± 0.34 in government hospitals.
Conclusion
Patients were moderately satisfied with services rendered to them during obstetric sonography in missionary hospitals but moderately dissatisfied with obstetric sonographic services in government hospitals. Patient waiting time, sonographer–patient communication, and protection of patients’ privacy need to be improved in government hospitals in Nigeria. Further studies to assess the satisfaction rating of patients during other sonographic examinations in private missionary and government hospitals would be interesting.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.