
Abstract
Background
In the United States, obesity is a prevalent chronic disease diagnosed in over 40% of adults. 1 Obesity is associated with an increased risk of hypertension, type 2 diabetes, cardiovascular disease, sleep apnea, liver disease, arthritis, and mortality.2,3 Sustained weight loss of at least 5% is recommended for clinically meaningful reductions in the risk of diabetes, with larger amounts of weight loss (10% or more) resulting in greater benefits. 4
In addition to exercise and dietary modification, glucagon-like peptide-1 receptor agonists (GLP-1 RA) and dual glucose-dependent insulinotropic polypeptide (GIP) receptor GLP-1 RA are FDA-approved and recommended in weight-management guidelines for the long-term treatment of obesity. 5 However, there are several challenges to initiating these newer therapies. Barriers include insurance coverage, cost, medication supply, and medication intolerance (leading to either full discontinuation of the medication, changing to a different medication in the class, or modifying the traditional stepwise dose increase schedule).
There is a large body of literature supporting clinical pharmacists working in primary care and positively impacting the management of chronic diseases, including type 2 diabetes, hypertension, and dyslipidemia. 6 At the Veterans Affairs Tennessee Valley Healthcare System, a multidisciplinary weight loss clinic with a pharmacist-run pharmacotherapy service demonstrated a statistically significant reduction in weight among participants. 7 There is also evidence to support weight loss in ambulatory clinics with multidisciplinary support of embedded pharmacists. 8
Data regarding the impact of clinical pharmacists in weight loss medication management services since the FDA approval of GLP-1 RAs and GIP/GLP-1 RAs for weight loss are limited. The Internal Medicine resident clinic at the University of Vermont Medical Center includes 35 residents. The clinic embedded a clinical pharmacist in July 2023. The pharmacist has various roles, including improving access for patients with obesity, by providing direct patient care visits for chronic disease state management under a collaborative practice agreement, with the ability to prescribe new medications, adjust medication doses, and order and interpret lab results. Additional roles of the clinical pharmacist include offering e-consultation within the electronic medical record to answer drug information questions, providing population-based medication management, and providing clinician and patient education. This includes medical resident education with direct teaching in resident didactic conferences, and co-location 1 day per week in the resident workroom to assist with patient care. The purpose of this study was to assess the impact of the clinical pharmacist’s management on the amount and rate of weight loss in patients with obesity. Specifically, the study aimed to compare the percentage of weight loss achieved in patients managed by a clinical pharmacist versus those managed by other clinicians who did or did not prescribe weight loss pharmacotherapy.
Methods
This was a matched case-control study of primary care patients at the University of Vermont Medical Center’s Internal Medicine resident clinic. Cases were defined as adult patients 18 years or older, without a diagnosis of diabetes who had at least 1 appointment with the Internal Medicine clinic’s clinical pharmacist between July 2023 and May 2024 regarding weight loss. The 2 control groups included patients matched to cases by insurance and body mass index (BMI) who were either prescribed weight loss medications by a different primary care clinician or not prescribed any weight loss medications. Baseline demographic data included age, sex, race, type of insurance, and type of primary care clinician (resident physician, physician assistant, nurse practitioner, or attending physician).
Data including weight, BMI, lipid profiles, blood pressure, A1C, smoking status, atherosclerotic cardiovascular disease (ASCVD) risk score, depression screening scores (PHQ-9), anxiety screening scores (GAD7), and use of antihypertensive agent(s), aspirin, and statins were collected at baseline and at 6-month follow-up. If there was no follow-up data 6 months from the baseline date, then data as close to 6 months, but not sooner, was used. Use of medications that predisposed patients to weight gain including anticonvulsants/neuropathic medications, antidepressants, antipsychotics, corticosteroids, hormonal therapy, insulin, thiazolidines, or sulfonylureas was also documented.
For patients prescribed weight loss medications, the name of medication, initiation date, and maximum dosage achieved were collected. Information about insurance prior authorizations (PAs) was also noted. Adverse reactions were reviewed including gastrointestinal intolerance (nausea, vomiting, heartburn, constipation, and diarrhea), headache, fatigue, injection site reactions, and rarer adverse effects such as acute pancreatitis, acute gallbladder disease, acute kidney injury, and suicidal ideation. As part of data collection, it was noted if patients experienced medication interruptions or discontinuation and the reason (such as cost, drug shortage, temporary adverse effects, or other reasons). Data on total number of telehealth visits with the pharmacist and total number of nonvisit encounters including calls and patient portal messages during the data collection window was recorded. Additional interventions, including referral to a dietician, referral to case management and referral to another resource were tracked. This study was approved as exempt research by the University of Vermont and University of Vermont Medical Center’s Institutional Review Board (STUDY00003126).
The primary outcome was the change in percentage weight loss among groups. Secondary objectives included evaluating the rate of weight loss across groups, changes to blood pressure and other serologic markers between groups, and frequency of referral to other specialists (dieticians). Data were analyzed using descriptive and univariate statistics. Dichotomous variables were analyzed using Chi-square and Fisher’s exact tests. Continuous variables were analyzed using the Mann-Whitney-Wilcoxon test. Data were analyzed using Stata version 18 (Stata Corp, College Station, Texas), with P < 0.05 required for statistical significance.
Results
A total of 94 patients met eligibility (Table 1). Mean age was 50.1 years (SD = 13.3), with a mean weight of 108.4 kg (SD = 30.3) and mean BMI of 39 kg/m2 (SD = 8.8) at baseline. A total of 35 patients were seen by a clinical pharmacist at least once, 24 control patients were prescribed weight loss medication, and 35 control patients were not prescribed weight loss medication. Most patients were white females with commercial insurance. There were no significant differences between groups in any baseline characteristics, except for 10-year ASCVD risk (3.5% in controls with weight loss medications vs 7.2% in controls without weight loss medications, P = 0.03).
Baseline Demographics (N = 94).
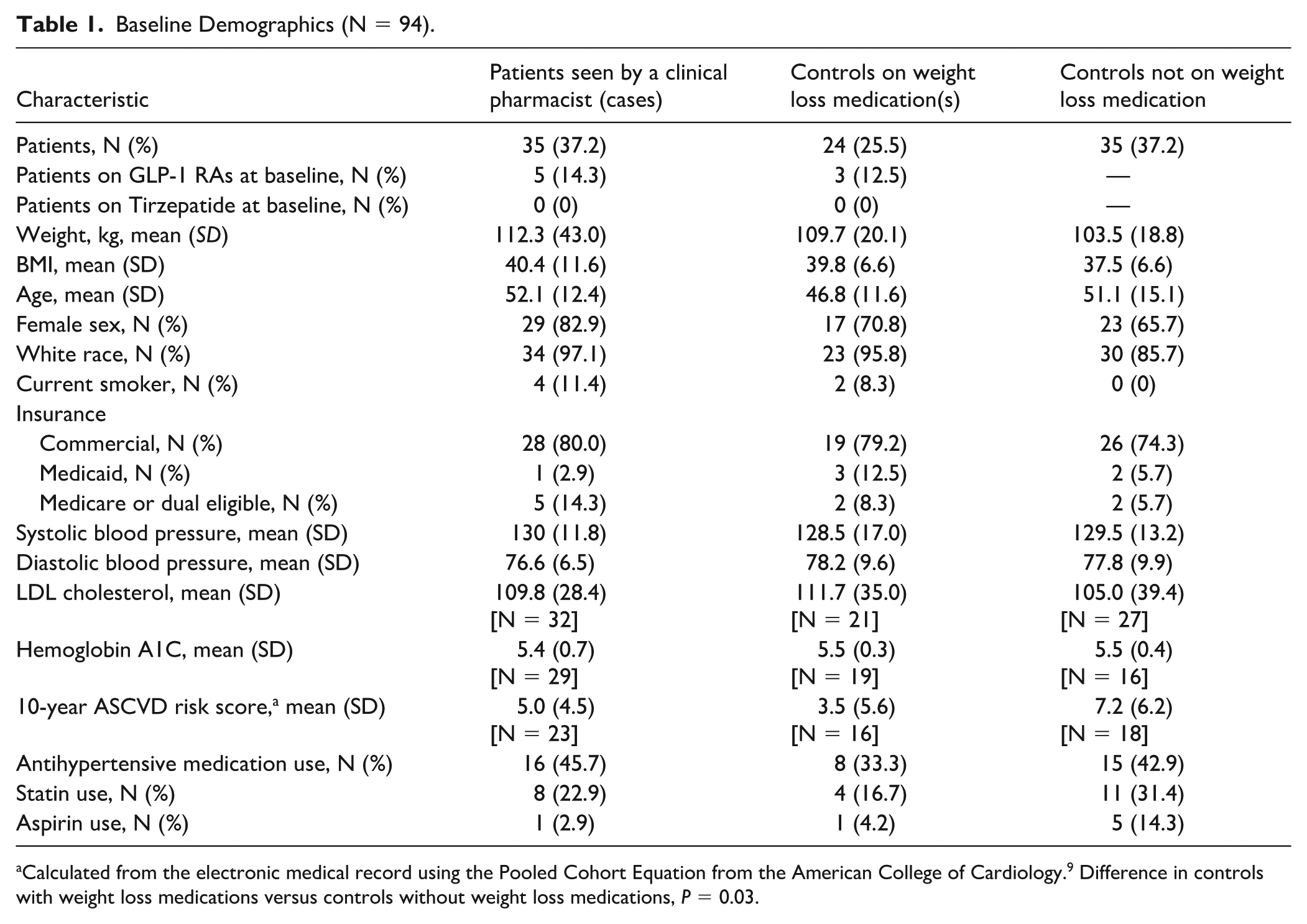
Calculated from the electronic medical record using the Pooled Cohort Equation from the American College of Cardiology. 9 Difference in controls with weight loss medications versus controls without weight loss medications, P = 0.03.
In our study time frame, patients were seen by the clinical pharmacist an average of 4 times (SD = 2) and had an average of 7.4 (SD = 4.4) additional nonvisit encounters (such as telephone calls or electronic messages through the electronic medical record). Forty-three percentage of patients were referred to our clinic’s dietician by the clinical pharmacist versus 25% of control patients prescribed a weight loss medication (P = 0.18) and 11% of control patients not on weight loss medication (P = 0.006). Referrals to case management or other resources were similar between groups.
Fourteen patients (40%) were started on semaglutide and 11 patients (31.4%) were started on tirzepatide in the pharmacist-managed group, as the first medication prescribed. Insurance coverage and drug shortages sometimes necessitated changes in therapy. At the end of the study, 10 patients (28.6%) in the pharmacist group were on maintenance semaglutide doses (1.7 or 2.4 mg) and 13 (37.1%) were on maintenance tirzepatide doses (5, 10, or 15 mg), compared with 3 patients (12.5%) on each medication in the clinician group. No patients in the control group who were not on baseline weight loss medications initiated either therapy during the study period.
At 6-month follow-up, mean weight loss from baseline was −11.8%, −8.3%, and +1.3% among pharmacist-managed cases, controls with weight loss medications, and controls without weight loss medications, respectively (Figures 1 and 2). Weight loss was significantly higher in patients on weight loss medications than controls not on weight loss medications (cases vs controls without weight loss medications, P < 0.001; controls with weight loss medications vs controls without weight loss medications, P = 0.002) but was not significantly different between cases and controls with weight loss medications (P = 0.12). The rate of weight change per week was −0.29, −0.17, and −.02 kg among cases, controls with weight loss medications, and controls without weight loss medications, respectively. The rate of weight change was significantly higher for cases versus controls with weight loss medications (P = 0.04) and for cases versus controls without weight loss medications (P < 0.001). Controls with weight loss medications had a significantly higher rate of weight change than controls without weight loss medications (P = 0.008). The average number of weeks to follow-up was 39.6 weeks (SD = 10.3) among cases, 59.7 weeks (SD = 40.3) among controls with weight loss medications, and 48.6 weeks (SD = 62.1) among controls without weight loss medications.

Difference in percentage weight loss at follow-up.
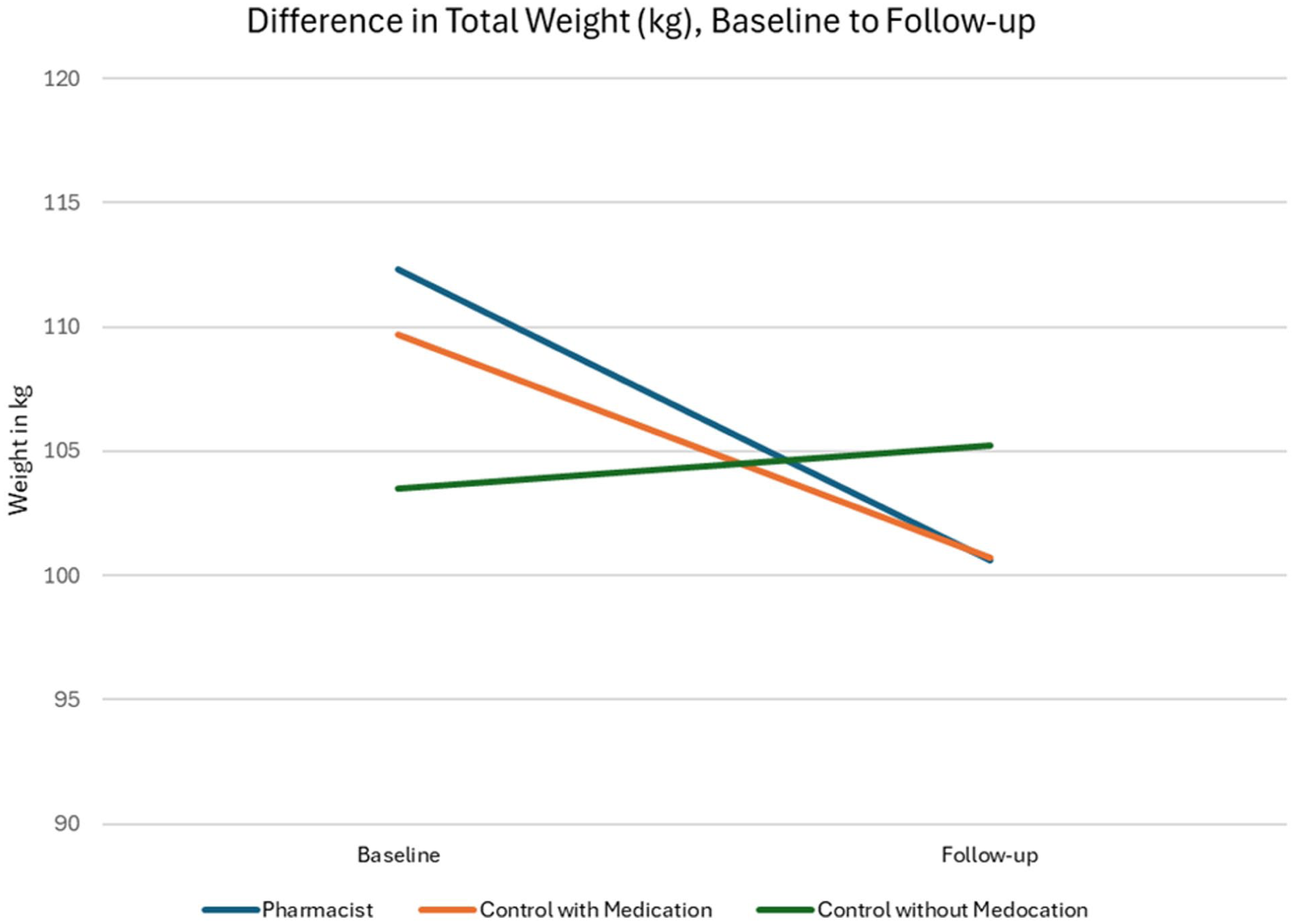
Difference in total weight (kg), baseline to follow-up.
Among all groups, there were no significant differences in numbers of patients on antihypertensive therapy, (P = 0.62), statin therapy (P = 0.47), anticonvulsants/neuropathic pain medications (P = 0.062), antidepressants (P = 0.34), antipsychotics (P = 0.88), or hormonal therapy (P = 1.0) at the completion of the study. Missing data at follow-up prevented analyses on additional variables (lipid profiles, A1C, systolic and diastolic blood pressure, ASCVD risk, and PHQ/GAD scores).
Discussion
In our study, patients prescribed weight loss medications lost significantly more weight than patients who were not on weight loss medications, emphasizing the important role medications have in the treatment of patients with obesity. Patients managed by a clinical pharmacist trended toward greater weight loss, although these patients did not lose significantly more weight than patients managed by other clinicians.
The rate of weight loss was significantly higher in patients managed by a clinical pharmacist. This is potentially due to the closer follow-up, faster titration of medications to maintenance doses, patient coaching and education, and the structure of the pharmacist’s management. The pharmacist’s general approach for weight loss medications included prescribing initial doses (semaglutide 0.25 mg, tirzepatide 2.5 mg) and titrating no more frequently than 4 weeks per FDA-approved dosing. Semaglutide was titrated every 4 weeks as tolerated to a maintenance dose of 1.7 or 2.4 mg, and tirzepatide was titrated as tolerated to a maintenance dose of 5, 10, or 15 mg, based on patient response and tolerability. Dose adjustments or interruptions were handled on a case-by-case basis, especially during this timeframe where drug shortages were prevalent. The clinical pharmacist visits were focused on weight management (vs primary care clinician visits which often cover multiple patient concerns) and this appointment structure provided the clinical pharmacist time to review weight loss specific therapies and considerations like referral to a dietician. The clinical pharmacist additionally had dedicated follow-up visits for weight management as well as other communication through electronic messages and/or telephone calls. Recurring topics addressed in electronic messages and telephone calls included finding a pharmacy if the patient’s weight loss medication was unavailable due to supply issues, navigating doses adjustments when desired dose was unavailable, and recommendations to manage adverse reactions.
Most patients in this study had commercial insurance and required PAs to cover GLP-1 RAs and GIP/GLP-1 RAs. From our review of patients’ records, most PAs were approved for these patients; however, during the study timeframe, medication shortages were common. For patients with Medicare and Medicaid, the PAs for newer weight loss medications were often denied; during this study period, our state’s Medicaid program did not cover any weight loss medications, and this study was conducted prior to the FDA approval of semaglutide and tirzepatide for additional indications in patients with overweight or obesity like cardiovascular risk reduction and obstructive sleep apnea. We were therefore unable to fully assess the impact of a clinical pharmacist on weight management for patients with Medicare and Medicaid insurance.
GLP-1 RAs and GIP/GLP-1 RAs, primarily semaglutide and tirzepatide, respectively, have demonstrated substantial weight reduction for patients in clinical trials. Mean weight loss in pivotal clinical trials for semaglutide and tirzepatide at maximum doses were 14.9% and 20.9%, respectively.10,11 In addition, these trials were longer than a year in duration, providing good efficacy data for long-term treatment of obesity.
The decision to initiate medication for obesity must balance risks, benefits, and practical issues (insurance coverage, medication supply) for individual patients. Pharmacists play an important role in assisting patients with medication selection, navigating insurance coverage, managing titration schedules and adverse effects, and providing education to clinicians and patients. Schermerhorn et al 12 analyzed weight loss data from 79 patients at 3 ambulatory clinics in an urban center. Their study found weight loss benefits of approximately 8% from baseline. Crocetta et al 13 analyzed weight loss data of 85 patients in 2 family practices and found a mean weight loss of 9.3%, compared with a clinician-managed cohort (5.1%). Our study included more patients and found slighter higher weight loss in the pharmacist-managed group than previous studies (11.8%), however all recent data demonstrate clinically important effectiveness and should strengthen the limited evidence base for pharmacist management of obesity in ambulatory care.
There are limitations to our study. Our sample size was small, primarily white, and with commercial insurance. Our study duration was also short at 6 months; we would expect to see continued weight loss with longer durations of medication use and may have captured additional significant differences between patients managed by pharmacists and other clinicians with a longer study that included more patients. The setting included an Internal Medicine residency clinic, which is likely different in several ways from other nonteaching clinic practice sites, which may limit the generalizability of this study. Not all resident clinics have the resources of an embedded pharmacist; however, this collaborative model is important for the education and growth of the residents in collaborative interprofessional care, and this could strengthen the ability of other resident clinics to follow this model. We also observed that scheduled follow-up (and follow-up weight documentation) varied between groups. Pharmacist follow-up visits were consistently scheduled approximately 6 months from the initial visit. Patients managed by other clinicians often had follow-up weights collected much further out than 6 months from their baseline weight. Although we sought to match participants on age, sex, and clinician in addition to insurance and BMI, the available sample size was insufficient to permit matching on these additional variables. Therefore, confounding by these factors cannot be ruled out and may have influenced some of the observed associations. Additionally, missing follow-up data for lipid profiles, A1C, systolic and diastolic blood pressure, ASCVD risk, and PHQ/GAD scores limited our ability to examine these secondary outcomes. These limitations should be considered when interpreting the findings, as they may have affected the validity and generalizability of the results.
Conclusion
This study found clinically important weight loss for primary care patients prescribed obesity medications, regardless of whether patients were managed by pharmacists or other clinicians. Patients managed by a clinical pharmacist lost weight at a significantly faster rate than patients managed by another clinicians. These data add support for including clinical pharmacists in patient care teams related to weight loss.
Footnotes
Acknowledgements
None.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the University of Vermont (STUDY00003126) on May 24, 2024, with the need for written informed consent waived.
Author Contributions
Study design and conception: KS, HS, AK, MW. Data collection: KS, JH. Analysis and interpretation of results: KS, HS, AK, MW, JH. Drafting of manuscript: KS, AK. All authors reviewed the results, made important edits to the manuscript, and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.