
Abstract
Background
The rising demand for respiratory care practitioners creates a need for qualified faculty members to teach and mentor the next generation of respiratory therapists (RTs). Key personnel (Program Directors (PDs) and Directors of Clinical Education (DCEs)) turnover can adversely affect student outcomes and the sustainability of RT programming. Recruiting qualified faculty has proven challenging for some, if not most, RT programs. This study aimed to identify the characteristics of current key personnel (PD and DCE) in Commission on Accreditation for Respiratory Care (CoARC)-accredited Entry into Practice and Degree Advancement programs and the self-reported benefits of undertaking a role in RT education.
Methods
The study employed a cross-sectional survey research design using a 20-item electronic instrument. There were 11 demographic questions and nine questions that specifically inquired about the benefits and rewards of becoming and continuing to serve as key personnel. Two questions were open-ended. Associations between the key personnel role and sociodemographic variables were examined using the chi-square tests of independence and an alpha significance level of .05.
Results
There were 294 usable survey responses (35.4% response rate). Key findings include that over half (51%) of respondents have less than 5 years of experience in their administrative role, 24% are currently pursuing an advanced degree, and over 80% receive education-focused professional development. PDs were more likely to report having earned a doctoral degree, more experience within the profession, a higher likelihood of having been promoted, and a higher salary. In contrast, the DCE role was more closely associated with currently pursuing an advanced degree and having completed the Key Personnel Academy through the CoARC. The highest reported benefit of becoming key personnel was the ability to impact the profession through educating future RTs.
Conclusions
PDs and DCEs have important distinctions. PDs often hold advanced credentials and receive higher compensation, whereas DCEs are earlier in their careers and are frequently pursuing degrees. Both share a strong motivation to educate future RTs. Sustaining respiratory care education will require institutional support for career development, along with attention to work–life balance to improve RT educator recruitment and retention.
Keywords
Introduction
Respiratory therapists (RTs) are essential members of the interprofessional healthcare team. The respiratory care profession continues to grow in both number and scope. According to the Bureau of Labor Statistics, the job outlook over the next decade is projected to increase by 13%, adding approximately 17,500 new jobs by 2033. 1 This rising demand for respiratory care practitioners creates a parallel need for qualified faculty members to teach and mentor the next generation of RTs. The Commission on Accreditation for Respiratory Care (CoARC) is the agency responsible for accrediting RT programs, including Entry into Professional Practice and Degree Advancement (DA). Degree levels encompass associate, baccalaureate, and master’s for Entry into Practice, as well as baccalaureate and master’s for DA programs.
RT program faculty are responsible for designing and implementing the curriculum, student instruction across all areas (didactic, laboratory, simulation, clinical), and evaluating program outcomes and effectiveness. 2 In addition to instructional faculty, programs must identify and appoint key personnel. The two primary key personnel roles are the Program Director (PD) and the Director of Clinical Education (DCE). The requirements for these roles are similar and include (1) holding a valid Registered Respiratory Therapist (RRT) credential and a current state license; (2) having a minimum of 4 years of experience as an RRT, including at least 2 years in clinical respiratory care; (3) having at least 2 years of teaching experience as an appointed faculty member in a CoARC-accredited respiratory care program or as a clinical instructor/preceptor for students of such programs; and (4) completing the CoARC Key Personnel (Academy) Training Program if applicable. 2 For DA programs that lack a clinical component, a DCE is not required. Though the PD has broader programmatic responsibilities, the DCE effectively leads the clinical education component of the program.
As part of its annual report, the CoARC shares changes in key personnel. The 2024 Report on Accreditation in Respiratory Care Education highlighted over 220 changes in the calendar year for PDs and DCEs. 3 To add perspective, there were 520 programs and program options under accreditation review by the CoARC in 2024. These changes are classified as permanent, transitional, temporary, or acting, with reasons reported by sponsoring institutions, including resignation, accepting a key personnel role in a different RT program, reassignment, and retirement. This marks an 8% increase from 2023 for both positions. 3 Such a level of key personnel turnover can adversely affect student outcomes and the sustainability of RT programs. Just as retirement and departures from bedside practice can lead to shortages, similar dynamics can arise in the academic setting.
It is the responsibility of the sponsoring institution to recruit and retain a sufficient number of qualified faculty to fulfill the key personnel roles.2,4 With the number of CoARC-accredited RT programs exceeding 500, the need for key personnel naturally increases. Currently, there are over 900 PD and DCE positions for the Entry into Practice and DA programs, some of which remain unfilled. 3 Recruiting qualified faculty, whether instructional or administrative, has proven challenging for some, if not most, RT programs. In the most recent AARC Human Resources Survey for Education Programs, just over half (54%) of all PDs who participated reported difficulties recruiting faculty. 5 The top limitations cited were salary, small applicant pools, lack of adequate academic preparation, and a lack of teaching experience. 5 To recruit means to attract individuals to the role who have a proven record of academic success or the potential to achieve it. Faculty retention involves supporting the educator’s growth and fostering a nurturing academic community. 6 When executed intentionally and with best practices in mind, faculty recruitment and retention efforts can enhance employee satisfaction and lead to impactful student learning experiences. 6 Both factors contribute to high-quality RT education. Given the challenges in recruiting and retaining qualified faculty, understanding the characteristics and perceived benefits of those currently serving in key personnel roles is important. Thus, the purpose of this study was to identify the characteristics of current key personnel in CoARC-accredited Entry into Practice and DA programs and to identify self-reported benefits of serving in these roles. Subsequently, associations between the key personnel role and sociodemographic variables were examined.
Quick look
Current knowledge
The profession of respiratory care and, subsequently, respiratory therapy programming continues to grow, which has resulted in the challenge of recruiting and retaining qualified respiratory therapy educators. There are hundreds of changes in key personnel (PD and DCE) annually, leading to unfilled educator positions. This degree of turnover in key personnel can negatively impact student outcomes and the sustainability of respiratory therapy programs.
What this paper contributes to our knowledge
The sociodemographic profile of PDs and DCEs varies significantly in a few key areas, including education level, practitioner experience, promotion status, and salary. The majority of respondents had less than 5 years of experience as key personnel; however, most received education-focused professional development through their sponsoring institution and the CoARC. The greatest reported benefit of becoming an educator is the impact one can have on the profession of respiratory care through mentoring current and future RTs.
Methods
The methodology for the study is cross-sectional survey research. 7 The investigators designed a 20-item survey (Supplemental Material) after reviewing the literature about the perceived advantages of transitioning from clinician to educator and applicable CoARC-accreditation standards and policies/procedures. Eleven items are demographic, intended to describe the population of key personnel in CoARC-accredited programs. Nine items specifically inquire about the perceived benefits and rewards of becoming key personnel, with two being open-ended to allow categories to surface that may not have been addressed in the creation of the instrument. Qualitative data (including other and open-ended responses) were placed in a quantitative platform (Google Sheets) to be categorized by frequency of occurrence. 7 The primary investigator (KLM) developed the initial version of the survey, after which feedback was solicited from the co-investigators (NP and JBS). Following consensus on the survey content among the investigators, the survey was sent to two additional individuals involved in RT education (organizational administration and key personnel) for further feedback on content, wording, and the estimated time required for completion. This pilot testing process helped establish the face validity of the survey instrument. The feedback from pilot testing led to additional revisions to the survey, and once consensus was reached, the items were uploaded to an electronic survey platform (Qualtrics) for distribution. Goodfellow notes that online surveys offer strategic advantages, such as cost-effectiveness and ease of data collection. 8 The study (IRB25-032) was approved (deemed exempt) by the primary investigator’s Office of Research Compliance.
The finalized instrument was placed into an online survey platform for distribution to all current key personnel from CoARC-accredited Entry into Professional Practice and DA programs. The primary contact for each program is publicly available on the CoARC website under “Find an Accredited Program.” PD contact information is public information and is not treated as confidential. 9 A request for DCE contact information (i.e., institution email address) was requested and provided by the CoARC for research purposes. The invitation to participate in the study was initially sent on March 6, 2025, with reminders sent on March 27, 2025, and April 17, 2025. The survey closed on May 9, 2025. Intellectus360 (Intellectus Statistics 2023, https://www.intellectusstatistics.com) statistical software was used to analyze the data. 10 Descriptive statistics are reported as frequencies and percentages for all categorical data. Chi-square tests of independence were used to examine associations between key personnel roles and each categorical variable. To satisfy the assumption for minimum expected cell counts, some response categories were consolidated before analysis. The electronic survey was sent out to 430 PDs of Entry into Practice and DA programs and 410 DCEs from Entry into Practice programs. The decision was made to exclude Sleep Disorder Specialists and Advanced Practice Respiratory Therapy programs due to their low numbers to protect participant anonymity. Similarly, Medical Directors, while technically key personnel, were not included in the study population because of the significant differences in their roles and responsibilities. PDs and DCEs represent a nonprobability sample, and the sampling technique employed was single-stage. The recruitment email sent to potential participants (N = 840) contained a link to the survey along with the IRB-approved informed consent document. An a priori power analysis was performed using Intellectus360 statistical software to establish the appropriate target sample size. With an alpha level of .05 and a desired power of .80, based on an unspecified effect size, the analysis indicated that a minimum sample size of n = 264 is required.
Results
Demographic characteristics of participants (n = 294).
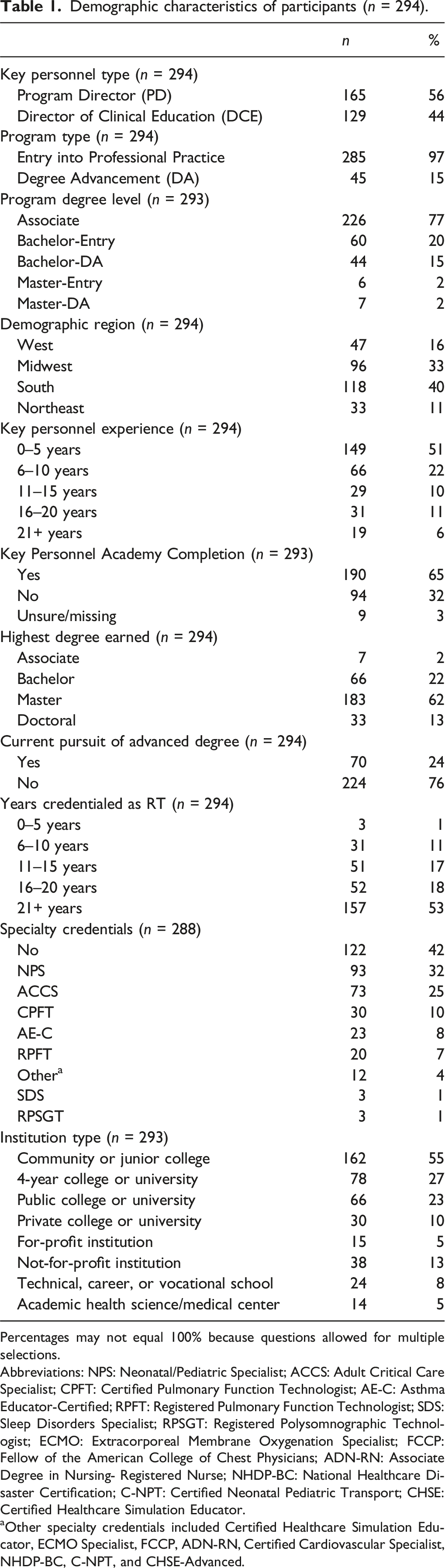
Percentages may not equal 100% because questions allowed for multiple selections.
Abbreviations: NPS: Neonatal/Pediatric Specialist; ACCS: Adult Critical Care Specialist; CPFT: Certified Pulmonary Function Technologist; AE-C: Asthma Educator-Certified; RPFT: Registered Pulmonary Function Technologist; SDS: Sleep Disorders Specialist; RPSGT: Registered Polysomnographic Technologist; ECMO: Extracorporeal Membrane Oxygenation Specialist; FCCP: Fellow of the American College of Chest Physicians; ADN-RN: Associate Degree in Nursing- Registered Nurse; NHDP-BC: National Healthcare Disaster Certification; C-NPT: Certified Neonatal Pediatric Transport; CHSE: Certified Healthcare Simulation Educator.
aOther specialty credentials included Certified Healthcare Simulation Educator, ECMO Specialist, FCCP, ADN-RN, Certified Cardiovascular Specialist, NHDP-BC, C-NPT, and CHSE-Advanced.
Perceived benefits of becoming key personnel (N = 280).

Descriptive statistics on additional potential benefits.

Note. Percentages may not equal 100% because questions allowed for multiple selections. *Other types of support and leadership development are described in the summary section.
Frequency by key personnel type.

Note. Due to rounding error, percentages may not sum to 100%.
Summary of open-ended responses
Additional types of professional support noted by respondents were categorized into three areas: monetary support/funds, tuition/degree advancement support, and pandemic impact on professional development support. The annual monetary funds ranged from $700 to $2000. Sponsoring institutions either paid/reimbursed key personnel for pursuing an advanced degree or the faculty members received additional salary for earning the degree. Three respondents noted that the COVID-19 pandemic had negatively impacted the availability of professional development funds for faculty. Key personnel also reported holding other leadership positions outside of their program administrative role. Categories, which arose from open-ended questions on the survey instrument, are presented based on the quantity of the responses received for each in order of most to least frequently reported: state society leadership (board and/or committee member), institutional committee member/chair, transitioned from DCE to PD, college leadership (department chair, associate dean, dean, etc.), organizational board member (CoARC, AARC, NBRC, etc.), organizational committee member/chair (AARC, CHEST, House of Delegates), department manager/director or clinical supervisor/specialist, accreditation site visitor, state licensing board, simulation lab coordinator, and international committee efforts.
Discussion
When evaluating the characteristics of key personnel, we found that PDs appeared more senior both in key personnel tenure and as respiratory care practitioners as 10 years or less in role was less common among PDs than DCEs (65.5% vs 83.0%; P = < .001), while 16 years or more of RT experience was more common (82.8% vs 57.4%; P < .001). Educational attainment differed by role, as the highest degree held by PDs was a masters or doctoral degree more often (86.7% vs 60.5%; P < .001), whereas DCEs highest degree earned was an associates or bachelor’s degree (39.5% vs 13.3%, P < .001) and were more likely to be actively pursuing an advanced degree (31.8% vs 17.6%; P = .005). Consistent with being newer to the role, KPA completion was higher among DCEs (72.9% vs 58.2%; P = .031). Markers of advancement and compensation favored PDs, including higher placement in upper salary bands (overall P < .001) and higher promotion prevalence (48.4% vs 18.6%; P < .001). This finding could reflect the typical and progressive nature of becoming a PD after serving as a DCE. A notable finding was the number of key personnel who did not possess a specialty credential (42%). This could be related to the fact that nearly 3/4 of the population under investigation were relatively new to their higher education administrative roles, and close to 1/4 were currently pursuing an advanced degree. Though there is no specific evidence to suggest that RT faculty members who possess specialty credentials positively impact the teaching and learning of distinct curricular content, the credentials do represent expertise and continued competence beyond traditional RT certifications. 18
Our findings suggest that the main perceived benefit of serving as key personnel is the ability to impact the profession by educating future RTs (265/280; 95%). A second, closely ranked cluster emphasized professional growth and autonomy: networking (160/280; 57%), continued learning (158/280; 56%), independence in work planning (153/280; 55%), and a flexible schedule (152/280; 54%). Third-tier benefits included service/volunteer impact on the profession (135/280; 48%), flexible work locations (125/280; 45%), work–life balance (125/280; 45%), and retirement options (116/280; 41%). Less frequently selected items included the roles not being physically demanding (99/280; 35%), tuition benefits (92/280; 33%), time/energy for family (91/280; 33%), and time/energy for self-care (50/280; 18%). Interpreted together, respondents value these roles primarily for others-centered, mission-driven impact and professional development with real autonomy, rather than for material perks or personal wellness gains. The sacrificial nature of RTs turned educators was apparent in the least reported benefit of not having the time and energy to dedicate to self-care. This finding is somewhat unsurprising given the rates of burnout within the profession as a whole (as high as 79%). 19 Heightened job-related stress, heavy workloads, staffing shortages, and perceived lack of leadership support can result in a loss of energy to dedicate to oneself in both the clinical environment and higher education. Though not specifically asked within this study, many RT educators hold clinical-track faculty appointments, which one study found to have higher reported rates of burnout. 20 Clinical-track faculty members tend to focus on teaching clinical skills and maintaining professional practice acumen, whereas tenure-track faculty have higher research requirements within their respective academic workloads. Administrative appointments as key personnel could also contribute to this phenomenon.
A notable observation is the gap between the mission-first benefit (95%) and the next tier of benefits (45–57%). Networking, continued learning, and service/volunteer learning were all viewed positively among this sample of key personnel. There is an opportunity to use these findings to our collective profession’s advantage to help recruit and retain RTs into academia. For example, independence in work planning, a flexible schedule and work location, and the ability to achieve some semblance of work–life balance were all reported benefits of serving as key personnel. While research on why RTs enter or leave academia is scarce, evidence suggests that allied health professionals, particularly younger cohorts, value flexibility in work conditions, career-advancement opportunities, and work–life balance. Meeting these expectations may attract professionals to academic respiratory care and support retention.13,14 Additionally, perceived organizational support for PDs and DCEs appears to be a key factor in commitment to the organization. 15 Though self-care is undoubtedly important, it is also not uncommon or unpredictable to have increased responsibility, autonomy, and role demands (and subsequently salary) as one rises through the ranks of leadership.
Though there were no significant role differences observed for administrative release time (P = .14), it was noted that 36% of key personnel reported 0–20%. It is important to mention that the CoARC Entry into Professional Practice Standards is currently undergoing a significant revision. The revision proposes a minimum threshold of 25% release in workload to ensure sufficient time to dedicate to performing these administrative functions for both key personnel roles. 16 If this revision is approved and adopted, the institutional sponsor will need to be aware of this requirement and adjust faculty workloads to remain compliant with the applicable standards. Approximately two-thirds of respondents indicate a salary of ≥ $75,000 per year. This finding is encouraging in that it is comparable to the current median ($80,450) annual wage for the profession. 1 Key personnel’s salary is typically commensurate with experience in the profession and as an educator and is partly determined by the geographic location of the sponsoring institution. It is important to note that in comparing the salary of RT key personnel to that of any other PD or DCE in higher education, pay differences usually stem from the expected wage of the respective discipline. Interestingly, 93% of participants responded “no” to the question “Do you feel that you have developed/grown as a leader since becoming key personnel”?, yet there were 267 responses for ways they felt they had developed/grown as a leader. It is possible that participants were demonstrating humility in that they do not wholly view themselves as leaders, despite notable leadership roles inside and outside their academic institutions. Humility is an important leadership characteristic and can contribute to the team’s collective success. 17 Perhaps, because the profession also delineates specialty areas into Education or Leadership and Management, they do not view themselves in the traditional sense of the term. Leadership development of RT educators could be a potential area of future research to better understand this finding.
In our sample, DCEs appeared to be earlier in their academic career (more likely to have completed the KPA and to be pursuing additional degrees). In contrast, PDs were typically later-career, with longer practice tenure, higher academic credentials, and higher rates of promotion and salary. Because program type, degree mix, region, and release time did not differ by role, these differences most likely reflect experience and education rather than institutional placement. To our knowledge, this is the first study to characterize why RTs value key personnel roles and how PD and DCE profiles differ. The main takeaway is straightforward, as respondents chose these roles to shape the next generation of RTs, an emphasis that aligns with broader health-profession motives to help and serve.11,12
Limitations
Several limitations were present in our study. The primary limitation is the response rate, which was 35%, though sufficient power was achieved. While the data provides valuable insights and the sample was proportionally representative of the known population in terms of degree and program type, the perspectives of non-respondents remain unknown. Those who chose to participate may differ in meaningful ways from those who did not, introducing the potential for nonresponse bias. Additionally, the structure of the profession means that some key personnel serve in dual roles, and some institutions offer multiple degree-level options. These overlapping roles and institutional variations are reflected in the data and may limit the ability to make clean, role-specific comparisons. Despite these limitations, the sample reflects the demographic and professional profile of the larger key personnel population, supporting the generalizability of the findings to academic respiratory care settings. Another limitation was the survey design. One survey item permitted participants to answer a follow-up question on leadership development growth even when 93% had responded “no” to the initial question, potentially introducing inconsistencies in reporting leadership growth opportunities.
Conclusions
This study provides one of the first comprehensive examinations of key personnel in CoARC-accredited respiratory care programs. There are important distinctions between PDs and DCEs, as well as the benefits most valued in these roles. The findings reveal PDs are more likely to hold advanced academic credentials and report higher salaries and promotions, while DCEs are earlier in their academic trajectory, are more likely to be pursuing advanced degrees, and more frequently complete the CoARC KPA. Despite these differences, both roles share a common motivation around the opportunity to positively impact the profession by educating future RTs. While respondents report professional networking, autonomy, and continued learning as meaningful benefits, fewer perceived gains in work–life balance and self-care, reflecting the competing demands of a key personnel role. This underscores a critical area for improvement in recruitment and retention strategies for younger professionals entering academia who increasingly value flexibility and work–life balance. Ultimately, the sustainability of RT education depends on attracting and retaining qualified faculty who are well-supported in both professional and personal well-being. It is important to strengthen pathways into academic leadership and to address barriers to faculty retention to ensure stability and continued advancement of respiratory care education.
Supplemental Material
Supplemental material - Characteristics and perceived benefits of key personnel in CoARC-accredited respiratory care programs
Supplemental material for Characteristics and perceived benefits of key personnel in CoARC-accredited respiratory care programs by Kristen L. McHenry, Nicholas Prush, J. Brady Scott in Respiratory Care Reports
Footnotes
Author contributions
All authors contributed to the literature search, data collection, study design, data analysis, manuscript preparation, and review of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the George G. Burton, MD, Educational Research Scholarship awarded by the Commission on Accreditation for Respiratory Care (CoARC). The CoARC had no role in the design, analysis, or interpretation of findings for this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosure statement
Drs. McHenry, Prush, and Scott disclose that they are Commissioners and site visitors for the Commission on Accreditation for Respiratory Care (CoARC). Drs. Scott and McHenry also disclose research funding from the American Association for Respiratory Care.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.