
Abstract
Paediatric allergic disorders are among the most common chronic conditions affecting children’s quality of life and their prevalence is steadily increasing. This is a qualitative study in the form of a service evaluation on the quality of care of children with allergies who were followed up at a Paediatric Allergy Clinic between June 2021 and June 2022. The study found that 76% of patients had been diagnosed with allergies. Parents of 81% of patients rated their overall satisfaction with the allergy service as 5/5 (very satisfied) or 4/5 (satisfied) and 91% of parents reported clear communication regarding their children’s allergies. Key areas for improvement identified includes managing long waiting times, increasing allergy information availability to parents and better communication regarding allergy appointments. Overall, the majority of the parents were satisfied with the quality of care that their children received, with specific areas for improvement being identified.
Introduction
Paediatric allergic disorders are one of the most common chronic conditions affecting 30% to 35% of children in the developed world. 1 The prevalence and incidence of allergic disorders are increasing globally 2 with a notable increase in hospital admissions due to anaphylaxis in the UK between 1998 and 2018. 3 While the exact aetiology for this increase is unknown, 4 it may be related to genetic predisposition, environmental factors or cultural background. 5 Up to one third of all children are affected by allergic disorders both globally 6 and in the UK. 7
Paediatric allergy services have increased over the years, but many are small and vary widely by region. 8 West Midland studies have shown that parents strongly prefer to see formally trained specialist allergy clinicicians 9 in comparison to those with no formal allergy training. Parents also find it challenging to access appropriate advice in both primary and secondary care services in a timely manner. 10 Studies have positively evaluated the impact of General Practitioner and Primary Care led community Paediatric Allergy Clinics through demonstrating reduced referral burden and patient visits to secondary care clinics.11,12 Furthermore, UK based studies have shown appropriately trained allergy personnel in primary care, allow patients to be seen in a timely manner and closer to home. 12
Due to the increasing prevalence of allergic disorders and the impact that they can have on the quality of life of these patient, timely access to allergy testing and an early diagnosis are vital for optimal care of allergies in children. 13
Ysbyty Gwynedd is a District General Hospital that serves the population of Gwynedd and Ynys Mon in North Wales, with ~40 000 children and young people under the age of 18 years. The Paediatric Allergy Service is run by 3 General Paediatricians with special interest in paediatric allergy alongside a team undertaking allergy blood tests, skin prick tests, food challenges and providing training of adrenaline autoinjector care plans to the families where it is indicated.
Few studies have examined the quality of care provided to patients by paediatric allergy services especially at the District General Hospital or peripheral hospital level. The aim of this study is to provide a better understanding of the quality of care received by paediatric patients under follow up of the allergy service in a District General Hospital in North Wales to inform further reforms and improvements to the service.
Methods
This is a qualitative study in the form of a service evaluation on the quality of care of children with allergies. This qualitative survey was conducted using a specifically designed questionnaire by these authors based on their experience with the allergy service in Ysbyty Gwynedd. The questionnaire was conducted by the first author by telephone. The duration of the interview differed on the time taken to answer the questionnaire lasting between 5 and 20 minutes. The Questionnaire (Supplemental Appendix 1) consisted of a combination of closed and open questions with participants being given the opportunity to add any additional information that they felt was relevant to their experience with the allergy service.
All parents of patients under follow up at the paediatric allergy service who attended clinic appointments between June 2021 and June 2022 were invited to participate in this study. Interviews were conducted on weekdays between May 23, 2022 and June 14, 2022, after verbal consent was gained to participate in the study. Written consent was not obtained, no patient identifiable information was obtained or included within the study. Patient responses were collected anonymously and compiled in an Excel spreadsheet. Participants were contacted up to 5 times for a response. Interviews were not audio- or video-recorded, and repeat interviews were not conducted. This study did not require ethical approval.
The study included all children with a diagnosis of allergy identified from our outpatient clinic list. Diagnosis was based on a comprehensive allergy-focussed history, incorporating features of both IgE- and non-IgE-mediated reactions, in line with NICE and European Academy of Allergy and Clinical Immunology (EAACI) guidelines. Children with suspected IgE-mediated food allergy underwent objective testing, either serum total and specific IgE measurement or skin prick testing. Where feasible, skin prick testing was the preferred modality in cooperative children. Following discussion with parents, serum IgE testing was used when skin prick testing was not suitable, particularly in younger or less cooperative children who were unable to keep their forearm still, or when multiple food allergies were suspected, as this allowed assessment using a single blood sample rather than multiple skin pricks.
Results
A total of 100 patients who attended allergy clinics between June 2021 and June 2022 were identified. These parents were contacted by telephone, and 75 completed the questionnaire. Of the remaining 25, 3 declined participation and 22 did not respond or were unavailable at the time of contact.
From the patients that were included in the study 35% (n = 26) were females and 65% (n = 49) were males (Table 1).
Age and Sex of Patients Who Participated in the Questionnaire.

This table shows that nearly 50% more of the persons attending allergy clinic were male (65%-35%), and that male attendance under 5 was particularly high compared to the other ages.
The results showed that 76% (n = 57) of patients had received an allergy diagnosis. Reasons for not having an allergy diagnosis included diagnosis pending on test results, or no allergy being diagnosed. The majority of allergy diagnoses, 77% (n = 44) were made during the first clinic appointment, with 19% (n = 11) at the second visit (Figure 1).
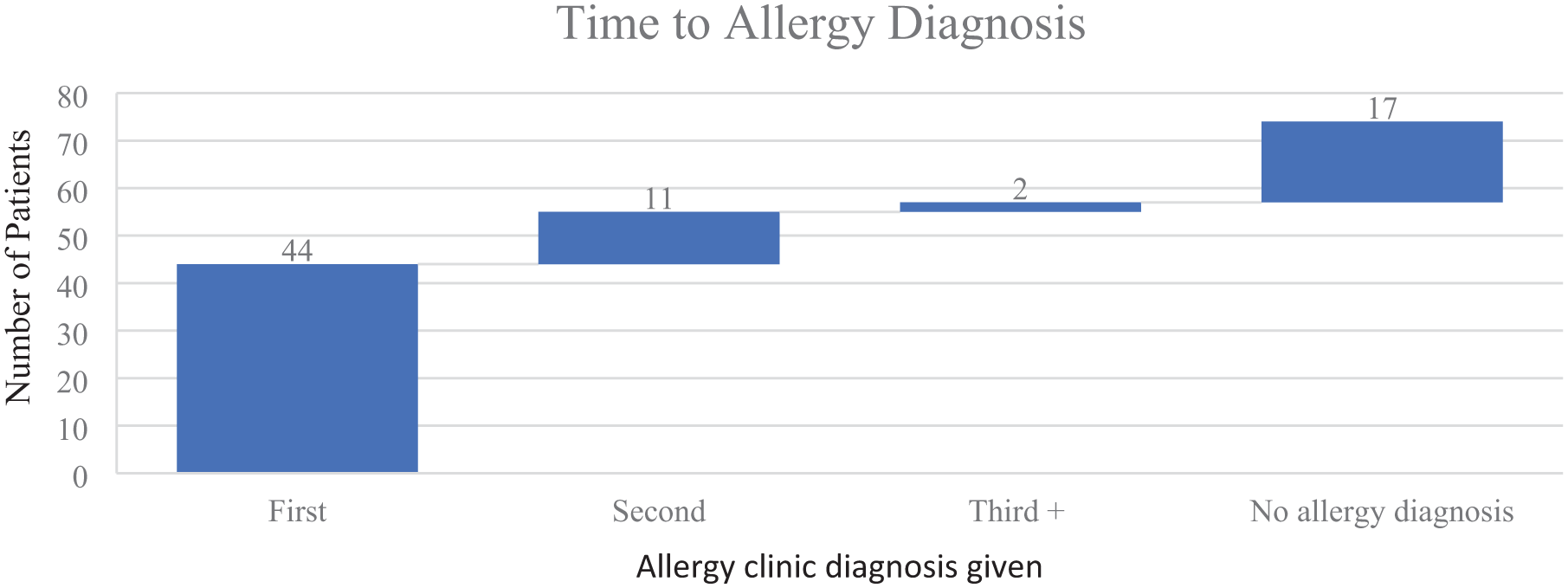
Time for allergy to be diagnosed.
Among those with a confirmed diagnosis, 23 (35%) had a single food allergy and 35 (60%) had multiple allergies; Table 2 summarises the distribution of allergy types within the study cohort.
Breakdown of Allergy Diagnosis.

This table shows the breakdown of allergies seen in the allergy clinic.
On attendance to allergy clinic 65% (n = 49) received allergy focussed blood tests and 39% (n = 29) underwent a skin allergy test.
At the allergy clinic there are 3 health care professionals working together; doctors, allergy nurses and dieticians. Doctors saw 97% (n = 73) of patients, whereas the allergy nurse saw 24% (n = 18) and dietician 29% (n = 22; Table 3).
Health Care Professionals Interacted With at the Allergy Clinic.

This table shows the breakdown of how many patients had access to the 3 health care professionals making up the allergy clinic MDT. This suggests greater use of the dietician and nurse allergy specialist could be beneficial.
Of those that attended the allergy clinic 68% (n = 51) were started on a treatment plan while 32% (n = 24) were not given a treatment plan/ were told that they did not require medical management of their allergies. Of those that were started on medical management including antihistamines 10% (n = 5) experienced side effects of feeling drowsy/tired. No other side effects were reported.
Adrenaline autoinjectors (AAI) were carried by 26% (n = 20) of patients with severe allergy symptoms. Of those who carried AAIs 90% (n = 18) said they received training using a trainer AAI pen and 85% (n = 17) received patient information leaflets about AAIs. All patients prescribed an Adrenaline Autoinjector confirmed they knew their child’s allergy treatment plan.
When asked about communication around allergies, 91% (n = 68) of the parents stated that communication was clear, 56% (n = 42) received patient information leaflets and 83% (n = 62) felt that they had enough information about allergies. Schools of 17% (n = 13) of patients had been informed of the child’s allergies by the allergy team and 0% (n = 0) of the patients had been put in contact with allergy support groups.
The strengths of the allergy service are listed in (Table 4) and the areas for improvement within the allergy service are listed in (Table 5).
The Strengths of the Allergy Service.
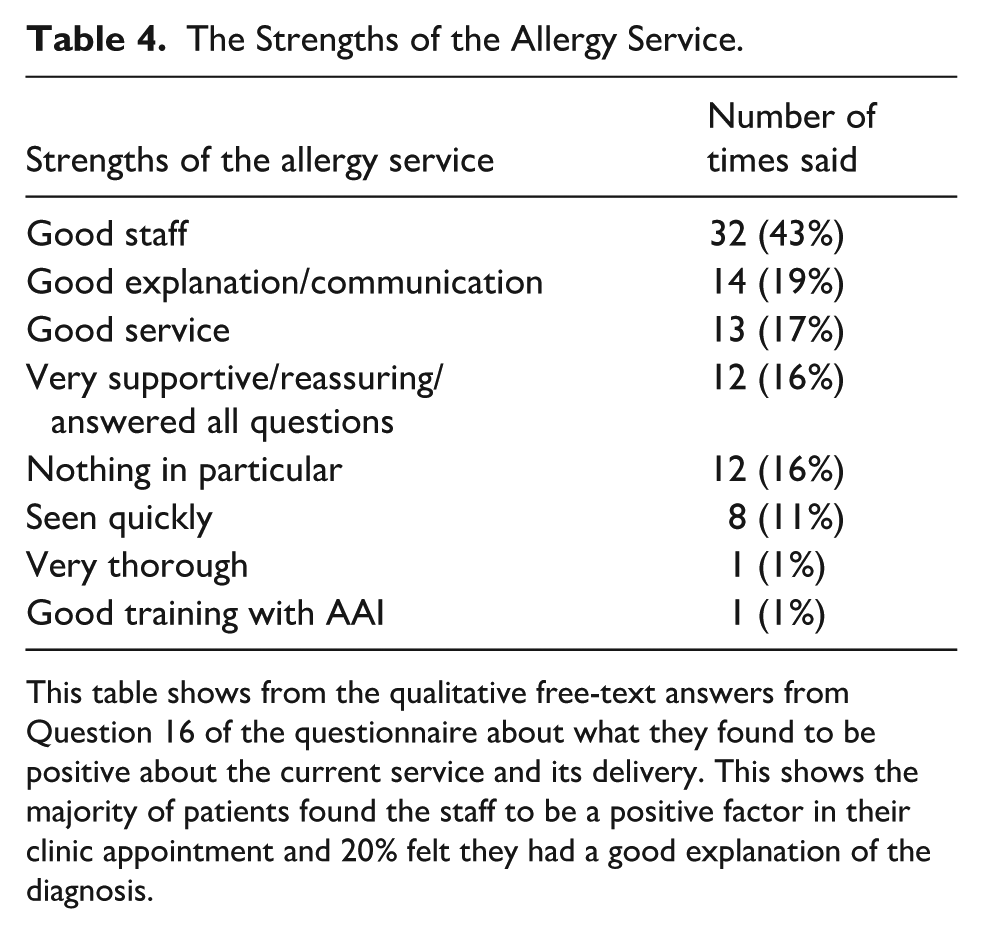
This table shows from the qualitative free-text answers from Question 16 of the questionnaire about what they found to be positive about the current service and its delivery. This shows the majority of patients found the staff to be a positive factor in their clinic appointment and 20% felt they had a good explanation of the diagnosis.
Qualitative Feedback on Areas for Improvement for the North Wales Allergy Service.

This table shows all the comments and opinions from the parents attending the allergy clinic on where they felt the service could be improved. We acknowledge wait times being one of the most common, however the impact from COVID-19 was still prominent at this time. This table shows the qualitative feedback from patients’ parents on what they felt could improve the service in the free-text Question 17. This shows that 36% felt that there were no areas for improvement, which was higher than expected. However, 31% felt that the wait times were the largest area for improvement. The other main areas for concern are shown to be further testing, and better communication outside of the clinic room in the forms of more information, support groups and a range of communication media.
Following on from Question 17 in the survey, Parents of patients were asked how they would rate their experience with the allergy service on a scale of 1 to 5 with 1 being very unsatisfied and 5 being very satisfied. One percent (n = 1) chose 1, 4% (n = 3) chose 2, 13% (n = 10) chose 3, 33% (n = 25) chose 4 and 48% (n = 36) chose 5. We found that parental perspectives were not influenced by disease severity or whether the allergy was single or multiple. Those who rated the service 3 or below, have had their areas for improvement listed below (Table 6).
Areas for Improvement Expressed by Those Who Rated Their Experience With the Allergy Service as 3 or Below.

Patients were given a score of 1 to 5 to rate their experience of the North Wales allergy service. 1 was very unsatisfactory, 5 was very satisfactory. For those who felt it was neither good or bad, or bad, further analysis of their common experience and free-text answers is provided here. The most common themes were long wait times and feeling that more information would be helpful.
Discussion
This service evaluation examined the quality of care of patients during the follow up of paediatric allergy clinics at Ysbyty Gwynedd in North Wales through a tele-questionnaire. This allowed us to gain insight into the patients’ experience with the allergy service.
A survey conducted in 2002 and repeated in 2009 showed that GPs perceived allergy care in the NHS as poor. 14 The GPs felt that the quality of care given for allergies in primary and secondary care was poor, with limited access to Allergy specialists. This reflects the feeling expressed by the parents to see an allergy trained specialist within this survey and others.9,11 Therefore, further educational opportunities for GPs on allergies could prove very beneficial, and as previously shown primary care allergy services delivered by appropriately trained personnel can reduce inappropriate secondary referrals and encourage local community-centred care. 1 Similarly, only 29% of patients saw a dietician at allergy clinic, but from the feedback received, patients who has not seen the dietician would have liked too. Therefore, an even greater MDT approach to the North Wales Allergy Service Clinic appointments could be a beneficial improvement for patient understanding and holistic approach.
Despite implied long wait times from the questionnaire, 76% were diagnosed within 1 appointment, which provides answers and allows for swift implementation of prevention strategies and prescription of AAIs if needed. Importantly all parents with children with allergies severe enough to require an AAI were aware of their child’s treatment plan, however further communication around management of milder allergies with antihistamines and symptomatic relief could be improved.
The majority of allergy diagnoses were made during the first clinic appointment, however 19% were diagnosed at the second visit as they were often waiting for the results of blood or skin tests. In comparison, another study conducted in the UK showed that 1 in 3 respondents required 4 or more visits to healthcare professionals to secure a diagnosis. 7 This is reflected in the overall high satisfaction with the allergy service, with 81% of respondents rating their experience as either 5/5 (very satisfied) or 4/5 (satisfied), highlighting the strengths and efficiency of the North Wales Allergy Service.
These findings are consistent with and build upon the research of and mirror the research of Gore et al, who in the UK in 2016, reported 71% of parents rated their allergy care to be good/excellent. 7 This suggests a gradual improvement, over time, in allergy services in the UK.
A study on the influence of a multidisciplinary paediatric allergy clinic on parental knowledge and the rate of subsequent allergic reactions showed significant improvements in the management and prevention of allergic reactions to food after 1 allergy clinic appointment. 15 This was reflected in our study when parents highlighted clear communication as one of the benefits of the allergy service.
Long waiting times, largely due to a reduction in clinic consultations during the COVID-19 pandemic, was the most frequently mentioned area for improvement in our allergy service. This was highlighted by nearly all participants who rated their experience 1 to 3 out of 5. A study on allergy services in the West Midlands, however, shows that the difficulty of accessing allergy services and being seen in a timely manner is a common, and widespread issue. 10 Parents also mentioned appointment cancellations, and administrative issues including difficulties with receiving appointments in the post, not receiving results, and desires for electronic communications. This area should be prioritised for improvement. Offering a text, email and letter service for communication, along with results being available online with the NHS app, should help improve these technical errors and improve parent satisfaction. Unfortunately, wait times is a chronic problem for the NHS post Covid, we would recommend more staff training or clinics, if possible, to help ease the waitlist times.
Other areas for improvement highlighted by the questionnaire were that only 55% of the patients received information leaflets about their allergies, only 17.33% of the schools were informed of the child’s allergy and no one was put in contact with support groups.
Due to the rapid and potentially life-threatening nature of anaphylaxis, schools must be promptly informed of any allergy diagnosis. Clear responsibility should be established—either with the allergy clinical team or with parents—particularly when an AAI is prescribed, as schools may not always have spare devices or trained staff available. 16 A study in Sweden looking at the consequences of an allergy diagnosis on patients and their families also identified a lack of understanding of allergies in schools and preschools. 17 Additionally, only 90% of the parents recalled having AAI training, which potentially highlights a need for more thorough training or perhaps refresher courses to be completed after diagnosis.
Although parents of patients perceived that they had not been provided access to allergy support groups, many were verbally informed about support groups on the Northwest Allergy Network and the Allergy UK websites. However, it is evident from our findings that this information was not adequately retained to the patient, and an information sheet may also be beneficial that they can read at a later date.
The limitations of this study include not able to complete the interview with a quarter of the initial study population. As this study did not contain information on the patients where the parents declined to participate or were unable to participate, there is a possibility that those parents may have had different experience with the allergy service. Furthermore, the waitlist times were not investigated which limits our ability to measure service delivery and improvement (Supplemental Material).
Another limitation of this study is that the questionnaires were developed by the authors for the purpose of this study. The questionnaire was not pilot-tested prior to use in this study.
Overall, the parent’s experience of the North Wales Allergy Clinic is positive. A few areas of improvement have been identified which include attempts to reduce referral waitlist times, increase available information and training on allergies, developing more communication channels between the clinic and the families and a greater MDT approach to allergy management. Furthermore, seeking additional funding to support training more allergy specialists within the North Welsh community would be greatly beneficial.
Our findings are not unexpected and instead reiterate the common themes found in other studies on paediatric allergy service. This highlights the importance of involving parents in the development and implementation of paediatric allergy services. Future studies could also explore parental preferences for different allergy service models, along with strategies to reduce waiting times, could provide valuable insights into improving parental satisfaction.
Conclusions
Overall, most parents were satisfied with the quality of care that they received. The feedback received from this study highlights key areas for improvement and will enable further development of the existing paediatric allergy services.
Supplemental Material
sj-docx-1-gph-10.1177_30502225261424331 – Supplemental material for Parent Perspectives on the Quality of a Paediatric Allergy Service in North Wales
Supplemental material, sj-docx-1-gph-10.1177_30502225261424331 for Parent Perspectives on the Quality of a Paediatric Allergy Service in North Wales by Abby Fayen, Genevieve Harvey and Manohar Joishy in Sage Open Pediatrics
Supplemental Material
sj-docx-2-gph-10.1177_30502225261424331 – Supplemental material for Parent Perspectives on the Quality of a Paediatric Allergy Service in North Wales
Supplemental material, sj-docx-2-gph-10.1177_30502225261424331 for Parent Perspectives on the Quality of a Paediatric Allergy Service in North Wales by Abby Fayen, Genevieve Harvey and Manohar Joishy in Sage Open Pediatrics
Footnotes
Consent to Participate
Informed verbal consent from legally authorised representatives to take part in this study.
Author Contributions
AF contributed to conception and design, contributed to analysis, drafted the manuscript, critically revised the manuscript, gave final approval, agrees to be accountable for all aspects of work ensuring integrity and accuracy. GH contributed to conception and design, contributed to analysis, critically revised the manuscript, gave final approval, agrees to be accountable for all aspects of work ensuring integrity and accuracy. MJ contributed to conception and design, contributed to analysis, critically revised the manuscript, gave final approval, agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data Availability Statement
Data is available in the appendix below.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.