
Abstract
This cross-sectional study was aimed to find out prevalence of diabetes and prediabetes and associated factors among school going children in Bangladesh by multistage sampling. Data were collected through face-to-face interview using a semi-structured questionnaire and blood sample was collected by laboratory technologist. Data were verified and analyzed using SPSS. Informed written consent and assent was obtained. Ethical issues were maintained. The prevalence of diabetes was 0.09% (3/3342) and prevalence of prediabetes was 0.569% (19/3342). Female gender (AOR: 2.8, CI: 1.1-7.2, P = .03), family history of diabetes among 1st-degree relatives (AOR: 4.7, CI: 1.6-14.2, P = .006), obesity (AOR: 65.91, CI: 8.7-499.9, P < .001) and comorbidities (AOR: 4.09, CI: 1.1-15.9, P = .04) had higher chance for diabetes & prediabetes. Gestational Diabetes mellitus was an independent risk factor (COR: 9.25, CI: 1.2-72.7, P = .034). This provided epidemiological data for development of a screening protocol for children.
Introduction
Noncommunicable diseases (NCDs) represent a significant health challenge globally, characterized by long-term health implications requiring prolonged treatment and care. These diseases, including cancers, cardiovascular diseases, diabetes, and chronic lung diseases, have substantial economic implications, particularly in developing countries like Bangladesh. Among the NCDs, diabetes imposes a significant burden on public health systems worldwide. The epidemic of diabetes is a major concern, with a staggering 537 million people affected globally, including 90 million in Southeast Asia alone and projections indicate that by 2045, these numbers will rise to 783 million globally and 151.5 million in Southeast Asia. 1 Besides it has been found that diabetes is not only highly prevalent in adults but also has been increasing among the youth, particularly type 2 diabetes mellitus (T2DM). In the United States, the incidence rates of T2DM among 10 to 19 years old youths have risen by 7.1% annually. 2 This trend is mirrored in some countries of Asia like Japan and Taiwan.3,4 In Africa, the incidence and prevalence of DM are also shown to be on the increase among children and teenagers. 5 In Bangladesh, individuals are predisposed to develop diabetes at an early age, with Asian youths, in particular, exhibiting a higher prevalence of T2DM, often with a lean body mass index compared to European counterparts, due to genetic factors such as reduced beta cell function. 6 Furthermore, lifestyle changes associated with rapid urbanization and adoption of Westernized diets contribute to the increased prevalence of diabetes, including childhood diabetes, in Bangladesh. 7
Although type 1 diabetes mellitus (T1DM) remains the main form of the disease in children worldwide, type 2 diabetes has become an increasingly important public health concern globally among children in high-risk ethnic populations.2,8 The early onset of T2D in children makes lifetime exposure to hyperglycemia longer and consequently causes a greater risk for long-term complications. Early diagnosis of diabetes is critical for effective management and prevention of complications. Children with prediabetes, an intermediary and reversible condition preceding T2DM, benefit from timely interventions by maintaining a healthy lifestyle thus reducing the risk of developing diabetes and related complications. 9
A recent hospital-based study showed a mean T1DM incidence of 1.25/100 000 population in Dhaka District among participants with <20 years of age. 10 The number of children with type 2 diabetes increased more than 7-fold from 2010 (2%) to 2015 (14%) found in a study done in BIRDEM Hospital. 11 Given the limited population-based data on children with diabetes and prediabetes in Bangladesh, this study aims to assess the prevalence of diabetes and prediabetes, along with associated risk factors, among school going children in Bangladesh.
Subject, Materials and Methods
Study Design & Place
This cross-sectional study was conducted in all geographic areas of 8 divisions of Bangladesh from August 2022 to August 2023.
Study Population
School going children, aged from 5 to 17 years, were the study population. Participants of the study were students who met the following criteria (1) Aged from 5 to 17 years (2) Both male and female children (3) Who`s legal guardian gave informed written consent (4) Children who gave assent to participate in the study. Students who did not meet the inclusion criteria, who wished to withdraw from the study or who had an acute illness (fever, infection) were excluded from the study.
Sample Size
The sample size was calculated considering the prevalence of impaired fasting glycemia (IFG), relative precision rate (20%), and feasibility of the survey. The design effect and non-response rate were also considered to calculate the final sample size. The final study sample size was 3697.
Sampling & Data Collection Technique
The study was conducted through a multi-stage sampling technique. All 8 divisions of Bangladesh were included in this study. One district was selected from each division by a simple random sampling technique. From each district, a list of 20 schools had been prepared and from those, 2 schools from each district had been selected by simple random sampling technique. Then by seeking proper permission from schools, a list of the total students from each school was prepared, and again by simple random sampling technique, approximately 230 to 232 students were selected from each school and thus approximately 461 to 462 samples were selected from each division. Data were collected by using a semi-structured questionnaire through face-to-face interview and at the same time capillary blood sample was also collected by laboratory technologist to measure the fasting blood glucose level using a glucometer. Socio-demographic, socio-economic, diabetes-related data, anthropometric data, etc. were included. The children were advised to have at least 8 hours of fasting before giving a blood sample. Then blood samples (fasting capillary blood glucose) and data were collected in the morning from the school. The fasting capillary blood glucose of the participants was measured by a glucometer for screening diabetes and prediabetes. Diabetes and prediabetes were diagnosed according to the American Diabetes Association and International Society for Pediatric and Adolescent Diabetes (ISPAD) criteria. 12 Impaired fasting Glucose (IFG) was defined as blood glucose (BG) between 5.6- 6.9 mmol/l (100-125 mg/l) and diabetes if fasting BG ≥7 mmol/l (126 mg/dl). In case of a positive screening test by glucometer at school for prediabetes (impaired fasting blood glucose) or diabetes, further evaluation was done by oral glucose tolerance test (OGTT) on a separate day at the nearest diabetes center to confirm prediabetes (impaired fasting glucose and/or impaired glucose tolerance) and diabetes. During the test of oral glucose tolerance, the test load for glucose was 1.75 gm per kg of body weight (max 75 g) for children. In this study, prediabetes was defined as the fasting blood glucose between 5.6 to 6.9 mmol/l or blood glucose level after 2 hours of taking 1.75 gm kg of body weight (max 75 g) glucose between 7.8-11.0 mmol/l. In addition, diabetes was defined as fasting blood glucose (FBG) level ≥7.0 mmol/l or blood glucose level after 2 hours of taking 1.75 gm per kg of body weight (max 75 g) glucose ≥11.1 mmol/l. The type of diabetes (type 1, type 2, or other type of diabetes) was confirmed by the physician by further examinations, clinical criteria, and C-peptide level.13,14
Blood pressure was measured by a mercury sphygmomanometer. Weight was measured using a bathroom scale to the nearest 100 g. Standing height was measured with a stadiometer and measurement was done to the nearest 0.1 cm.
Statistical Analysis Plan
Data were collected, checked, verified, and compiled using SPSS software (version 25). Data were expressed by descriptive and inferential analysis. Descriptive analysis was described using frequency, mean, and standard deviation. The association was revealed by inferential analysis and primary comparison was made between children who were diabetic & prediabetic and non-diabetic. Initial comparison was described by using the chi-square test and further logistic regression was done among the significant associations among gender, DM in 1st degree relatives, GDM, having comorbidities and BMI.
Ethic Statement
Ethical approval was obtained from the ethical review committee of the Diabetic Association of Bangladesh (BADAS) with the approval number (Memo: BADAS-ERC/EC/22/393) before the commencement of the study. Informed written consent from parents and respective guardians of all participants and assent from 12 to 17 years aged children were obtained. Privacy and confidentiality of data were maintained strictly. All ethical considerations were maintained properly.
Results
A total of 3697 children were interviewed for the study. Among them, 355 were excluded from the study as they had taken breakfast. The remaining 3342 participants were taken as the final sample size, and they were interviewed, and blood samples were collected from them.
Among the total participants (3342), male students were predominant (54.3%). Most of the students (45.99%) belonged to the age group of 13 to 14 years and most of the students (72.6%) came from urban areas. Besides, most of the participants (86.12%) hailed from nuclear families. (Table 1). The mean age for all participants was 13.64 ± 1.512 and the mean BMI for all participants was 19.60 ± 18.666.
Distribution of Sociodemographic Variables Among Total Participants.
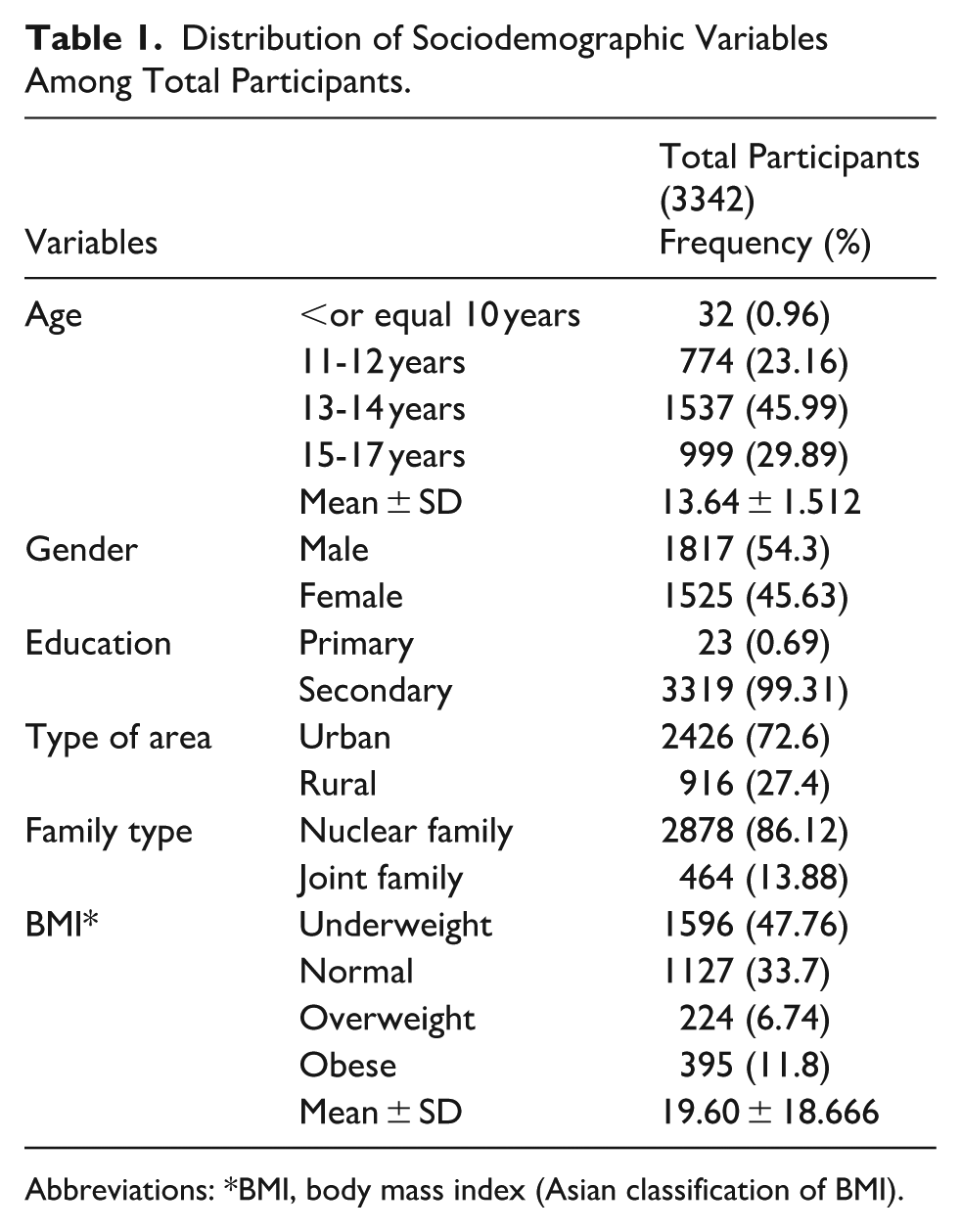
Abbreviations: *BMI, body mass index (Asian classification of BMI).
Many participants (52.51%) had no DM among the first-degree relatives. One hundred and two (3.05%) participants had other disease conditions, like thyroid disease, anxiety neurosis, polycystic ovarian syndrome (PCOS), etc. It was observed that carbohydrate and junk food intake were high among the participants. It was observed that most of the participants (80.9%) had a history of screen time for more than 2 hours. (Table 2).
Distribution of DM-Related, Food-Related, and Lifestyle-Related Variables Among Total Participants.

Among the total 3342 participants, 3173 (94.94%) participants were found as screened negative participants whose fasting blood glucose level was less than 5.6 mmol/l, and the rest 169 (5.06%) participants had more than 5.6 mmol/l fasting blood glucose level and were identified as screened positive participants. These 169 participants were further evaluated by OGTT. Among them, 3 (1.78%) were found to be diabetic, and 19 (11.24%) were found to be pre-diabetics. As the total diabetic cases were 03 and the prediabetic cases were 19, the prevalence of diabetes was 0.09% or 90 per 100 000 population and the prevalence of prediabetes was 0.569% or 569 per 100 000 population (Figure 1).

Flow chart of detecting diabetic and pre-diabetic participants.
The mean of fasting capillary blood glucose for the 03 diabetic children was 12.17 ± 5.83 and mean of fasting blood glucose at OGTT was 8.80 ± 3.27 and the mean of blood glucose level after 2 hours of taking 1.75 gm kg of body weight (max. 75 g) glucose was 15.95 ± 3.27. The mean of fasting capillary blood glucose for the 19 prediabetic children was 6.54 ± 1.40 and mean of fasting blood glucose at OGTT was 5.80 ± 0.369 and the mean of blood glucose level after 2 hours of taking 1.75 gm kg of body weight (max 75 g) glucose was 7.70 ± 1.11. The type of diabetes was further evaluated by C-peptide level, history, and clinical examination done by a physician, and all 03 diabetic children were found to have type 2 diabetes (Not included in the table).
Among the diabetic and prediabetic participants, most children (68.2%) were female but among the nondiabetic participants, most (54.5%) were male. The presence of DM in families was higher in diabetic and prediabetic groups than in non-diabetic groups (81.8% vs 44.7%). Moreover, 4.5% of diabetic and prediabetic children had a maternal history of GDM. It was found that gender, BMI, having comorbidities, and DM among 1st degree relatives were associated with development of diabetes and prediabetic conditions among children (P < .05; Table 3).
Distribution of Associated Risk Factors Among Diabetic & Prediabetic Participants.

Abbreviations: *BMI, body mass index (Asian classification of BMI).
Comorbidities: thyroid disease, anxiety neurosis, polycystic ovary syndrome, etc.
On the contrary, any food intake (like carbohydrate intake, protein intake, or junk food intake), or screen time was not found statistically significant (not included in the table).
Both bivariate and multivariate analysis showed that female gender, family history of diabetes, having comorbidities (Thyroid disease, Anxiety Neurosis, Polycystic ovary syndrome, etc.), and obesity/overweight were observed to be risk factors for having diabetes and prediabetic conditions among children (P < .05). GDM was also found to be an independent risk factors for diabetes and prediabetes (P = .034; Table 4).
Factors Associated with Diabetes & Prediabetes (n = 22; Regression Table).
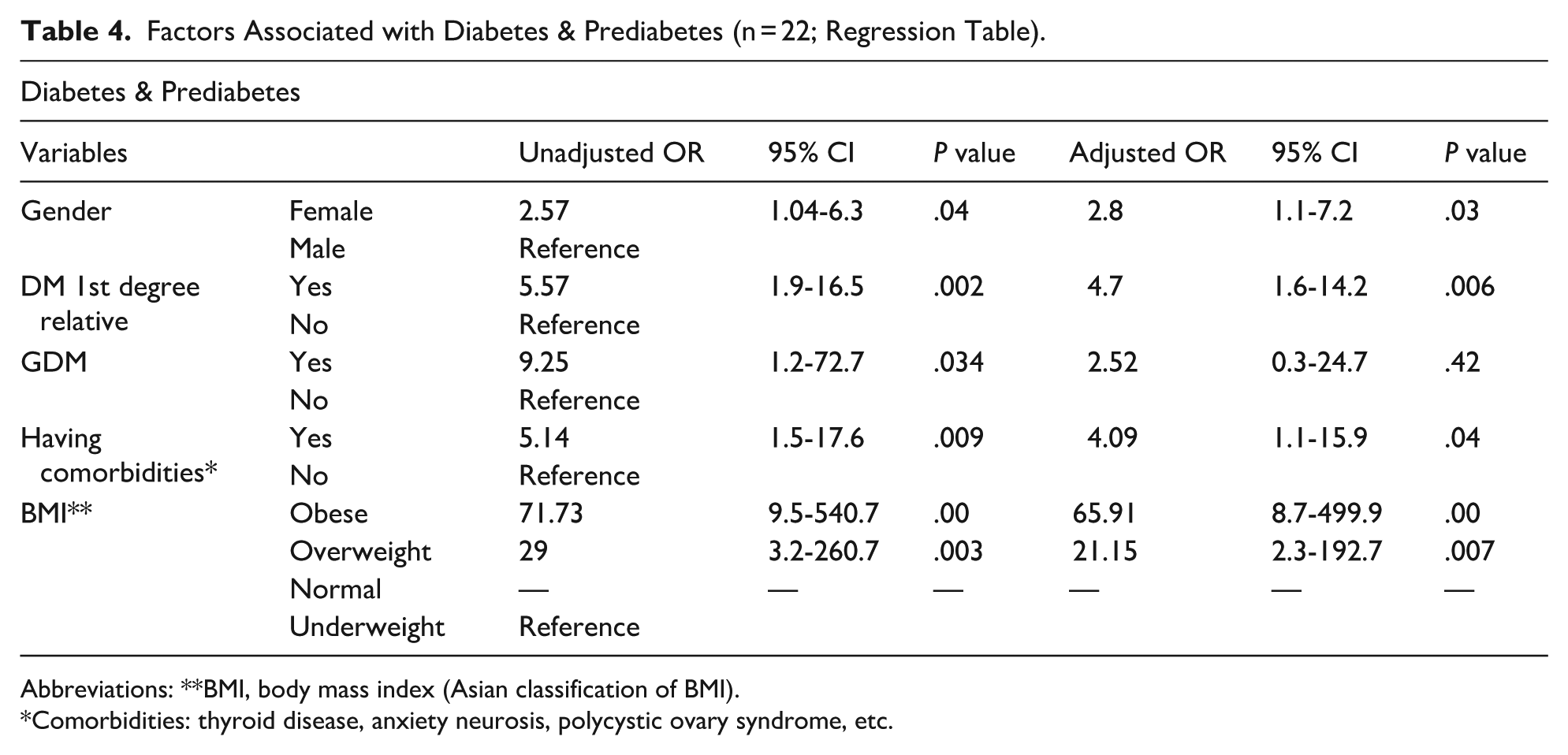
Abbreviations: **BMI, body mass index (Asian classification of BMI).
Comorbidities: thyroid disease, anxiety neurosis, polycystic ovary syndrome, etc.
Discussion
The present study aimed to investigate the prevalence of diabetes and prediabetes among school going children in Bangladesh, along with identifying associated factors. The findings revealed several significant insights into the epidemiology and determinants of these conditions among the pediatric population. Firstly, the prevalence of diabetes and prediabetes among the study participants was noteworthy, In the present study, the prevalence of diabetes among school going children was 0.09%. This prevalence of diabetes aligns with similar studies conducted in Bangladesh and other countries, ranging from 0.07% to 0.1% suggesting a comparable burden of these conditions across different socio-economic settings.15 -17 It was lower than the prevalence among Brazilian school children aged 12 to 17 years in 2013 to 2014 (3.3%), 18 in the USA in 2009 among children aged 10 to 19 years (0.17%-1.2%), in Mysore, India in 2006 to 2007 (0.6%), in Birjand, Iran in 2012 among children aged 6 to 11 years (0.3%), and in Bangladesh among the children aged 10 to 18 years in 2013 (1.8%).19 -22
In this study, all diabetic participants were identified as having type 2 diabetes. A study from Bangladesh indicates a rising trend of type 1 diabetes and however it also suggested that the pattern of diabetes is evolving. 23 Additionally, another study from Bangladesh indicated that the number of children and adolescents with type 2 diabetes is increasing due to the increased incidence of childhood diabetes. 24
Additionally, the prevalence of prediabetic cases in our study was 0.569%. This is comparable to a recent study done in south Dhaka region, Bangladesh (0.6%). 15 However, other studies have reported higher prevalence rates for prediabetes ranging from 1.89% to 22%.17,18,25 -27 These disparities might be attributed to differences in age group, genetic, socioeconomic, nutritional, and environmental conditions. Moreover, methodological differences in studies, study design, case ascertainment methods, etc. might also contribute to substantial variation in results. Rapid urbanization and increased consumption of fast food with a sedentary lifestyle in children might be the risk factors for an increased trend of prediabetes and type 2 diabetes in children.11,13
In our study, a higher proportion of females were diagnosed with diabetes and prediabetes. This finding is consistent with other studies suggesting potential hormonal and lifestyle influences contributing to the higher susceptibility of females to these conditions.7,13
In present study, diabetic and prediabetic participants were within the age group of 13 to 14 years. Pubertal age was found to be associated with diabetes and prediabetes in other studies, likely due to the physiological and hormonal changes occurring during this period, rendering individuals more vulnerable to metabolic disturbances.13,28,29
Obese/overweight children had a higher prevalence rate of diabetes and prediabetes in our study in concordance with other school-based data among children and adolescents.7,14,30 In our study obese children had 65 times higher chances of developing diabetes and prediabetes, so obesity can be explained as an emerging risk factor for metabolic disorder. Though some factors like carbohydrate intake, junk food intake, and screen time of more than 2 hours were not found to be associated with diabetes and prediabetes in our study but these were highly prevalent among the participants. Aside from this, in our study, physical inactivity was not significantly associated with diabetic and prediabetic conditions in children which was different from the findings of another study. 31 The rise in childhood obesity, changes in diet and physical activity, maternal obesity and diabetes, and other factors contribute to the escalating incidence of T2DM. 7 These findings underscore the importance of addressing childhood obesity and a healthy lifestyle as a preventive strategy for mitigating the risk of metabolic disorders.
Family history of diabetes was found to be significant for both diabetes and prediabetes in our study population, which is consistent with findings from other studies.7,32 Gestational diabetes mellitus (GDM) emerged as an independent risk factor for developing diabetes and prediabetes in children in our study. However, in a study conducted in Vietnam, the results regarding GDM differed from ours, possibly due to regional variations and differences in immunology. 16 Nevertheless, GDM has been identified as a risk factor for diabetes in various other studies.32,33 In the present study, the prevalence of diabetes among school going children was 0.09%, indicating that 90 students per 100 000 children were affected by diabetes. Overall, the combined prevalence of diabetes and prediabetes was 0.658%, indicating that 658 children per 100 000 had either diabetes or prediabetes.
Despite the valuable insights provided by this study, it is essential to acknowledge certain limitations. The cross-sectional design restricts our ability to establish causal relationships between identified risk factors and disease outcomes. Longitudinal studies could have offered a more comprehensive understanding of these associations over time. For obtaining sustainable development goals regarding NCD, it is essential to prevent prediabetes and diabetes, especially type 2 diabetes in childhood. The strength of this study is that it covers whole Bangladesh and provides epidemiological data which highlight the emergence of prediabetes and type 2 diabetes in children and adolescents.
Conclusion
This study contributes valuable knowledge to the field of pediatric diabetes epidemiology in Bangladesh. The associated factors may provide a basis for the development of targeted intervention strategies and screening protocols aimed at early detection and prevention of diabetes and prediabetes among school going children.
Footnotes
Acknowledgements
This research received a grant from the Govt. of Bangladesh. All authors contributed to the designing and drafting of the work, data collection, and analysis, in preparation of this report and agreed to be accountable for all aspects of the work. We are grateful to the school authorities for their support during the data collection period.
Ethical Considerations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Ethical approval was obtained from the ethical review committee of the Diabetic Association of Bangladesh (BADAS) with the approval number (Memo: BADAS-ERC/EC/22/393) before the commencement of the study.
Consent to Participate
Informed written consent was taken from all participants before data collection. Privacy and confidentiality of data were maintained strictly. All ethical considerations were maintained properly.
Consent for Publication
All authors approved the manuscript for publication.
Author Contributions
Fauzia Mohsin: Conceptualization, Formal analysis, Methodology, Project administration, Writing-review & editing. Nasreen Islam: Formal analysis, Data curation, Supervision, Visualization. Md. Abdul Baki: Supervision, Data Curation. Tasnima Ahmed: Data curation, Investigation. Shareen Khan: Data curation, Validation, Resources. Amrita Lal Halder: Data curation, Investigation, Software, Validation. Bedowra Zabeen: Review and editing. Jebun Nahar: Data curation, Formal Analysis, Software. Md. Abid Hossain Mollah: Conceptualization, Supervision. Kishwar Azad: Conceptualization, Supervision.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Integrated Health Science Research & Development Fund, Medical Education & Family Welfare Division, Ministry of Health & Family Welfare, Govt. of Bangladesh.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.