
Abstract
Objective:
To assess the nationwide prevalence and factors of unhealthy food consumption (UFC) among young children (6-23 months) in Somaliland.
Introduction:
Rising availability of unhealthy foods and poor healthcare access in Somaliland threatens infants and young children with serious health risks like overweight, obesity, and non-communicable diseases, requiring urgent nutritional attention.
Methods:
Cross-sectional analysis used 2020 SDHS data (n = 5263). UFC was defined by WHO IYCF indicators. Multivariable logistic regression reported AORs and 95% CIs.
Results:
UFC was associated with a unique nutrition transition. Highest wealth quintile children had greater odds (AOR = 3.87, P < .01). Conversely, Sool/Sanaag regions, 3 antenatal visits (AOR = 0.37, P < .01), and husband/partner not working (AOR = 0.85, P < .05) showed significantly lower UFC odds.
Conclusion:
This study provides critical evidence of wealth-driven UFC and protective regional/healthcare factors. Findings highlight the urgent need for targeted interventions leveraging antenatal care to improve child nutrition in Somaliland.
Introduction
Unhealthy dietary practices, particularly during infancy and early childhood, represent a significant global health issue, characterized by the excessive consumption of foods and beverages high in added sugars, salt, and unhealthy fats, while deficient in essential nutrients.1,2 Ultra-processed foods (UPFs), which are often energy-dense and nutrient-poor, further exacerbate this problem.3,4 The World Health Organization (WHO) defines complementary feeding as the introduction of additional foods and liquids alongside breastfeeding. 5 Unfortunately, the increasing availability, affordability, and aggressive marketing of unhealthy foods have led to their rising consumption, even in resource-constrained settings.5,6 Many infants and young children globally develop a preference for sugary drinks and salty snacks over nutrient-rich foods. 7 Studies indicate that 60% to 70% of children in certain regions regularly consume such unhealthy foods. These early dietary patterns can result in poor nutrition, impaired growth, and an increased risk of obesity, necessitating interventions.8 -10
The global shift toward unhealthy dietary patterns is particularly evident in low- and middle-income countries (LMICs), where processed foods are increasingly supplanting traditional diets.3,11 For example, a study conducted in Brazil documented an increase in the consumption of ultra-processed foods from 20% to 30% of total energy intake between 1987 and 2009.3,12 The consumption of unhealthy foods, especially in sub-Saharan Africa, poses a significant public health risk due to nutrient inadequacy, overweight/obesity, and chronic diseases stemming from early-life dietary habits. 13 In West Africa, 25% to 45% of children aged 6 to 59 months consume unhealthy processed foods, driven by factors such as affordability, convenience, and aggressive marketing strategies.12,14 In Somalia, challenges such as food insecurity, poverty, and conflict exacerbate difficulties in accessing nutritious food. 15 These interrelated factors create a precarious environment for vulnerable populations, particularly infants and young children. 16
Somalia faces enduring challenges, including conflict, displacement, and drought, which significantly impede efforts to ensure food security and adequate nutrition. 17 Somalia has a high rate of child malnutrition, with 30% of children under 5 stunted and 13% wasted, according to a 2020 report. 18 This trend poses a substantial threat to the health of Somali children. 19 Notably, there is a paucity of data regarding the consumption patterns of unhealthy foods among Somali infants and young children, this prevents the development of effective interventions, including targeted public health campaigns, feeding guidelines for carers, and rules governing the marketing of harmful foods to children. 20 The lack of comprehensive data on these consumption patterns obstructs the development of targeted interventions and policies. 21
This study addressed the issue of unhealthy food consumption among infants and young children in Somaliland by examining the prevalence of consumption of foods high in sugar, salt, and unhealthy fats. It aims to provide valuable insights for policymakers, program implementers, and researchers dedicated to enhancing child nutrition in Somalia. 13 The study contributes to the expanding body of evidence concerning the impact of unhealthy food consumption on child health in low- and middle-income countries (LMICs), thereby guiding evidence-based strategies to promote healthy eating habits. Significantly, this research will be the first to employ the most recent WHO Infant and Young Child Feeding (IYCF) indicators to assess unhealthy food consumption in Somalia, thereby informing targeted interventions and policies to address this escalating issue.
Material and Methods
Study Area
This study is conducted in Somaliland, a region situated north of the Equator, characterized by a semi-arid climate. The daily average temperatures range from 25°C to 35°C. Somaliland possesses a coastline extending 850 km and comprises 3 primary topographic zones: the coastal plain (Guban), the coastal range (Oogo), and the plateau (Hawd). The population is distributed across urban, rural, and nomadic settings. Administratively, the country is divided into 6 regions: Awdal, Waqooyi-Galbeed, Togdheer, Sool, Sanaag, and Sahil. Hargeisa serves as the capital city and the seat of government. These 6 regions further subdivided into 86 districts. 22
Study Design and Setting
This study utilized a quantitative, cross-sectional design through secondary data analysis to explore the factors associated with unhealthy food consumption (UFC) among infants and early toddlers aged 6 to 23 months in Somaliland. The research involved a cross-sectional analysis of a nationwide survey to assess the associations between various factors and unhealthy food consumption. This design facilitates the examination of relationships between variables at a single point in time. The study was conducted in Somaliland, with data collected from all regions of the country.
Study Population
The study population comprised all infants and early toddlers aged 6 to 23 months residing in households in Somaliland during the 2020 Somaliland Demographic and Health Survey (SDHS). Interviews were conducted with mothers or caregivers of the selected children to gather information on the children’s dietary intake and related factors. Inclusion criteria for the study were: (1) children aged 6 to 23 months at the time of the survey; (2) permanent residence in the households selected for the 2020 SDHS; and (3) having a mother or primary caregiver who consented and was available to complete the dietary intake interview. Records with incomplete or missing dietary data for the child were excluded from the final analysis.
Data Source (Sample size and Sampling procedure)
This study-utilized data from the SDHS 2020. A multi-stage cluster sampling technique was employed to obtain a nationally representative sample. Initially, Somaliland was divided into clusters based on administrative units, which are defined as enumeration areas (EAs) from the 2014 Population and Housing Census framework. Subsequently, households were randomly selected within each cluster. The final unweighted sample size comprised 5263 infants and early toddler children aged 6 to 23 months at the time of the survey. Sample weights were applied to adjust for the non-proportional allocation of the sample across different regions and to account for household and individual non-response, thereby ensuring the findings are nationally representative. Following data cleaning and extraction, 5263 observations were analyzed as illustrated in Figure 1.
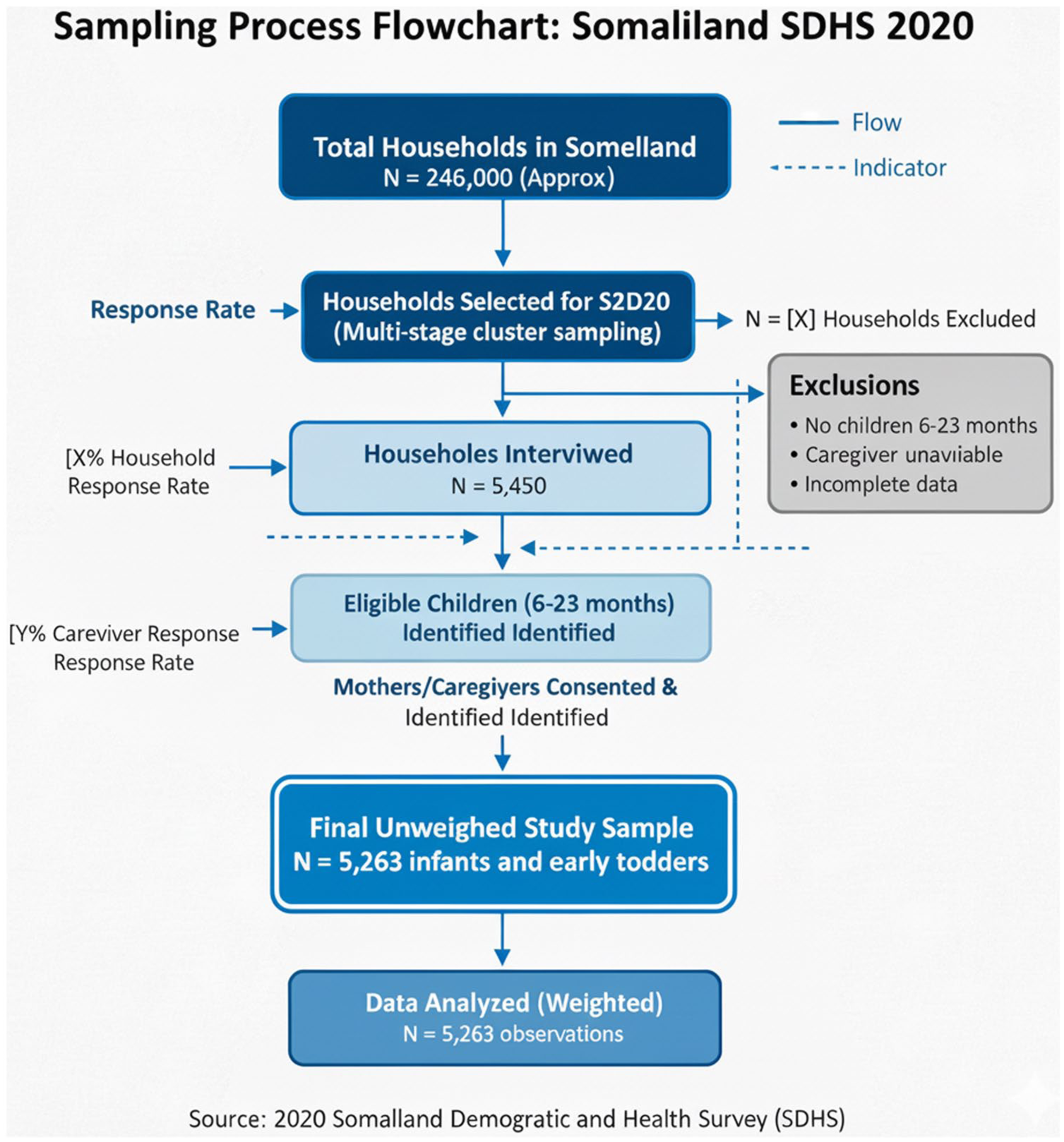
Flow chart of the sample selection procedure.
Operational Definition
Unhealthy food consumption (UFC) is characterized by the intake of at least one of the following food items within the 24 hours preceding the survey, as reported by the child’s mother or caregiver: sugary drinks (such as soda and juice with added sugar), processed snacks (including chips, candy, and cookies), instant noodles, and sweetened cereals.4,9,14,15 This definition is consistent with recommendations to limit foods high in added sugars, salt, and unhealthy fats in the diets of infants and young children.
Study Variables
Outcome Variable
Unhealthy food consumption (UFC) was the primary outcome variable, a binary measure (Yes/No) derived from 24-hour recall data. Mothers or caregivers reported all foods consumed by the child in the preceding 24 hours. UFC was defined as consumption of at least one of the following unhealthy foods: sugary drinks, soda, coffee or tea with sugar, candies, chocolate, cakes, sweet biscuits, ice cream, potato chips, and instant noodles. 7 Children consuming at least one of these items were classified as having “unhealthy food consumption”; otherwise, they were classified as having “healthy food consumption.”
Explanatory Variables
Drawing on the literature regarding child nutrition, dietary patterns, and socio-economic factors in similar settings,7,13 the selection of independent variables focused on socio-demographic characteristics, maternal and child health service utilization, and household factors. Specifically, the following explanatory variables were examined: Respondent’s current age (15-24, 25-30, 31-35, above 35); Region (Awdal, Waqooyi-Galbeed, Togdheer, Sool, Sanaag); Type of place of residence (Rural, Urban, Nomadic); Number of visits (1 visit, 2 visits, 3 visits); Highest educational level (No Education, Primary, Secondary, Higher); Age of household head (21 years or Less, 22-50, Above 51); Frequency of listening to radio (At least once a week, Less than once a week, Not at all); Frequency of watching television (At least once a week, Less than once a week, Not at all); Wealth quintile (Lowest, Second, Middle, Fourth, Highest); Husband/partner worked in the last 12 months (Yes, No); Sex of child (Male, Female); Age in months (Infancy, Toddlerhood, Preschool Age); and Place of delivery (Home delivery, Institutional delivery).
Statistical Analysis
Statistical analyses were conducted using Stata version 16.0. Descriptive statistics, including frequencies and percentages, were used to summarize sample characteristics and the prevalence of unhealthy food consumption. Bivariate analyses employed chi-square tests to assess associations between selected independent variables and unhealthy food consumption. Subsequently, multivariate logistic regression was used to identify independent predictors of unhealthy food consumption while controlling for potential confounders. Variables with P < .05 in bivariate analyses were included in the final multivariate logistic regression model, which was reported adjusted odds ratio (AORs) and crude odds ratio with 95% confidence intervals (CIs), with statistical significance set at P < .05. Before building the final model, multicollinearity among independent variables was checked using the variance inflation factor (VIF), where a VIF > 10 was considered indicative of significant collinearity; no variable exceeded this threshold. The model’s goodness-of-fit was assessed using the Hosmer-Lemeshow test, which showed a good fit for the model (P > .05) in Table 5.
Before building the final model, diagnostic checks confirmed its validity. The assessment for multicollinearity showed that the Variance Inflation Factor (VIF) values for all variables were low, ranging from 1.00 to 2.06 (mean VIF = 1.28), indicating that multicollinearity was not an issue. Furthermore, the model’s goodness-of-fit was confirmed using the Hosmer-Lemeshow test (χ2 = 13.35, df = 8, P = 0.1004), which demonstrated that the model was well-calibrated and adequately fitted the data.
Results
Magnitude of Unhealthy Food Consumption among Somaliland Children
The prevalence of unhealthy food consumption (UFC) among Somaliland children aged 6 to 23 months is presented in Figure 2. It shows that 39.41% of children aged 6 to 23 months consumed at least one unhealthy food item in the past 24 hours prior during SLDHS collection, while 60.59% did not consume any unhealthy foods. This indicates that unhealthy food consumption is relatively common, affecting about 2 in every 5 children in Somaliland.
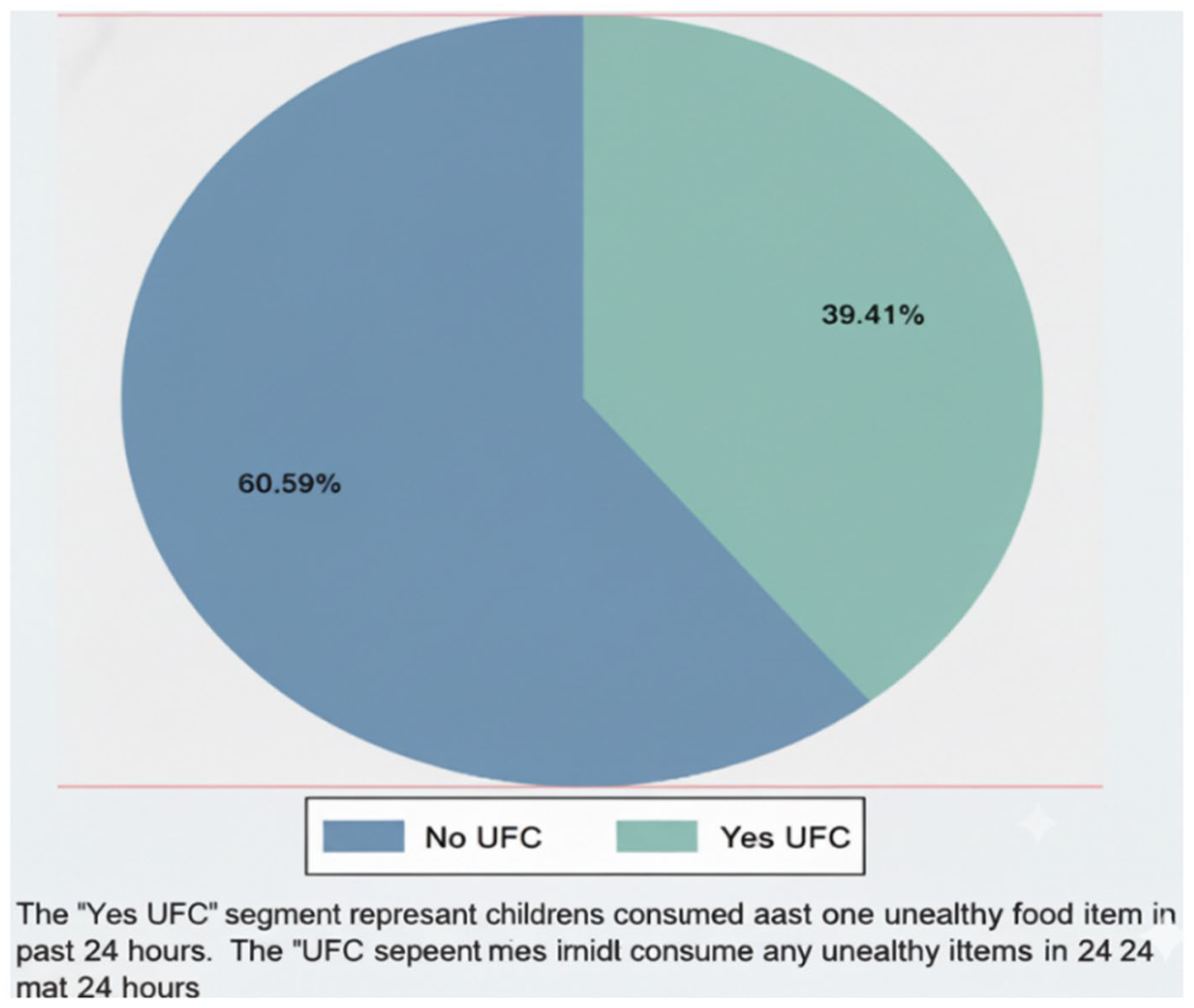
Prevalence of unhealthy food consumption (UFC) among children age 6 to 23 months in Somaliland (n = 5253).
The socio-demographic characteristics of the study population in relation to unhealthy food consumption (UFC) are detailed in Table 1. Bivariate analyses using chi-square tests revealed significant associations between UFC and several factors. Specifically, the region in which the child resided was significantly associated with UFC (χ2(4) = 19.84, P = .0005). The prevalence of UFC ranged from 37.43% (277 out of 740 children) in Awdal to 42.42% (448 out of 1056 children) in Waqooyi-Galbeed. Type of place of residence also showed a significant association with UFC (χ2(2) = 127.81, P < .0001), with higher UFC prevalence in rural (45.61%, 707 out of 1550 children) and urban areas (46.28%, 685 out of 1480 children) compared to nomadic areas (30.54%, 682 out of 2233 children).
Socio-Demographic Characteristics Associated Unhealthy Food Consumption among Somaliland Children Using 2020 SLDHS Data.

The highest educational level attained was significantly associated with UFC (χ2(3) = 75.11, P < .0001), showing a decreasing trend in UFC prevalence as education level increased, from 41.63% (1818 out of 4367 children) among those with no education to 8.16% (8 out of 98 children) among those with higher education. Similarly, age of the household head was significantly associated with UFC (χ2(2) = 93.87, P < .0001), with a UFC prevalence of 47.21% (508 out of 1076 children) in households where the head was 21 years or less, compared to 33.39% (948 out of 2839 children) where the head was above 51 years.
Frequency of listening to the radio (χ2(2) = 64.07, P < .0001) and frequency of watching television (χ2(2) = 132.83, P < .0001) were significantly associated with UFC, with lower prevalence among children who listened to the radio (25.49%, 117 out of 459 children) or watched television (22.70%, 175 out of 771 children) at least once a week, compared to those who did not listen to the radio (41.35%, 1924 out of 4653 children) or watch television (43.00%, 1864 out of 4335 children) at all. Wealth quintile was significantly associated with UFC (χ2(4) = 427.42, P < .0001), with the highest prevalence in the lowest quintile (58.48%, 776 out of 1327 children) and the lowest in the highest quintile (20.23%, 265 out of 1310 children). Whether the husband/partner worked in the last 12 months was also significantly associated with UFC (χ2(1) = 127.41, P < .0001), with higher UFC prevalence among children whose husband/partner did not work (47.40%, 1185 out of 2500 children) compared to those whose husband/partner did work (32.18%, 889 out of 2763 children).
Age in months (χ2 = 77.75, P < .0001) was significantly associated with UFC, where 50.85% (567 out of 1115) of infants consume unhealthy foods as compared to toddlerhood 36.66% (654 out of 1784) and preschool age (36.08%, 853 out of 2364). Lastly, place of delivery was significantly associated with UFC (χ2 = 122.89, P < .0001), with a higher UFC prevalence among children delivered at home (44.39%, 1617 out of 3643 children) compared to those delivered in a health facility (28.21%, 457 out of 1620 children). In contrast, the respondent’s current age (χ2(3) = 6.20, P = 0.1024), sex of the child (χ2(1) = 0.28, P = 0.5978), and number of visits (χ2(2) = 4.43, P = 0.1090) were not significantly associated with UFC.
This study utilized multivariable logistic regression to investigate the complex interplay between socio-demographic factors and unhealthy food consumption (UFC) among children in Somaliland, as shown in Table 2, providing a detailed understanding of this public health issue. The analysis revealed several significant associations, challenging some preconceived notions. Specifically, compared to children residing in the Awdal region, children in the Sool region (AOR = 0.766, 95% CI: −0.474, −0.06, P < .05) and the Sanaag region (AOR = 0.737, 95% CI: −0.487, −0.082, P < .01) exhibited significantly lower odds of consuming unhealthy foods. This suggests that regional cultural or environmental factors may play a protective role against UFC in these areas.
Multivariable Logistic Regression of Unhealthy Food Consumption Among Somaliland Children in Somaliland Using 2020 SLDHS DATA.

Abbreviations: Ref, reference category; COR, crude odds ratio, AOR, adjusted odds ratio; CI, confidence interval.
sig: ***P < .01. **P < .05. *P < .1.
Conversely, children living in nomadic communities (AOR = 1.238, 95% CI: 0.004, 0.424, P < .05) demonstrated a higher likelihood of UFC, potentially linked to limited access to diverse food options or different dietary norms. Furthermore, children from households within the highest wealth quintile (AOR = 3.865, 95% CI: 1.105, 1.598, P < .01) showed a significantly elevated risk of UFC, indicating that increased financial resources may paradoxically contribute to less healthy dietary choices, possibly due to the affordability and accessibility of processed and convenience foods.
However, several findings contradicted initial hypotheses. For example, mothers who attended 3 antenatal visits (AOR = 0.368, 95% CI: −1.676, −0.323, P < .01) were less likely to report UFC among their children, suggesting that increased engagement with healthcare services may promote healthier feeding practices, perhaps through nutrition counseling or education. Similarly, children whose husband/partner did not work (AOR = 0.854, 95% CI: −0.291, −0.025, P < .05) also showed lower odds of UFC, which is unexpected and suggests that factors beyond household income, such as time availability for home food preparation or different food purchasing priorities, may be at play.
In contrast, age of the household head (P > .05), frequency of watching television (P > 0.05), and the sex of the child (P > .05) demonstrated no statistically significant association with UFC, implying that these factors may not be primary drivers of unhealthy dietary habits in this population (Table 2)
Multicollinearity was assessed using the Variance Inflation Factor (VIF), and the results are presented in Table 3. As presented in Table 3, the VIF values for all variables included in the model ranged from 1.00 to 2.06, with a mean VIF of 1.28. These low values suggest that multicollinearity was not an issue and did not affect the stability of the regression coefficients.
Assessment of Multicollinearity.

Potential confounding variables were addressed using a standard statistical approach (Table 4). All variables that showed a statistically significant association with the outcome variable in the bivariate analysis (P < .05) were entered into the multivariable logistic regression model. This inclusion strategy allowed estimation of adjusted effects for each predictor while controlling for the influence of other significant factors, thereby ensuring the precision and validity of the adjusted odds ratios.
Control of Confounding Factors.

The goodness-of-fit of the final multivariable logistic regression model was assessed using the Hosmer-Lemeshow test, with the results shown in Table 5. The result showed that the model adequately fitted the data (χ2 = 13.35, df = 8, P = 0.1004), indicating no significant difference between the observed and predicted probabilities of unhealthy food consumption.
Assessment of Model Goodness-of-Fit. .

The non-significant Hosmer-Lemeshow test result (P > .05) suggests that the final multivariable logistic regression model has a satisfactory level of calibration, meaning the predicted probabilities closely align with the actual outcomes. This supports the reliability of the model estimates when interpreting the determinants of unhealthy food consumption among Somali children.
Discussion
The findings of this study, which reveal a high prevalence of unhealthy food consumption (UFC) among young children in Somaliland, have significant public health implications. Early-life dietary habits are foundational for long-term health, and high consumption of energy-dense, nutrient-poor foods is a major risk factor for childhood overweight and obesity, micronutrient deficiencies, and the later development of non-communicable diseases (NCDs) like type 2 diabetes and cardiovascular disease. These results signal an urgent need for preventative public health strategies to mitigate these future health risks.
Our finding that children in the Sool and Sanaag regions exhibited lower odds of UFC compared to those in the Awdal region aligns with the documented regional variations in dietary practices observed in other LMICs.12,21 This may reflect differences in cultural food preferences, agricultural practices, or the availability of local, healthier alternatives. Further qualitative research is needed to understand the specific factors driving these regional disparities. Conversely, the higher likelihood of UFC among children in nomadic communities’ echoes concerns about limited access to diverse food options and the potential reliance on readily available, processed foods in these settings, consistent with findings from other resource-constrained environments. 15
The unexpected association between higher wealth quintile and increased UFC warrants careful consideration. While previous studies have often linked lower socioeconomic status with poor dietary choices, 15 our results suggest that as household wealth increases in Somaliland, families may shift toward consuming more commercially available, processed foods high in sugar, salt, and unhealthy fats, similar to the nutrition transition described by Popkin et al. 11 This highlights the need for targeted nutrition education interventions aimed at informing wealthier households about healthy dietary choices for their children, even as their purchasing power increases.
The counterintuitive findings regarding antenatal visits and husband/partner employment status are particularly noteworthy. The lower odds of UFC among children whose mothers attended 3 antenatal visits suggests that increased engagement with healthcare services may be associated with improved maternal knowledge and practices related to infant and young child feeding, supporting the role of healthcare providers in promoting healthy dietary habits. 18 However, the observation that children whose husband/partner did not work had lower odds of UFC is puzzling and may reflect complex household dynamics. It is possible that in these households, mothers have more time for home food preparation and are less reliant on convenient, processed foods due to resource constraints, or that families are more likely to rely on food aid programs that promote healthier food. This finding contrasts with typical associations between unemployment and food insecurity 14 and calls for further investigation to disentangle the underlying mechanisms.
This study’s cross-sectional design limits our ability to establish causal relationships between the identified factors and UFC. Future longitudinal studies are needed to track dietary patterns over time and assess the impact of interventions aimed at promoting healthy eating habits. Furthermore, the reliance on maternal recall data may introduce reporting bias. Despite these limitations, this study provides a valuable baseline understanding of UFC and its associated factors among infants and young children in Somaliland. The findings underscore the need for multi-faceted interventions that address regional disparities, promote nutrition education, and create supportive environments for healthy eating, particularly in the context of rapid economic and social change. By identifying specific factors associated with UFC, this study contributes to the development of targeted strategies to improve child nutrition and reduce the long-term health consequences of unhealthy dietary habits in Somaliland and similar LMICs.
Novelty and Highlights of the Study
First Nationwide Assessment: This study provides the first nationwide assessment of unhealthy food consumption (UFC) among infants and young children (6-23 months) in Somaliland.
Application of WHO IYCF Indicators: It is among the first to apply the latest WHO IYCF (Infant and Young Child Feeding) indicators to specifically define and analyze unhealthy food consumption in the Somali context.
Unique Contextual Insights: The study identifies unique socio-demographic factors associated with UFC in Somaliland, including unexpected relationships with wealth quintile, antenatal care, and husband/partner employment, offering novel insights into dietary practices in a resource-constrained setting.
Informing Targeted Interventions: The findings provide crucial evidence for policymakers and program implementers to design targeted interventions and policies to address the growing burden of UFC and improve child nutrition in Somaliland.
Limitations and Future Work
The cross-sectional design limits causal inferences. Future longitudinal cohort studies are needed to track dietary patterns from infancy through childhood to establish causal links with health outcomes. Such studies would also enable the evaluation of specific public health interventions, such as the impact of sugar taxes, front-of-pack nutrition labeling, or community-based educational programs designed to promote healthier food choices. Reliance on maternal recall data may introduce bias. A primary limitation of this study is the use of a single 24-hour dietary recall, which may not accurately represent a child’s habitual diet due to day-to-day variation in food intake. This could lead to misclassification of children’s usual consumption patterns. Future research should aim to use multiple dietary recalls or food frequency questionnaires to capture a more stable estimate of dietary habits. Future longitudinal studies are needed to track dietary patterns over time and evaluate the impact of interventions. Reliance on maternal recall data may introduce bias. Future research should explore qualitative perspectives, investigate underlying mechanisms driving unexpected associations, and assess the effectiveness of culturally tailored interventions to reduce UFC and improve child health outcomes in Somaliland.
Policy Implications
This nationwide analysis of unhealthy food consumption (UFC) among infants and young children in Somaliland provides critical insights that necessitate targeted policy interventions. The significant associations identified between UFC and regional residence, wealth quintile, and maternal healthcare engagement demonstrate the limitations of a “one-size-fits-all” approach. Informed by systematic reviews highlighting the need for context-specific research in low- and middle-income countries, 21 the findings underscore the importance of nuanced strategies that address regional disparities, such as learning from protective factors in Sool and Sanaag, and mitigating the potential for increased wealth to drive consumption of processed foods. Successfully addressing UFC requires that policies acknowledge its multifaceted nature, leveraging cultural insights alongside economic realities to craft impactful and tailored solutions.
Specifically, this study suggests policymakers should: (1) Prioritize targeted nutrition education to high-income families emphasizing the importance of fresh, locally sourced foods over processed options; (2) Strengthen antenatal and postnatal care programs to include effective counseling on optimal infant and young child feeding practices, while focusing on high-risk groups like nomadic communities; and (3) Promote nutrition-related campaigns that improve access and availability of health foods as 1 approach that is more likely to shift the current trends. Moreover, future research is crucial to explore the drivers of these trends and evaluate the effectiveness of culturally tailored interventions to reduce UFC and improve long-term child health outcomes in Somaliland, contributing to a more robust evidence base for policy development in similar resource-constrained settings.
Conclusion
This study provides critical insights into unhealthy food consumption (UFC) among infants and young children in Somaliland, revealing significant associations with socio-demographic factors such as region, wealth quintile, and maternal healthcare engagement. The findings underscore the need for targeted, context-specific interventions to promote healthy dietary habits, addressing regional disparities and leveraging healthcare platforms to improve child nutrition in the face of a changing food environment.
Footnotes
Acknowledgements
The authors express their sincere gratitude to the Somalia National Bureau of Statistics for granting access to the 2020 SLDHS data. We also acknowledge measure DHS for their technical support in the data collection and dissemination process. We extend our appreciation to the mothers and caregivers who participated in the survey, providing valuable information for this research. Finally, we would like to acknowledge the contributions of Amoud University’s Research and Innovation Center for their support in performing this study and the assistance offered to us.
Abbreviations
Ethics Approval
This study utilized secondary data from the 2020 Somaliland Demographic and Health Survey (SDHS). The original survey protocol was reviewed and approved by the Institutional Review Board of the Somaliland National Bureau of Statistics. As the present study involved the analysis of a publicly available, anonymized dataset, no additional ethical approval was required. Formal permission to access and use the data was obtained from the Somalia National Bureau of Statistics.
Consent to Participate
During the primary data collection, written informed consent was obtained from all participating mothers or their legally authorized caregivers.
Consent for Publication
This manuscript represents an original cross-sectional analysis of unhealthy food consumption and associated factors among infants and early toddler children in Somaliland, utilizing a nationwide perspective derived from the 2020 SLDHS data. The findings presented have not been previously published, nor are they under consideration for publication elsewhere.
Author Contributions
Conceptualization: HGD, MMO, AMY, MAH, and AMO; Methodology: HGD, MMO, AMY, MAH, AMO, and AHM; Data curation: HGD, AMY, and AHM; Analysis: HGD, AMY, and AHM; Visualization: MMO, MAH, and AMO; Writing—original draft preparation: HGD, MMO, AMY, MAH, AMO, and AHM; Writing—intellectual content, review, and editing: HGD, AMY; MMO, and MAH; Supervision: AHM; All authors reviewed and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this study are available upon request from the Somalia National Bureau of Statistics. Access requires registration and adherence to the data use policies established by the Somalia National Bureau of Statistics.