
Abstract
Background:
Spina bifida (SB) is a congenital disorder often leading to disability and limited social participation. Children with SB face challenges engaging at home, school, and in the community. This review examined the types and degrees of social functioning in children with SB.
Methods:
Researchers searched 5 databases (CINAHL, MEDLINE, PubMed, EMBASE, and PsycINFO) for studies of various designs, both qualitative and quantitative, published between 2000 and 2025 that involved children with spina bifida (SB) aged 18 years or younger.
Results:
Findings revealed restricted participation with peers and family due to continence issues, motor impairments, stigma, and cognitive difficulties. Four domains of social functioning emerged: school and community participation, peer relationships and freindships, family interactions and parental role, and independence and autonomy.
Conclusions:
Children with SB demonstrate reduced social functioning. More research is needed to clarify the impact of parental expectations on social outcomes.
Keywords
Introduction
Spina bifida (SB) is the second most common birth defect globally, behind congenital heart abnormalities. 1 It is a congenital neural tube defect characterized by incompletely closed spinal column due to incomplete closure of the neural tube. 2 The severity of SB and the intensity of the associated physical challenges are determined by the size and location of the opening in the spine and the damage to the underlying nerves. A range of physical symptoms, including loss of mobility, incontinence, and hydrocephalus, can be observed in children with SB. 3 Physical impairment invariably affects other dimensions of the lives of children with SB, such as their psychological, social, and intellectual capacity. The challenges that children with SB face have long-term implications. 4 Social functioning in children with spina bifida refers to their capacity to form and maintain age-appropriate peer relationships and engage adaptively in social environments, an ability shaped by underlying social cognitive skills (eg, joint attention and perspective-taking), executive functions (eg, attention and planning), and behavioral autonomy. 5 However, these children often face challenges: they may display social immaturity and passivity, have fewer interactions outside school, rely more on adult support, and struggle with the neurocognitive processes needed to adjust socially. The consequences are particularly devastating for families of children with SB and, subsequently, for communities. Longitudinal, multimethod evidence by Holbein et al indicates that neuropsychological factors, particularly attention and executive function, are the strongest predictors of later social skills in youth with spina bifida, often explaining more variance than family or health measures. 5 Moreover, SB poses a substantial burden on healthcare systems. Regarding healthcare expenses, a 2013 study of a nationwide inpatient sample including all ages in the United States revealed that hospital stays linked to birth abnormalities of the brain and spine, including SB, cost more than $1.6 billion. 6 Grosse et al estimated that a person with SB in the United States will pay $791 900 for lifetime care, comprising $513 500 in medical costs, $63 500 in developmental services and special education costs, and $214 900 in caregiver time costs. 7
Children and teenagers with chronic illnesses often have decreased social functioning compared to those without chronic illnesses. 8 Many chronic diseases restrict the type and degree of physical exercise, social interaction, and school attendance; therefore, this restriction may be caused by many elements. These limitations may be attributable to physical restrictions, prolonged or repeated hospitalizations, frequent doctor’s appointments, or special transportation requirements. Low levels of community and preschool/school engagement were observed among children with spina bifida. Low levels of participation, dependency in day-to-day living, and delayed social development are frequently noted effects of spina bifida. Due to advances in neuropsychological research, we now know more about the cognitive consequences of spina bifida on language, perception, attention, memory, and executive functioning than we did 30 years ago. 9
Many children and adolescents with SB have poor social adjustment throughout development stages. 10 Previous research has focused on the limitations and challenges children with SB face when engaging in social functioning. For example, continence issues (ability to control bowel and bladder movements) were a major limitation for most participants in the studies by Fischer et al 12 and Kelly et al. 23 Incontinence problems in children with SB range from minimal to significant, depending on the level of the lesion. Because they were ashamed and felt compelled to conceal it from their peers, children with SB saw their incontinence as a serious problem in addition to the physical pain they experienced. Recent research indicates that 87% of people with spina bifida have bowel incontinence, and fewer than 30% have bowel continence. Urinary continence problems afflict 48% to 76% of children with the condition. 11 It can significantly hinder their social lives, limiting their participation in activities, reducing their peer relationships, and negatively impacting their self-esteem. 12 Similarly, children with spina bifida experience a decline in their quality of life and health-related quality of life as the severity of their bowel incontinence symptoms increases.
Much of the literature has focused on medical perspectives, while children’s own voices remain underrepresented. Yet, children’s perspectives are crucial for understanding how they interpret stigma, negotiate autonomy, and construct their identities. For instance, a qualitative study of Palestinian children with SB revealed experiences of vulnerability, dependency, and exclusion, but also highlighted resilience fostered through family and religious support. Such findings underscore that social functioning is deeply shaped by cultural, economic, and political contexts. 13 Children in high-income countries may benefit from inclusive education and rehabilitation programs, whereas those in low-resource or conflict-affected settings face compounded barriers of poverty, stigma, and limited services. Palestinian children with SB have reported vulnerability and exclusion, but also resilience through family and community support. 14
This review aimed to assess the types and degrees of social functioning in children with spina bifida. Through clarifying the strengths and gaps in the existing literature, the review underscores key opportunities to enhance both research efforts and the psychosocial and developmental services provided to these children.
Methods
Data Sources
Whittemore and Knafl’s framework provided the basic conceptual structure for this integrative review. 15 The 5 stages: 1. problem identification, 2. literature search, 3. data evaluation, 4. data analysis, and 5. Presentation. These were rigorously followed to ensure methodological transparency and trustworthiness.
During problem identification, the research question was refined to examine the dimensions of social functioning in children with spina bifida (SB). In the literature search stage, comprehensive searches were conducted across 5 major databases (CINAHL, MEDLINE, PubMed, EMBASE, and PsycINFO) using controlled vocabulary and Boolean operators to maximize inclusiveness. The data evaluation stage employed Olsen and Baisch’s 19 quality appraisal tool to assess methodological quality. The critical appraisal was conducted independently by 2 researchers (EA [Reviewer 1] and SA [Reviewer 2]). Any disagreements were resolved through discussion and consensus. For data analysis, a constant comparative technique was applied to identify patterns and themes across studies, integrating both qualitative and quantitative findings to develop synthesized domains. Finally, the presentation stage followed PRISMA guidelines to ensure clear reporting of the search and selection process.
To enhance rigor and confirmability, several strategies were employed. Transparent reporting was maintained through detailed documentation of database searches, inclusion/exclusion criteria, and quality assessment procedures. Reflexivity was observed by acknowledging potential author biases during data extraction and synthesis, with regular discussions to ensure that interpretations were grounded in evidence rather than assumptions. Triangulation of data sources including qualitative, quantitative, and mixed-method studies strengthened the comprehensiveness and depth of interpretation. In addition, peer debriefing among team members was conducted throughout the synthesis process to verify emerging themes and interpretations. These steps collectively enhanced the credibility, dependability, and confirmability of the review findings.
This allowed more diverse articles in the literature to be included than a systematic review would have permitted. The databases searched for relevant articles included CINAHL, MEDLINE, PubMed, the Excerpta Medica Database (EMBASE), and PsycINFO. The information is summarized in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram (Figure 1). 16 The terms used were spina bifida, family functioning, social participation, social adjustment, and social functioning. Since this study is a review paper and did not involve the collection of new data from human participants or animals, Institutional Review Board (IRB) approval and informed consent were not required.
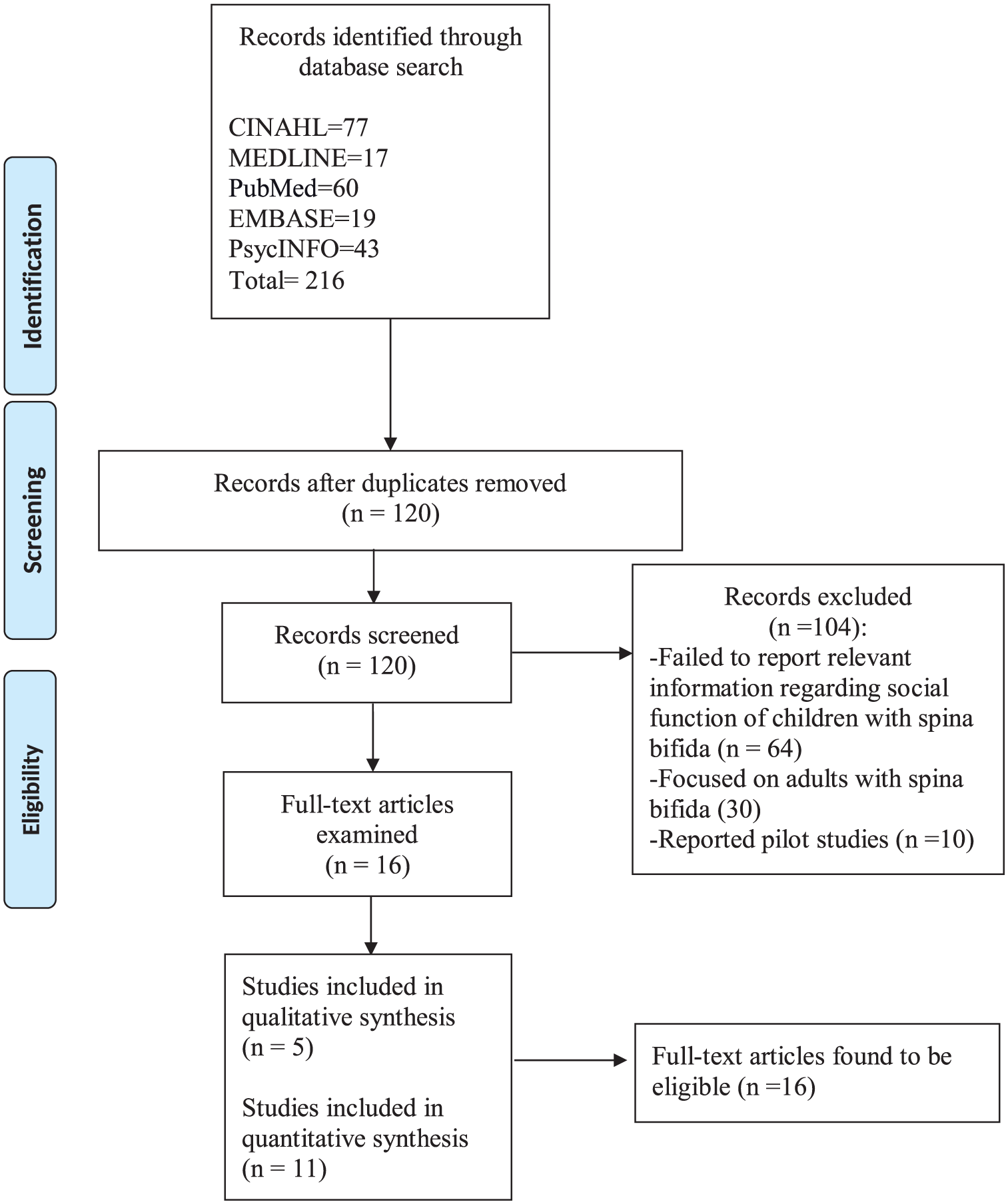
PRISMA diagram.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (1) research involving children with SB aged ≤ 18 years and/or their parents; (2) published in English between 2000 and 2025; and (3) addressed the participation of children with SB in social functioning at home, at school, with family, or with friends. Children with spinal cord injury (SCI) and typically developing peers were included in this review and compared with children with spina bifida. Studies were excluded if they failed to report relevant information on the social functioning of children with SB or if they focused exclusively on adults with SB. We focused on children with SB aged ≤ 18 years because the foundations for social functioning are generally developed during childhood, and adolescents tend to struggle with their social skills as they transition into adulthood. 17 Social functioning is particularly important for the development of social skills in children with SB. We limited the review of studies to between 2000 and 2025 to focus on more recent findings regarding children’s social functioning and skills.
Study Selection
In consideration of the PRISMA (2021) guidelines, the initial screening of titles and abstracts identified 216 potentially useful articles. Of these, 96 were duplicates and 104 did not meet the inclusion criteria, resulting in the exclusion of 200 articles. Sixteen articles that met the inclusion criteria were reviewed, and their data were analyzed and synthesized. Figure 1 summarizes the article selection process. 17
Study Synthesis
A literature review matrix (Table 1) was developed and used to organize and analyze the information from 16 articles. 18 Relevant data were extracted from each study, organized in ascending chronological order, and synthesized using a review matrix.
Literature Review Matrix of Selected Studies.

Quality Appraisal
To establish methodological quality, each selected study was evaluated using the quality appraisal tool developed by Olsen and Baisch. 19 This tool includes 4 components: study type, sampling method, data collection method, and analysis type. The scores assigned to the study types ranged from 1 (best practice report) to 6 (quantitative experimental design). The sampling method scores were assigned as follows: 0 = not explained or NA, 1 = convenience, 2 = purposive or case-matching, and 3 = random or 100%. For the data collection method, a score of 1 or 0 was assigned depending on whether the data collection methods and tools were explained (1) or not (0). Finally, based on the highest reported level of analysis, the analysis type was scored as follows: 1 = narrative, 2 = descriptive statistics, and 3 = inferential statistics. Consequently, the total tool scores ranged from 2 to 13; the higher the total score, the better the quality of the study. 19 Quality appraisal scores are listed in Table 1.
Results
Study Sample Characteristics
Table 1 provides a detailed summary of the studies included in this review. Five qualitative and 11 quantitative studies accounted for 31% and 69% of the studies, respectively. A total of 1489 children with SB were included in this study from various different studies. Notably, it’s important to mention that some studies of children with SB also included children without SB, specifically those with SCI, and typically developing peers. A total of 510 parents participated in these studies. The sample size range of children with SB was 20 to 140, while that of the parents was 20 to 90. Child/adolescent participants ranged from 2 to 18 years of age; however, a few studies reported adult participants up to 23 years of age.
As shown in Table 1, the studies had both quantitative and qualitative research designs. Among the quantitative studies, cross-sectional, prospective, longitudinal, and experimental designs were employed. Eleven studies were quantitative in nature, while the remaining 5 were qualitative, employing phenomenological, grounded theory, descriptive, and cross-sectional designs. A wide variety of instruments have been used to measure social participation, such as the Children’s Assessment of Participation and Enjoyment (CAPE), Activities Competence Scale of the Child Behavior Checklist (CBCL), School Function Assessment (SFA), and Participation and Environment Scale for Children and Youth (PEM-CY). In addition, open-ended questions about participation, the influences of participation, and barriers to participation in social activities were used during the interviews in the qualitative studies.
Examples of instruments used to measure peer relationships include the General Friendship Interview, Didactic Friendship Interview, Friendship Quality Scale, and open-ended questions in qualitative studies about interactions with friends.
Study Quality
Study quality was assessed by calculating the appraisal scores using the Olsen and Baisch’s quality appraisal tool. 19 Each study score was calculated with 13 as the maximum score and 2 as the minimum score. The overall quality appraisal scores (Table 1) for all studies ranged from 7 to 9.
Thematic Results
Guided by models of social participation in youth with chronic health conditions by Pinquart and Teubert, 8 the synthesis was organized into the following domains: (1) School and Community Participation, (2) Peer Relationships and Friendships, (3) Family Interactions and Parental Role, and (4) Independence and Autonomy. This integrative review revealed several key findings: Researchers have indicated that children with SB often show limited participation in school, community, and physical activities. Overall, this review shows that children with SB face various challenges in social functioning. Parents and friends significantly influenced the lives of individuals with SB regarding the social functioning of children with SB played a pivotal role in shaping their developmental trajectory. The synthesis identified 4 domains: (1) School and Community Participation, (2) Peer Relationships and Friendships, (3) Family Interactions and Parental Role, and (4) Independence and Autonomy. The domains that emerged from the integrative synthesis are presented below:
School and Community Participation
Engaging in school, community, and physical activities can be difficult for children with spina bifida (SB). However, parents felt that participating in outdoor sports could improve their children’s social and academic abilities, as well as their general health and well-being. 20
Various factors contributing to restricted social participation among children with SB were identified in this review, including mobility, incontinence, and intellectual challenges among others. Children with SB who use wheelchairs tend to have more limitations in social functioning due to difficulties with building accessibility and long-distance transportation. Fischer et al 12 revealed that children with SB who achieved bladder continence were more independent and participated in more social functioning than children who experienced incontinence. Similarly, compared to their younger peers, older children with spina bifida (SB) engage in fewer leisure, physical, and skill-based activities. Child’s gender and level of schooling had no impact on participation. However, youth with employed caregivers participated in more social activities. Child motor level, ambulation, and bladder/bowel issues showed no significant impact on participation, except for youth without a shunt, who participated more in physically demanding and skill-based activities. The study also highlighted a link between increased pain and reduced social competence, with greater pain intensity decreasing social activity. The association between social competence and pain decreased with increasing engagement in social activities. Additionally, decreased social activity has a significant negative effect on social competence.12,21 -23 Another study showed that various factors affect active community engagement. Among these factors are low motivation, lack of information, time constraints, and insufficient family support. 24 Similarly, Papadakis et al 41 found that in youth with SB, sociodemographic factors, including race, ethnicity, health insurance status, education level, and employment status, significantly and negatively affected academic performance and social functionality in some individuals with SB.
Family Interactions and Parental Role
Holbein et al 25 reported that parents of children with Spina Bifida (SB) aged 10 to 11 held high expectations for their children to achieve 5 life milestones: independent living, college attendance, full-time employment, marriage, and parenthood. However, when their children reached ages 16 to 17, these expectations significantly decreased compared to their counterparts with typical development. Optimism, sociodemographic factors, and the child’s larger environment are some of the factors that shape the nature and impact of parental expectations. 25
Researchers have found that parents are the most important source of support for children with SB to participate in social activities. In addition, parents provide a great deal of care by imparting health-related information and providing support for their children’s emotional well-being and sense of self to ensure their quality of life.24,26
Despite parents’ strong level of support, researchers have reported that most parents believe that their children with SB differ in aspects of their social participation from children without ailments, including siblings. In one qualitative study addressing parents’ perceptions of how their children with physical disabilities were influenced by outdoor sporting activities, thematic categories emerged from interviews: achieving good health, being part of a social group, and learning a sporting activity. These categories reflect the importance parents place on sports activities for children and adolescents with physical disabilities. 20 Moreover, parents lowered their expectations of their children with SB for academic and social performance over time because of their condition; however, optimistic parents showed increased expectations. 20
Peer Relationships and Friendships
While this is not always the case, children and adolescents with SB are more likely to name a healthy peer as their best friend. 27 Kids and teens with SB might benefit from peer support, although such assistance is often lacking. Peny-Dahlstand et al reported that although most children with SB try to explain their condition to their friends, they rarely discuss the difficulties surrounding bowel and bladder issues, which are the challenges that most interfere with their social participation. 21 In addition, peer acceptance of friends with SB varied considerably among studies, with some children reporting many close friends and others reporting that they had no friends.12,27 In a study by Stiles-Shields et al, many self-reported friendship qualities did not differ markedly from peers, which mirrors Stiles-Shields et al’s longitudinal findings that friendship trajectories for many quality domains are similar for youth with SB and their chosen peers, supporting a strengths-based interpretation. 28 Furthermore, Peny-Dahlstrand et al 21 found that 89% of individuals with SB had low levels of interest in participating in and being involved in school activities, especially structured activities in recess and playground settings. Youth with SB spend fewer days with friends and show lower levels of security, companionship, and emotional support from friends and family. 27 Furthermore, Suhs et al 29 examined 140 children and adolescents with spina bifida (mean age 11.4 years; 53.6% female) and their closest friends to show that observed peer-interaction quality, characterized by positive affect, responsiveness, and mutual engagement during a structured task, was significantly associated with both less withdrawn or depressed behaviors and better physical health adjustment. While self-reported emotional support was associated with enhanced emotional quality of life but not with physical health outcomes, friendship quantity, that is, the number of friends, was linked only with fewer withdrawn/depressed behaviors and did not predict physical health outcomes. 29
Independence and Autonomy
In addition, for children with SB, learning and intellectual disabilities can increase their risk of not participating in social functions. 30 Bakaniene and Prasauskiene 26 and Bloemen et al 31 focused on the influence of environmental variables as they investigated the patterns and determinants of social involvement in Lithuanian children and adolescents with SB and found that social participation is mainly affected by the home and school settings where they can be encouraged to participate or negatively influenced by the contrary. Furthermore, the social participation of children with spina bifida is shaped by a confluence of elements, encompassing their physical capacities, functional capabilities, and the extent of support provided by their environment. 30 These findings were further supported by Flanagan et al, who found that children with SB engaged in fewer activities than those with paraplegic SCI. 32
Social functioning in young adults with SB can be affected by their inability to reach normal developmental milestones. Holbein et al observed that emerging adults with SB exhibited a lower likelihood of attaining milestones such as attending college, securing full-time employment, living independently, getting married, and becoming parents than individuals with typical development. 25 Furthermore, even though children with SB were less likely to get a driver’s license, work in a competitive job, or hang out with friends, according to Liptak et al, 76% had competitive jobs or were enrolled in school, 30% had a driver’s license or learner’s permit, and 15% went on dates and spent time with friends. 30 Murray et al 33 caution that improving social functioning may also increase exposure to risky behaviors (eg, alcohol, sexual activity), so interventions should combine social-skill enhancement with risk-prevention education. 33 According to the findings of Darow et al, 34 the levels of Cognitive Disengagement Syndrome (CDS) that were judged by teachers at the beginning of the study were substantially higher in pupils with SB compared to their classmates with Typically developing (TD) (intercepts: SB = 1.60 vs TD = 1.02). However, the intercepts rated by mothers did not vary significantly (SB = 1.03; TD = 1.05). According to growth curve analysis, the CDS was constant throughout the 5 evaluations. More importantly, in the SB group, higher baseline teacher-reported CDS predicted lower father-rated (b = −0.53) and teacher-rated social skills (b = −0.80), and larger increases in teacher-reported CDS over time further predicted eventual social skill deficits (b = −0.54). Moreover, among SB kids, increases in mother-reported CDS specifically predicted worse behavioral autonomy (b = −0.43). These longitudinal correlations highlight how much social functioning and decision-making autonomy in children with spina bifida are undermined by both the degree and trajectory of attentional disengagement. 34
Children with Spina Bifida exhibit incredible resilience and a tremendous desire to participate in their communities despite the challenges they encounter. 30
Discussion
Our research provides important new information on the social functioning of children with SB. First, when comparing children and adolescents with SB to those with other chronic diseases, researchers have consistently shown poorer social functioning in patients with SB. However, the degree of impairment varied across the reviewed studies, underscoring important similarities and differences. Similarities across studies included the repeated identification of incontinence, hydrocephalus, mobility challenges, and cognitive delays as primary barriers to social participation. Regardless of geographic or cultural context, continence problems were strongly associated with isolation, reduced self-esteem, and withdrawal from peer activities. Similarly, motor impairments and executive dysfunctions were recurrently linked to limited participation in physical and school activities. Differences among studies largely reflected contextual and methodological variations. For instance, studies from high-income countries frequently emphasized environmental modifications, inclusive education, and structured rehabilitation programs as protective factors, while research from low- and middle-income settings highlighted the amplifying effects of poverty, stigma, and inadequate healthcare services. Qualitative studies, especially those incorporating children’s voices, described nuanced experiences of shame, resilience, and identity formation that were less visible in quantitative surveys. By contrast, quantitative studies often relied on standardized instruments (eg, PedsQL, SOC scales), which facilitated cross-country comparisons but may not fully capture cultural or contextual differences in lived experiences. Another divergence lay in the treatment of parental expectations. Some studies reported that parents of children with SB lowered milestone expectations over time, whereas others highlighted the risks of overprotective attitudes that restricted independence.
This highlights the unique social issues encountered by people with SB.
We investigated how parental expectations affect the social engagement of children with SB. It is important to recognize the complex interactions between parental expectations and the social functioning of children with SB, 35 even though the specific findings pertaining to these expectations were not clear in the summaries provided. A more thorough analysis of how parental expectations either exacerbate or lessen barriers to social participation for children with SB may be beneficial for future studies and interventions. 36
The identified lower social functionality in children and adolescents with SB compared to those with other chronic conditions underscores a significant challenge in their interactions with friends and family members. 30 This limitation appears to be mainly related to the lack of facilities that meet the requirements of children with chronic illnesses, such as SB, and parents’ ignorance of the existence of these facilities. 37 This highlights a crucial gap in the systems of support for children with SB, which impedes their ability to interact socially and might even make them feel alone. To address this complex issue, comprehensive initiatives are required to improve infrastructure and public knowledge of the resources available for children with SB and their families.
This review demonstrated that several factors significantly limit the social participation of children with SB. Incontinence issues lead to isolation, and motor level restrictions hinder engagement in activities such as running or jumping.5,12 Cognitive delays associated with hydrocephalus pose additional challenges. 9 Parental employment and income levels can affect access to social opportunities. Despite mothers being the primary source of support, there has been limited exploration of how parental expectations influence the social functioning of children with SB. The impact of incontinence on children’s social participation was evident, leading to isolation and restriction of engagement with others. Incontinence is considered a major health issue for children, as some tend to hide it from their families and friends. It is crucial to understand the factors that affect children with SB to participate in social development, which could help children who need intervention. Motor level restricts children’s ability to engage in activities, specifically those that require running or jumping skills. Children with hydrocephalus tend to experience cognitive delays that affect their participation in sports. Parents’ employment was related to social participation because income may provide more opportunities for children to engage in private centers or extended networks. Furthermore, although some investigators reported that mothers served as the primary source of support for children with SB, a notable gap identified in this review is the absence of studies explicitly connecting parental expectations to social functioning in SB, despite robust evidence for such links in academic and developmental contexts. This absence is itself important: it highlights a critical area for future inquiry and suggests that parental expectations, while well-established as predictors in other pediatric domains, remain underexplored in SB. Based on the literature, children born with disabilities are viewed as vulnerable by their parents, especially when compared to their healthy peers or siblings. This viewpoint may lead to overprotective behavior on the part of parents, which can, in turn, result in less functioning in a child. According to Holmbeck et al, 38 parents of children with SB showed greater overprotective behavior than parents of children without the condition, and children of overprotective parents may have less autonomy, less social maturity, and a limited ability to interact with other children. 38 It is often not emphasized or researched in detail which parent views the child with SB more vulnerable that is, father or mother. Kritikos et al examined informant discrepancies between mother and father reports of child vulnerability in 92 families of youth with spina bifida. They found that fathers were more likely than mothers to rate their child as highly vulnerable, and that these “father-high/mother-low” discrepancies were significantly associated with greater paternal mental-health symptoms, higher parenting stress, poorer parenting alliance, and more child behavior problems. The authors conclude that such father–mother perceptual gaps may serve as a “red flag” for clinicians, signaling the need to assess parental adjustment and family functioning. 39 According to Holbein et al, parents of children with spina bifida decreased their expectations for the majority of milestones with time; these expectations were positive and had nothing to do with the actual attainment of milestones. Compared to those with regular development, emerging adults with spina bifida had a lower chance of reaching every milestone. While it’s crucial for families to establish reasonable objectives, children with spina bifida and their families may benefit from optimistic parental expectations. 25
The effects of spina bifida on several bodily systems, such as the neurological, musculoskeletal, genitourinary, and gastrointestinal systems, as well as the influence on a child’s psychosocial development, need multidisciplinary treatment. Therefore, the findings of this review underscore the importance of interdisciplinary care in developing interventions to maximize the social functioning of adolescents with SB, regardless of their physical limitations. Future intervention research of interdisciplinary teams that assist parents with their ability to help their children with spina bifida engage in social functioning and become more socially involved with family and friends is needed. Furthermore, social activities such as sleepovers, camp overnights, dating, and social and recreational activities outside the home should be encouraged. This could help in development and maintenance of friendships. 40 Such research could reveal avenues for parents and other caregivers to empower children and adolescents with SB, helping them better understand and accept their bodies and take pride in their identity, rather than viewing themselves as broken or shameful. 12 In addition, the limited body of research on the association between incontinence and social participation should be expanded, and nurses should familiarize themselves with such research so that they can help children with SB to avoid social isolation. Healthcare providers, including nurses, can assist families in choosing to learn clean intermittent catheterization, which can reduce incontinence and influence social participation.
Future Implications
This review highlights the need for multidisciplinary interventions that go beyond physical rehabilitation to include cognitive, psychosocial, and educational supports for children with spina bifida. A key gap is the limited evidence on parental expectations, which future studies should explore through longitudinal and intervention-based designs to determine how realistic yet optimistic outlooks influence social outcomes. Rigorous, prospective SB studies using multi-informant measures and standardized social outcomes are needed to clarify whether and how expectations shape social functioning. Greater attention to environmental supports such as accessible infrastructure, inclusive school policies, and stigma reduction is also critical. Finally, programs that prepare families and youth for the transition to adolescence and adulthood, combining social-skill building with risk-prevention strategies, may help maximize participation and independence.
Limitations
Despite the multiple insights reported, this review has limitations. First, the review focused only on studies published in English; therefore, relevant studies published in other languages may have been omitted. Second, the quality appraisal performed for this review found that the quality scores were lower for 9 studies because they did not fully address their sampling and data collection methods; this limitation reduced the significance of their findings and conclusions. In contrast, the 7 studies that detailed their research methods received overall quality appraisal scores of 8 and 9, suggesting that their findings can be considered more reliable and meaningful.
Conclusion
This review identified 4 domains which are engagement in social activities, parents’ expectations or roles, and peer relationships, and found consistent participation limitations among children with spina bifida. Major drivers were continence and mobility problems, hydrocephalus and neuropsychological deficits (eg, attention/executive dysfunction), and contextual barriers (stigma, limited school/community supports). We recommend interdisciplinary care that pairs medical/rehabilitation management with routine cognitive screening, psychosocial support, and school accommodations, and that includes risk-prevention education. While this review confirms consistent limitations in social functioning among children with SB, it also reveals a striking gap: the lack of studies examining the influence of parental expectations on social outcomes. Given the established role of expectations in shaping academic achievement and self-management in chronic conditions, this omission should be a priority for future research. Recognizing and addressing this gap can help families and healthcare providers develop interventions that better support children’s social integration. Thus, future nursing research should focus on addressing this gap, with the goal of maximizing the social functioning of children and adolescents with SB.
Footnotes
Ethical Considerations
As this was an integrative review, no permission was required.
Author Contributions
Dr. Ranya Bafail: Conceptualization, Methodology, Investigation, Data Curation, Formal Analysis, Writing—Original Draft, Writing—Review & Editing, Visualization, Project Administration.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data was acquired from public sources.