
Abstract
Intraosseous (IO) access is vital for pediatric resuscitation when intravenous access is challenging. This study aimed at developing and evaluating a simulation-based procedural training curriculum for pediatric residents to improve IO access knowledge and skills. Residents across different training years participated in an online didactic module coupled with a hands-on simulation session practicing the use of IO drills. Skills and knowledge were assessed at baseline and post-intervention at an average of 4.8 months. Of the 68 participants, 72% completed both assessments, and results showed a significant improvement in skills (median score increased from 0 to 5, P < .001) and knowledge (median score increased from 19 to 25, P < .001) at post-intervention. These findings support the integration of simulation-based curricula into residency programs to enhance procedural competency and skill retention. Further research is needed to assess translation of learned skills into clinical practice.
Keywords
Introduction
In critically ill children, establishing vascular access is a crucial step in resuscitation to administer fluids, antimicrobial therapy, and cardiovascular support, as well as obtain diagnostic tests. While intravenous (IV) access is typically the standard modality for this, obtaining IV access can often be difficult in pediatric patients due to smaller veins, anxiety about procedure, changes in vascular tone, and higher thickness of subcutaneous adipose tissue. 1 An alternate modality of vascular access, known as intraosseous (IO) access was first described in the 1920s in the adult population as a safe, reliable, and quick technique, and by the 1940s, research demonstrated its safety in the pediatric population. 2 IO access placement refers to the procedure of inserting a hollow bore needle directly into the medullary space within bone cortex to administer fluids, medications, blood products, or obtain samples for laboratory work-up. 3
Studies show that IO access can be obtained as fast as 20 seconds, allowing rapid access during emergencies that would otherwise be challenging to access intravenously. 4 Comparing success rate in IO versus IV access in pediatric out-of-hospital cardiac arrest showed that success rates were significantly higher in IO access attempts compared to IV access attempts (91.8% vs 70.7%). 5 The success in the first attempt in IO is 81.9%, with approximately 63.6% of pediatric patients having IO access completed within 3 minutes. 6 Neonatal and pediatric critical care transport services have highlighted that early insertion of an IO access facilitates early volume expansion, timely delivery of critical drugs, and allows time for retrieval teams to gain more definitive venous access. 7 Therefore, American Heart Association (AHA) recommends IO access as the preferred alternative when IV access is not obtained within 30 seconds of pediatric resuscitative care given the safety, effectiveness and short procedure time of IO access.8,9
Although the crucial value of IO access in critically ill patients is widely acknowledged, its use is limited by several existing barriers. These barriers include infrequent IO use in pediatrics and therefore lack of prior experience in IO placements, training, confidence in the indications for using IO.10,11 Literature review notes that IO clinical exposure is limited amongst physicians-in-training across specialties. Assessing procedural competencies amongst 89 internal medicine residents at a tertiary care center in the United States showed that only 7% of these residents had experience with IO access placement. 12 Currently, the Accreditation Council for Graduate Medical Education does not enlist IO access placement as one of the mandatory requirements in pediatric residency training.13,14 Further, highlighting similar gaps in IO access training amongst pediatric residents globally, IO access is listed as 1 of the top 5 procedures in simulation-based training. 15
We, therefore, present this study that aimed to create a much-needed simulation-based curriculum targeted at novice pediatric residents to teach IO access.
Methods
Study Design
This was an empirical investigation study which evaluated the performance of a novel simulation-based procedural curriculum. The study was conducted at a children’s hospital-within-a-hospital at an urban setting. The curriculum development and study design were introduced at the middle of 2 consecutive academic years between December 2021 to December 2022. Participants were selected from interested pediatric residents of all 3 post-graduate year (PGY) levels of training. Eligibility criteria included pediatric residents currently enrolled at the residency program at a first, second, or third PGY level. Exclusion criteria included residents who have participated in the study’s curriculum in previous training sessions. Subjects were enrolled following an informed consent process and training took place at the hospital during didactic hours. There were multiple educational sessions held during that period to facilitate small-group learning. The study was approved by the institutional review board (1749965-2).
Curriculum Components and Evaluation
The curriculum included 2 main interventions: (1) an online self-paced didactic module and (2) small-group simulation-based training sessions conducted by trained instructors. Learning objectives were developed in a similar manner to Kern’s framework 16 by evaluating existing gaps in residency training, setting clear goals for learners, and identifying clinical best-practices in IO procedure via literature review and consensus opinion of faculty pediatric intensivists (Figure 1).

Learning objectives for the intraosseous procedural training curriculum for pediatric residents.
Pediatric residents who were available to attend scheduled training sessions were approached about participation in the study, provided information about the study, and given the option to opt out of the study and only participate in training as learners. All residents were sent links to the online module and were asked to complete it asynchronously within 1 week prior to attending the training sessions. Those who agreed to enroll in the study were also asked to complete a baseline demographic and knowledge survey before starting the online module (see Supplemental Digital Content 1 and 2 for the full survey questionnaires). All residents received the same hands-on training sessions regardless of study enrollment. Those enrolled were evaluated on their baseline skills performance using a skills assessment tool prior to the beginning of the training session (Figure 2).

Skills assessment tool.
Training sessions were led by Pediatric Advanced Life Support (PALS) instructors and started with a summary of the knowledge module followed by hands-on teaching of the use of IO drills, needles, catheters, and stabilizing equipment on simulated trainers including bone replicas and chicken eggs. Immediate feedback was provided to participants during the hands-on portion regarding their technique and dexterity. Each training session included 15 to 20 participants and 4 PALS instructors and lasted 45 minutes. There was a total of 2 sessions each quarter spanning 2 academic years, resulting in 16 total sessions for the duration of the study. Residents who trained in previous sessions were able to attend new sessions in the next academic year but were not re-enrolled in the study. Following completion of the training sessions, enrolled participants were asked to fill out a follow-up knowledge survey and were re-evaluated using the skills assessment tool by 2 raters. Post-intervention evaluations took place anywhere between 3 and 6 months to evaluate skills and knowledge retention, and the timing varied between participants based on their availability for the evaluation. The timeline of the study interventions and participants’ evaluation is shown in Figure 3.

Timeline of curriculum and resident evaluations.
Study Data and Variables
The demographic survey collected data on participants’ PGY level, medical school graduation country of origin (American vs International Medical Graduate), history of training in IO access procedure prior to residency, and participation in both real-life and simulated pediatric codes. The skills assessment tool was derived from various published resources on IO procedural competency checklists available at the time of developing the study.1-3 The tool addressed areas not included in the knowledge survey where technical skills were predominantly targeted, included choice of correct equipment, anatomy, manipulation techniques, and completion of the procedure. Both the knowledge survey and the skills assessment tools were developed by consensus agreement between 2 pediatric intensivists and 4 PALS instructors following an in-depth literature search of proper IO cannulation techniques1,2 and went through multiple rounds of review until agreement was reached. The skills assessment tool was scored independently by 2 study members who observed each participant complete the procedure during baseline and post-intervention evaluations. Prior to data collection, raters completed a structured calibration session, including joint scoring of sample cases to ensure alignment in interpretation. Raters were blinded to each other’s scores. Some evaluations were conducted by only 1 rater due to time limitations. The knowledge survey included 9 multiple-choice questions and 11 true-and-false questions that tested participants’ comprehension of various procedure components including anatomy, indications, contraindications, complications, and technique. A perfect score would come to 36 if all the choices in the multiple-choice questions were correctly picked. The skills assessment tool addressed participants’ competence in using the IO equipment on the same simulated trainers (eg, bone replicas) used during training session.
Statistical Analysis
The primary measure was successful performance of the procedure during the post-intervention phase measured by achieving a passing score of 4 or higher in the skills assessment tool. The score was a numerical value that was calculated from the 6 parameters on the skills assessment tool and was averaged between 2 expert observers for each participant. Overlapping scores were averaged while single scores were included as is in analysis. Inter-rater reliability was evaluated by percent agreement to quantify consistency between the 2-raters. The secondary measure included relative improvement in knowledge scores between baseline and post-intervention phases. Categorical variables including demographic data were analyzed using a χ2 test. Median and interquartile range of the continuous variables including knowledge and skills assessment scores at baseline and post-intervention were calculated using a Wilcoxon Signed Rank test. The effects of baseline and post-intervention scores across different PGY levels were compared using a regression model (simple and multiple linear regression model) and the Wilcoxon signed rank test and plotted on a box plot. All analyses were performed using RStudio.
Results
A total of 68 pediatric residents were enrolled in the study. Sixty-one of 68 participants graduated from international medical schools. There was a similar representation across all 3 PGY levels and prior IO training experience. Forty-nine percent of participants had no experience with real-life pediatric codes, while most had some experience with simulated pediatric codes (Table 1).
Results of the Demographics Survey at Baseline.
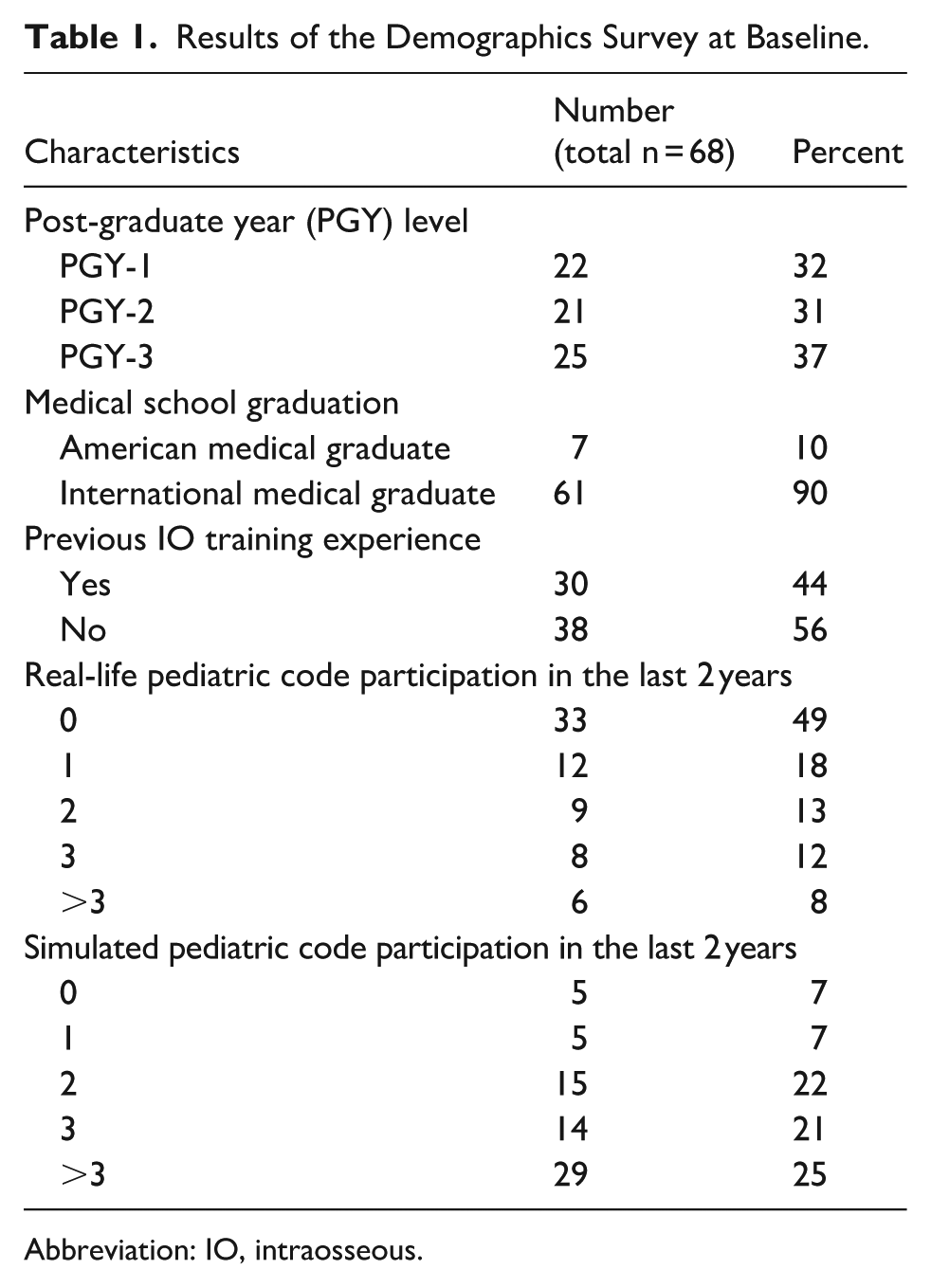
Abbreviation: IO, intraosseous.
The average time between baseline and post-intervention evaluations was 4.8 months (range 4.1-5.4 months).
Skills assessment scores were collected for 42 participants by the first rater and 47 participants for the second rater during both phases resulting in 49 total participant scores for comparison (72% of total enrolled). The skills assessment scores significantly improved from a baseline of 0 (95% CI 0,1) to post-intervention of 5 (95% CI 4,5, P < .001). Similar results were appreciated when each rater’s scores were analyzed separately. There was a 90% agreement when evaluating inter-rater reliability. Knowledge surveys were completed by 51 participants (75% of total enrolled) at both baseline and post-intervention phases. Knowledge scores significantly improved from 19 (95% CI 16, 21.25) at baseline to 25 (95% CI 22, 28.5, P < .001; Table 2).
Results of the Knowledge Survey and Skills Assessment Tool at Baseline and Post-Intervention.

IQR = interquartile range, both IQR and median are compared using Wilcoxon Signed rank test.
Skills score is a numerical value on a scale from 0 to 6, passing score was defined as a score of 4 or more. Average score used data from either the average of 2
Knowledge score is a numerical value on a scale from 0 to 36.
At baseline, sub-group analysis showed that there was no statistically significant difference in both knowledge and skills assessment scores when comparing residents of the 3 PGY levels (Figure 4). Similarly, no statistically significant difference was detected while comparing baseline knowledge and skills assessment scores with previous IO training prior to residency. Analysis of baseline data revealed a weak positive correlation of the baseline knowledge scores with residents’ experience in real-life pediatric codes (r = .31) and simulated pediatric codes (r = .24). No correlation was identified with the skills assessment scores.

Comparison of knowledge and skills scores at baseline between different PGY levels.
Discussion
This study demonstrated significant improvement in pediatric residents’ knowledge and skills following a structured simulation-based procedural training curriculum for IO access. Research specifically focusing on pediatric residents for this particular procedure is sparse and is primarily performed in the emergency department setting.13,17,18 Therefore, evaluating the outcomes of IO access teaching within pediatric residency is crucial in developing effective and targeted curricula. Our study included residents from all 3 years of training, including interns, which sets it apart from other studies that focused on senior residents. 19 The improvement in knowledge and skills scores across all PGY levels underscores the value of initiating such curricula early in residency training.
The focus of the curriculum evaluation was to obtain objective measures of improvement while examining acquirement and retention of both theoretical knowledge and practical skill. Previous studies tested either one of the objective measures or other subjective factors such as comfort and confidence in procedure performance.11,18,20 A large Canadian study highlighted the need to prioritize IO access training based on self-assessed questionnaires completed by pediatricians. 11 Another study demonstrated the infrequent experience with IO access among pediatricians through self-reported surveys conducted by the Canadian Pediatric Surveillance Program (CPSP). 20 Similarly, a study in a pediatric emergency setting assessed knowledge and comfort levels in IO access before and after training but did not further elucidate change in skill performance. 18
The outcomes of this study align with existing literature on the beneficial impact of simulation-based procedural training in various aspects of resuscitation. Furthermore, they highlight the aspect of skill decay following educational sessions, particularly for procedures not performed frequently. 21 Notably, 30% of the pediatric residents in our cohort had received some form of IO access training prior to residency; however, we did not expand on the methods or time of training in this subgroup. Despite this, their baseline scores were comparable to those without prior training. Our post-intervention evaluations showed that both knowledge and skills were retained at an average of 5 months following the simulations-based curriculum, which emphasizes the need for ongoing training to minimize skill decay over time. Long-term sustainability plans to address this include as just-in time training, hands-on refreshers during PICU rotations, or integration of IO skills into a recurring longitudinal comprehensive procedural curriculum.
Study Limitations
The study was conducted in a single, urban, academic institution on residents on a single track of training which may lead to difficulty in generalizing its outcomes on other populations. However, given the simplicity and low cost of the curricular design and low-cost of training, adaptations of this methodology can be applied to other training settings such rural programs or other tracks who may benefit from such training such as emergency, internal, or family medicine programs. While our outcomes delineate successful retention after an average of 5 months, it does not further evaluate longer-term retention of acquired skills and knowledge. Additionally, although improvement of scores was noted in the simulated setting, direct translation of the learned skills onto real patients was not evaluated and the impact of educational curricula on patient outcomes is not determined.
Conclusion
This study adds to the existing knowledge that simulation-based training for urgent and emergent procedures in pediatrics is beneficial when taught in a structured curriculum. More studies are required to evaluate the translation of knowledge and skills to the bedside and the effect of ongoing training over frequent intervals on skill retention.
Supplemental Material
sj-docx-1-gph-10.1177_30502225251405338 – Supplemental material for Simulation-Based Training in Intraosseous Access: Improving Procedural Skills in Pediatric Residents
Supplemental material, sj-docx-1-gph-10.1177_30502225251405338 for Simulation-Based Training in Intraosseous Access: Improving Procedural Skills in Pediatric Residents by Reem S. Saadoon, Ramya J. Sivasubramanian, Christina Kim, Rose Calixte and Sule Doymaz in Sage Open Pediatrics
Supplemental Material
sj-docx-2-gph-10.1177_30502225251405338 – Supplemental material for Simulation-Based Training in Intraosseous Access: Improving Procedural Skills in Pediatric Residents
Supplemental material, sj-docx-2-gph-10.1177_30502225251405338 for Simulation-Based Training in Intraosseous Access: Improving Procedural Skills in Pediatric Residents by Reem S. Saadoon, Ramya J. Sivasubramanian, Christina Kim, Rose Calixte and Sule Doymaz in Sage Open Pediatrics
Footnotes
Acknowledgements
We would like to thank Dr. Jennifer Sherwin and Dr. Silvia Schibeci Oraa for their contribution to the curriculum implementation and training sessions.
Ethical Considerations
This study received ethical approval from the State University of New York (SUNY) Downstate Health Sciences University IRB (approval #1749965-2) on December 1, 2021. This is an IRB-approved study, all participant information was de-identified and participant consent was not required. Participant data will not be shared with third parties.
Consent to Participate
Waiver of informed consent was approved by the SUNY Downstate Health Sciences University IRB & Privacy Board as per section 3 of the waiver of informed consent policy, which states that the research presents no more than minimal risk of harm to research participants and involves no procedures for which written consent is normally required outside of the research context. The participants were provided with informational sheets describing the research goals, details about contacting research staff, and opt-out information.
Author Contributions
All authors made substantial intellectual contributions to the design, execution, analysis, and interpretation of the work, drafting and revising the manuscript critically for important intellectual content, giving final approval of the version to be published, and taking accountability for all aspects of the work, including accuracy and validity of the contents, and ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is no longer available as abided by SUNY Downstate Health Sciences University policy on data storage, which states that records that are retained digitally in a REDCap database will be destroyed in conformity with the General Retention and Disposition Schedule for New York State Government Records with respect to categories of state government records included therein or with the State University of New York Records Retention and Disposition Schedule with respect to education and other SUNY-specific records.
Supplemental Material
Supplemental material for this article is available online.
Trial Registration Number/Date
Not applicable.
Grant Number
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.