
Abstract
Background:
Efforts to improve malaria treatment outcomes may fail if household decision-making, particularly in Nigeria, is overlooked.
Objectives:
We assessed how sociodemographics and house decision-making dynamics influenced presentation timing among children with severe malaria at a secondary facility in northcentral Nigeria.
Methods:
A cross-sectional study was conducted among children admitted with severe malaria. Data on sociodemographics, household decision-making, presentation timing, and outcomes were collected and analyzed. Delayed presentation was defined as arrival >24 hours after symptom onset.
Results:
Among 146 children, 69.2% (101/146) presented late. Most were male, 59.6% (87/146), and under five, 65.1% (95/146). Common reasons for delay included failure to recognize child’s illness, 44.6% (45/101), and lack of fund, 38.6% (39/101). Waiting for the father’s decision was associated with presentation timing. Socioeconomic class independently predicted delayed presentation (AOR 3.05, 95% CI 1.10-8.48).
Conclusion:
Nearly two-thirds of children presented late. Father-dependent decisions and socioeconomic status influenced presentation timing.
Introduction
Malaria remains a disease of public health significance in Africa. In 2023, African countries accounted for 94% of the 263 million global malaria cases and 95% of the 597 000 malaria-related deaths. 1 Among African countries with a significant malaria burden, Nigeria ranks first, with malaria contributing substantially to hospital admissions and mortality, particularly among children under the age of five.2,3 Many factors, including access to diagnostic services, appropriateness of interventions, and timing of presentation, influence the outcomes of childhood severe malaria.4,5
Due to the risk of poor outcomes, the timing of presentation of children with severe malaria is considered delayed if a patient presents more than 24 hours after the onset of symptoms. 6 A delay in malaria treatment significantly increases the risk of progression of severe malaria and subsequent poor outcomes.4,5 It has also been reported that general healthcare barriers, including socioeconomic status, educational background, geographic location, and caregivers’ healthcare-seeking behaviors, affect the timing of seeking healthcare services.7 -9 However, the role of household decision-making, which remains unexplored, may critically influence how a child with malaria presents for healthcare services in an African sociocultural setting. In pediatrics, household decision-making is influenced by the parents’ socioeconomic status, cultural beliefs, health literacy, family roles, and external influences such as community norms. 10 Interventions focused solely on increasing access to malaria treatment, without considering the household decision-making dynamics, may fail to produce the desired outcomes. Caregivers’ decision-making processes are known to play a crucial role in determining when and where medical care is sought. 11 Therefore, this study examined the influence of household decision-making dynamics, including the role of extended family members, family income, and socio-demographics, on the timing of presentation among children with severe malaria at a secondary health facility in northcentral Nigeria.
Materials and Methods
Study Design and Setting
This cross-sectional study involved children admitted for severe malaria between 1 July 2023 and 15 February 2025 at a secondary health facility in northcentral Nigeria. The hospital is a government-owned health facility located in Ilorin, Kwara State, northcentral region of Nigeria. The hospital is a referral center for primary health centers (PHCs), secondary health facilities, and private hospitals within and outside the city (Ilorin). The hospital has 35 in-patient beds, including a dedicated emergency pediatrics unit (EPU) for the stabilization of critically ill children. A consultant pediatrician leads the emergency team, with support from general practitioners, interns, and nursing staff. The overall staff at the facility for delivering healthcare services included 5 pediatricians, 7 general practitioners, 4 interns, 20 nurses covering the EPU and ward, and 15 laboratory personnel. The hospital offers outpatient clinics, inpatient care, and 24-hour pediatric emergency healthcare services to children.
Study Population
The study included all admitted children (3 months to 15 years) diagnosed with severe malaria confirmed with a rapid diagnostic test for Plasmodium falciparum and the presence of 1 or more clinical features of severe malaria, as described in the Nigeria national malaria management guidelines. 12 This study excluded children with chronic diseases, such as sickle cell disease, chronic kidney disease, and other non-malarial diagnoses during the study period.
Sample Size Estimation
The minimum sample size for this study was estimated using an online sample size calculator (http://www.raosoft.com/samplesize.html) and the proportion of severe malaria among children admitted at another health facility in the state. Using a prevalence of 18.6%, 13 (the prevalence of severe malaria reported in another facility in the same state), at a 95% confidence interval and margin of error of 5%, we obtained a minimum sample size of 230. By applying infinite population corrections from 390 total admissions reported in the years 2021 and 2022 (hospital records) in our facility, we obtained a final sample size of 146. 14
Sampling Technique
We used a non-probability purposive sampling technique to consecutively recruit all children and adolescents who met the study inclusion criteria until the required sample size was attained. Individuals who did not meet the eligibility criteria or who declined consent/assent were excluded from the study.
Delayed presentation was defined as any child who presented with clinical features of severe malaria 24 hours after the onset of symptoms. 6
Data Collection Instruments
After the literature review, we developed structured questionnaires that comprised 4 sections: (i) sociodemographic characteristics, including socioeconomic status; (ii) clinical and laboratory features of severe malaria; (iii) timing of presentation and reasons for any delay; and (iv) in-hospital outcomes of the patients. The drafted tool was piloted and further refined prior to the data collection. Household socioeconomic status was assessed using the Oyedeji socioeconomic classification, which derived a child’s social class from both parents’/caregivers’ highest educational attainment and occupations. 15 Each parent’s education and occupation were ranked on a 5-point scale. The average of the 2 scores from education and occupation was rounded to the nearest whole number and assigned a final social class (I-V). The social classes were further classified into upper (I-II), middle (III), and lower (IV-V).
Data Analysis
Data were entered into an Excel spreadsheet and analyzed using the IBM SPSS version 29. The age was classified as infants, under 5 and above 5 years old. The sociodemographic parameters, including parents’ educational level, family income, and household decision-making, were presented as a frequency table and later cross-tabulated with the timing of presentation. Variables significant in two-by-two tables from household decision-making, clinical features, and sociodemographics were entered into binary logistic regression models to determine variables associated with delayed presentation, and results were presented as odds ratios along with 95% confidence intervals (CI). Statistical significance was set at P < .05.
Ethical Approval and Consideration
The Kwara State Ministry of Health Ethical Review Committee approved the study prior to the commencement of the study (Approval number: MOH/KS/EU/777/464). This study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from the parents and caregivers of the children after a detailed explanation of the study. Data were entered into a password-secured computer and maintained with absolute confidentiality.
Results
General Characteristics of the Study Children
Of the 146 children in the study, 69.2% (101/146) had a delayed presentation to the hospital to address malaria symptoms. Most children were male, 59.6% (87/146), and under 5 years old, 65.1% (95/146). Most of the parents of children in the study had a secondary level of education (Table 1), belonged to middle socioeconomic classes, and most had a cumulative family income of less than 70 000 Naira per month, 5.5% (81/146) (Table 1).
General Characteristics of the Children With Severe Malaria.

Monthly minimum wage in Nigeria.
Of the 146 children in this study, 47 (32.1%) were referred from health facilities, while the remaining were self-referrals, and most received antibiotics and antipyretics before presentation (Supplemental Table 1).
Relationship Between Timing of Presentation and Household Decision-Making
The most common reasons for delayed presentation included caregivers/parents who did not recognize that the child was sick, 44.6% (45/101), and no money to bring the child to the hospital, 38.6% (39/101). Among household decision-making factors, only waiting for the father’s decision was associated with the timing of the presentation (Table 2).
Relationship Between Households’ Decision Making and the Timing of Presentation Among Children With Severe Malaria.

Fischer’s exact test.
Inability to consider early symptoms as an illness that requires care or a healthcare visit.
Relationship Between Timing of Presentation and Socio-Demographics
Age, sex, parental education level, and family income were not associated with the timing of presentation at the hospital. However, socioeconomic class was associated with the timing of presentation (Table 3).
Relationship Between General Characteristics and the Timing of Presentation Among Children With Severe Malaria.
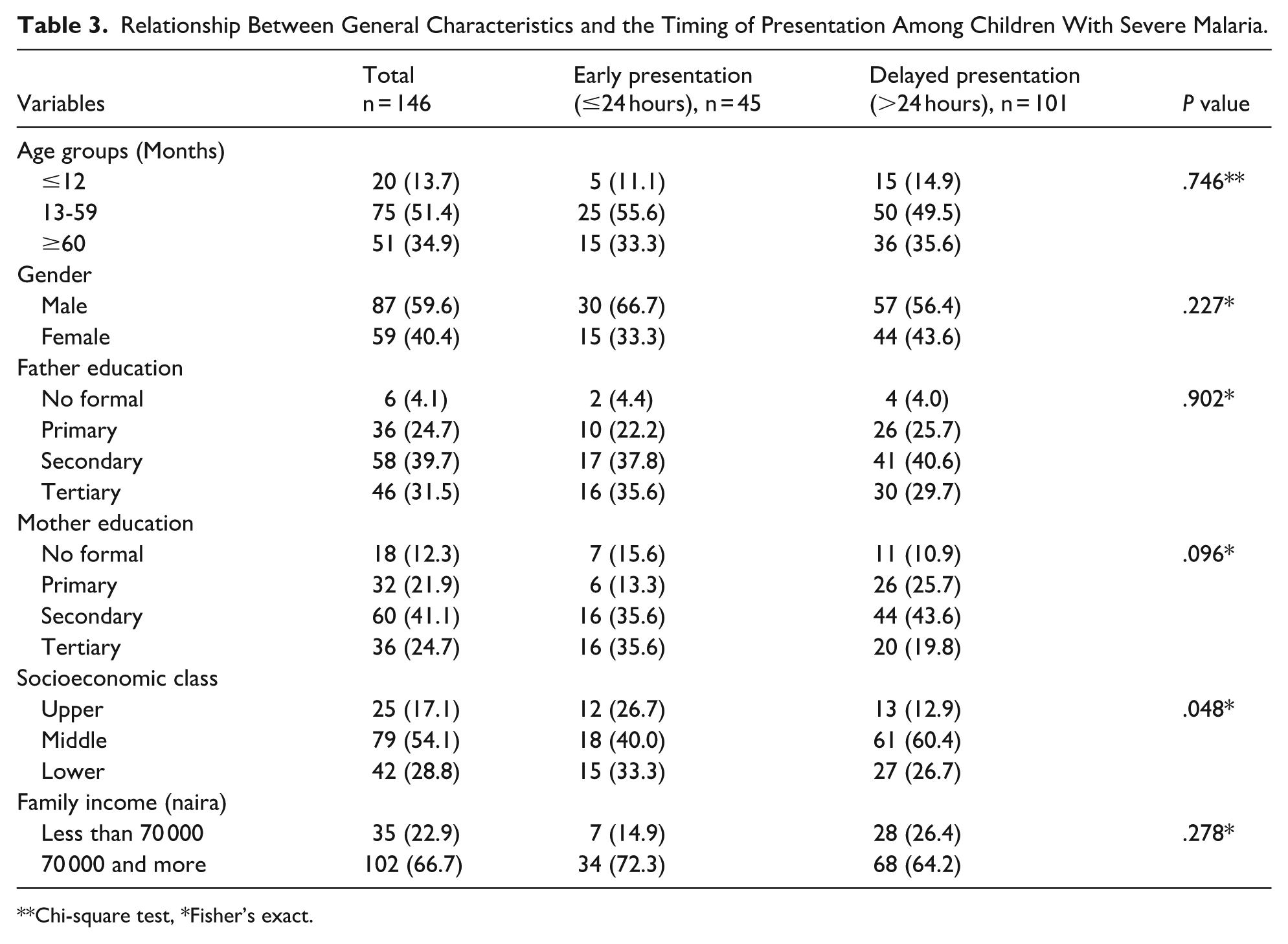
Chi-square test, *Fisher’s exact.
Relationship Between Timing of Presentation and Clinical Features
Most clinical features were not associated with the timing of presentation, except for paleness (P = .029) and dark urine (P = .019) (Table 4). Of the 146 children, 2 deaths occurred, with a case fatality rate of 1.4%, which was not significantly related to the timing of presentation (Table 4). The 2 deaths occurred in 2 children with cerebral malaria and disseminated intravascular coagulopathy.
Relationship Between Clinical Features and the Timing of Presentation Among Children With Severe Malaria.

Fisher’s exact.
Factors That Are Associated With Delayed Presentation
In household decision-making, only the factor of waiting for the father’s decision was associated with delayed presentation. After adjusting for confounders, only socioeconomic class significantly predicted delayed presentation (middle class with an adjusted odds ratio of 3.05, 95% confidence interval (CI) 1.10-8.48) (Table 5).
Binary Logistic Regression of Factors That Are Associated With Delayed Presentation Among Children With Severe Malaria.

Abbreviations: β, beta coefficient; SE, standard error; AOR, adjusted odds ratio; CI, confidence interval.
References-No.
Discussion
Timely presentation is among the determinants of outcomes in childhood severe malaria.4,16 In this study, more than two-thirds of the participants presented to the hospital 24 hours after the onset of symptoms, highlighting a significant delay in seeking care for severe malaria. Our findings are comparable to reports from other common childhood diseases in Ethiopia and Uganda, where children with common childhood illnesses had a significant delay before presentation to health care facilities.17,18 However, our prevalence is far higher than the 37.3% reported among children with severe malaria in southwestern Nigeria. 9 The higher prevalence observed in this study may be due to the definition cut-off point used for this study (24 hours) compared with 72 hours used for the southwestern Nigerian study. 9 This observation reinforces the need to encourage early presentation of a sick child to a health facility, especially in malaria-endemic regions such as Nigeria. This will ensure early intervention and further mitigate the progression of illnesses such as severe malaria.
Household decision-making in accessing health is a critical factor in African culture, where the power lies within a certain group of family members. 18 Financial constraints and non-recognition of illness are also well-documented barriers to delayed presentation, which are not significant in this study, suggesting the possibility of other moderating factors.19 -22 However, the significant association between delayed presentation and waiting for the father’s decision underscores the paternal influence on the timely seeking of appropriate healthcare services. This dynamic not only limits the autonomy of primary caregivers, mostly mothers, but also increases the risk of delays, especially in life-threatening emergencies such as severe malaria. This finding aligns with observations from studies in Ethiopia and Uganda, where caregivers often delayed seeking appropriate care due to the need for consultation with male household heads or grandparents.17,18 These patterns suggest that interventions aimed at reducing malaria treatment delays should not only address economic and educational barriers but also incorporate gender dynamics/decision-making within households. Also worthy of note is the large adjusted OR in the multivariable logistic regression for “waiting for the father’s decision,” which likely reflects sparse-data bias from a small subgroup, yielding an unstable, inflated estimate rather than evidence of a significant actual effect. The effect of “waiting for the father’s decision” would have been better assessed with a large subgroup that would allow its exact impact to be measured, rather than the statistical artifact observed in this study.
Socioeconomic class was significantly associated with delayed presentation in our study, which aligns with a study in Southwestern Nigeria. 9 Socioeconomic class reflects the dynamic status of the family in terms of educational levels and occupation, which are critical in determining the economic empowerment that could influence caregivers’ decisions to bring their sick child early for medical care. Similarly, our findings are similar to those of other authors who indirectly assessed socioeconomic class using the financial power of caregivers in delayed presentation for childhood illnesses, including severe malaria.18,20
Among the clinical features, paleness and passage of dark-colored urine have emerged as important clinical indicators that influence the timeliness of accessing healthcare services. Our findings align with those of Mpimbaza et al, 7 who reported a significant association between delayed presentation and severe anemia in children with malaria. Notably, all patients with reduced urine output, jaundice, and abnormal bleeding were late for treatment. Most earlier studies did not test this association, except for a Nigerian study 9 that tested a few clinical features that were not significant. The association between paleness and dark urine reflects the progression of malaria infection without intervention and further supports the need for caregivers of sick children to seek medical care early.
After controlling for potential confounders, socioeconomic class remained the only significant predictor of delayed presentation, with children from middle-class households showing more than 3 times the odds of late presentation compared with those from higher socioeconomic backgrounds. Interestingly, the vulnerability of the middle socioeconomic group may stem from the double disadvantage of not possessing either the financial resilience of upper-class households or the external support often directed at the poorest 23 ; hence, the likelihood of a late presentation when their child falls sick. This finding suggests the need to provide support for the middle class and ensure that their social class does not become a barrier to accessing healthcare for children with severe malaria.
The mortality rate in this study is low (1.4%, 2/146), which is consistent with the reduction in mortality observes in other studies in Nigeria.3,13 Also, the state government policy of free treatment for malaria, including artesunate, at our facility, which ensured access to artesunate and other management support irrespective of the social status, may also contributed to improved outcomes. This policy ensured that all children with severe malaria received intravenous artesunate at presentation. In addition, it is worth noting that the 2 deaths in this study occurred in children who presented after 24 hours, which further reinforced the poorer outcomes with delayed presentation. This finding highlights the need to continue to emphasize early presentation of sick children in malaria-endemic settings for prompt diagnosis and appropriate intervention.
Public Implications of the Study
The implication of almost two-thirds of children with severe malaria in this study presenting late to the health facility demonstrated the need to carry out health education targeting community members on the significance of early presentation of a sick child. This will ensure prompt intervention and prevent the progression of the child’s illness. Among the cited reasons for delayed presentation (almost 40% of the caregivers) was a lack of funds. Funding has been a critical part of healthcare barriers in resource-constrained settings, including Nigeria. 24 Addressing funding barriers will include the need to consider alternative healthcare financing options, such as community health insurance, which has been documented as successful in resource-constrained settings. 25 In African settings, fathers are seen as the head of the family and mostly with final authority in decisions, including health seeking care for a sick child. Active community engagement, including strengthening female education and empowerment to allow women to make decisions, especially regarding a sick child, will go a long way in improving the outcomes of childhood severe malaria.
Study Limitations
Although this study prospectively gathered data from children with severe malaria, it had some limitations. While this was a quantitative study, a qualitative exploration of household decision-making via detailed interviews with caregivers may have provided a broader perspective for delayed presentation. This study provides insight into the possible associations between household decisions and delays in seeking treatment in children with severe malaria; however, its cross-sectional design meant that it could not provide causal inference between them. This was a single-center study with a relatively small sample size of 146, which limited the generalizability of the findings. In addition, the caregivers’ responses may be subject to recall bias, although they were obtained at admission during recruitment. Even though the health facility is located within the metropolis, this study did not explore the possible role of geographical distance to the facility.
Conclusion
This study shows that more than two-thirds of children with severe malaria have a delayed presentation. In household decision-making, waiting for the father’s approval to visit the hospital and socioeconomic status were associated with the timing of presentation among children with severe malaria. Public health interventions aimed at reducing the burden of malaria in Nigeria should consider improved living standards and male involvement through health education programs.
Supplemental Material
sj-docx-1-gph-10.1177_30502225251393787 – Supplemental material for Influence of Sociodemographic Factors and Household Decision-Making on the Delayed Presentation of Childhood Severe Malaria at a Secondary Facility in North-Central Nigeria
Supplemental material, sj-docx-1-gph-10.1177_30502225251393787 for Influence of Sociodemographic Factors and Household Decision-Making on the Delayed Presentation of Childhood Severe Malaria at a Secondary Facility in North-Central Nigeria by Amudalat Issa, Aisha Funmi Lawal, Mosunmola Folorunsho and Olayinka Rasheed Ibrahim in Sage Open Pediatrics
Footnotes
Acknowledgements
We thank the staff of Children specialist hospital, Ilorin, Nigeria for the care of the recruited children.
Ethical Considerations
Kwara State Ministry of Health Ethical Review Committee approved the study prior to the commencement of the study (Approval number: MOH/KS/EU/777/464). This study was performed in accordance with the Declaration of Helsinki.
Consent to Participate
A written informed consent was obtained after a detailed explanation of what the study entailed to the parents and caregivers of the children. Data were entered into a password-secured computer and maintained with absolute confidentiality.
Author Contributions
Amudalat Issa was involved in the conceptualization, data curration, data visualization, data analysis, literature review, draft and approved the final version. Aisha Funmi Lawal was involved in the conceptualization, data curation, data visualization, literature review, draft and approved the final version. Mosunmola Folorunsho was involved in the conceptualization, data curation, data visualization, literature review, draft and approved the final version. Olayinka Rasheed Ibrahim was involved in the conceptualization, data curation, data visualization, data analysis, literature review, draft, critical appraisal and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The raw data file could be provided for research purposes only, upon request, via e-mail from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.