
Abstract
Background and Purpose:
Glucocorticoids bursts may be harmful. We aimed to explore their prescribing patterns in our pediatric ambulatory setting.
Methods:
All children scheduled for their well-child checkups from May to November 2022, upon entering and leaving primary school, were included. In parallel, case notes were reviewed for glucocorticoid prescriptions due to wheezing or acute skin conditions from birth to the consultation date.
Results:
We recruited 79 children, 34 (43%) received at least 1 glucocorticoid burst. Most children were prescribed glucocorticoids against wheezing, it accounted for 48 short courses of glucocorticoids, divided into 40 (83%) for preschoolers up to 6 years of age, and 8 (17%) for schoolchildren beyond age 6. Thirteen children have been prescribed glucocorticoids bursts due to acute skin conditions, mainly dermatitis or insect bites.
Conclusion:
Pediatric glucocorticoids overuse is a common finding in our community.
Keywords
Introduction
The short-term oral use (defined as bursts or short courses for <15 days) of glucocorticoids (GCs) has been considered safe for the past 4 decades. However, over the last years, we have seen mounting evidence of its frequent or significant detrimental effects on children’s metabolism and immune response.1,2 This should mark a turning point in the tendency to overtreat children wrongly perceived as at risk.
For these safety reasons, because alternative treatments are available,3,4 and because it is often an indicator of poor compliance with proper wheezing treatment, 5 GCs bursts are now only indicated for wheezing exacerbations in schoolchildren when serious emergencies arise. 6 In addition, current policy discourages the ubiquitous use of GCs for the most common acute rashes in Pediatrics. 7
Despite the widespread confirmation of these statements, doctors have been slow to adopt these guidelines. Notably, GCs has remained in the pharmacopeia for the treatment of childhood eczema or wheezy children, as initially presented.
Hence, our objectives are to record the GCs bursts prescriptions against wheezing or rashes from birth to the end of primary school in our area and to assess whether needless GCs prescriptions with safety risks occur in this area.
Methods
A retrospective cohort study was used to evaluate the pattern of prescribing GCs to children getting care in an outpatient setting. This is a secondary analysis, the data included in this study originate from case notes of all children who attended our pediatric clinics from May to November 2022 for scheduled well-child checkups and to complete a cardiological evaluation upon entering and leaving primary school.8,9 Children on long-term GC treatment were excluded, this was only the case for a girl with nephrotic syndrome; there were no missing cases. Our medical services consist of ambulatory clinics and emergency rooms that serve a socioeconomically diverse community of 27 000 people, including 4500 children under 15.
Information on patients’ characteristics and GCs prescription was collected from our medical files. We have recorded any short course of GCs prescribed to our participants for wheezing or rash from birth to their well-child consultation at ages 6 or 12.
Ethics
The Institutional Review Board approved the study’s protocol for Health and Medical Research (ECICAP:P122/29). Parents were asked to provide written consent for the prospective cardiological research, as well as for access to historical data regarding their children’s illnesses and treatments.
Statistics
Descriptive statistics have been used to summarize the data of this case series. The t-test and the chi-square test were used in bivariate analysis.
Results
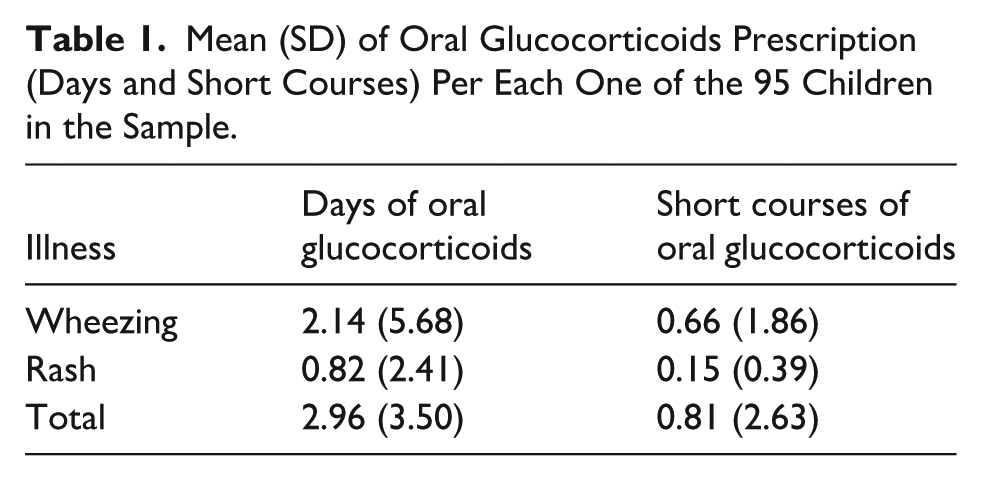
GCs were prescribed to almost half of the children enrolled in our sample at some point between birth and secondary school. We recruited 79 children, 34 (43%) of them received at least 1 GC burst. On average, the total of these children received 3 days and 1 burst of GCs in roughly 11 years of life (Table 1). Among GCs users, the median number of days per short course was 3 and the range of short courses per child was 1 to 10. We found no significant differences in baseline or somatometric characteristics between children who were ever and never prescribed GCs (Table 2).
Mean (SD) of Oral Glucocorticoids Prescription (Days and Short Courses) Per Each One of the 95 Children in the Sample.
Demographic and Somatometric Data by Glucocorticoid Prescription.

Data are mean (SD) unless otherwise specified.
Abbreviations: *<0.05; BMI, body mass index; NS, non significant.
As expected, the most common indication for GCs bursts was wheezing; 9 wheezy children were prescribed several GCs bursts, and 12 wheezy children were prescribed one such burst. Our wheezy participants were given 48 short courses of GCs, divided into 40 for preschoolers up to 6 years of age, and 8 for schoolchildren beyond age 6 (Table 3). Five out of 21 wheezy children on short courses of GCs had moderate or severe wheezing; only one of them was of school age. Most wheezy children with any GC dispensing (18 out of 21) did not have other utilization.
List of Cases With Oral Glucorticoids Prescriptions.

Thirteen children have been prescribed GCs bursts due to acute skin conditions, 38% of them had had dermatitis, 31% suffered an insect bite, and the remaining 31% were equally divided between urticaria, cellulitis, miliaria, scarlet fever, and urticaria (Table 3).
Discussion
Just under half of 79 children in urban ambulatory care received a GC burst for wheezing or rash at some point between birth and the end of primary school; 83% of children treated for wheezing were under 6 years of age, and 69% of those treated for a rash had dermatitis or an insect bite. The meaning of these treatments varies depending on whether they were prescribed for respiratory or skin conditions.
Wheezing
Two out of 5 children in our case series who were prescribed GCs received repeated GCs prescriptions, which is considered a red flag for poor bronchospasm control. 5 Unfortunately, these findings align with previous reports that show how between 15% and 50% of children receive more than 1 GC prescription. 10
Wheezy schoolchildren frequently present with eosinophilic, highly steroid-responsive airway infiltration. Conversely, in preschool wheezers, airway inflammation is primarily due to a neutrophilic response to viral triggers. 11 The use of GCs, given for decades to treat wheezy toddlers, was based on an extrapolation from studies conducted in asthmatic older children and adolescents who responded to this class of drugs. 12 A meta-analysis on the role of GCs in toddlers with wheezing exacerbations found no difference between GCs and placebo regarding unscheduled visits, and that outpatient toddlers treated with GCs had a higher hospitalization rate. 13 Accordingly, current guidelines remind us of the strong evidence against GCs bursts in preschool children with acute wheezing.6,14 We do not know what drives disregard for these guidelines. However, GCs dispensing rates are higher for wheezy preschoolers compared with older children in most available previous research 15 as well as in this case series. Regarding schoolchildren, current guidelines state that although clear evidence is lacking to support GCs use for those with mild exacerbations, closely monitored GC should be a part of the initial treatment of moderate to severe asthma attacks. 16 We have found that 83% of our patients who received GCs for wheezing were preschoolers, and just one of the schoolchildren in our sample had a moderate wheezing crisis that warranted treatment with GCs bursts.
Rash
One in 6 of our children was treated with GCs for acute skin disorders. About two-thirds of them had dermatitis or insect bites, and the rest had cellulitis, urticaria, miliaria, or scarlet fever. According to current standards, GCs should not be used for atopic dermatitis. 7 It is debatable whether GCs is helpful managing acute urticaria. 17 The effectiveness of concurrent systemic GCs in children with orbital cellulitis 18 is well-established. We have not found references to support GCs short courses to treat miliaria, scarlet fever, or irritation from insect bites.
Vast differences in the prescription of GCs have been described over time and space. There is an annual rise in GC use, 19 with a 30% increase in the UK over 2 decades and a 14% increase in France over 1 decade.12,20 In certain countries, the number of GCs prescriptions for children is about 20 times higher than in others. 21 It is unclear whether the extended use of GCs bursts can be attributed to the incidence of these medications’ approved indications or to irrational outpatient drug use. 11 However, the wide variation (15%-86%) in GC prescribing among pediatricians 15 must gain some relevance.
Over the last decade, research into the potential adverse effects of GCs bursts has intensified. A research involving 1.5 million adults unveiled that sepsis, thromboembolism, and fracture rates increased several-fold within 30 days of starting the medication and then decreased over the next 31-90 days. 2 A meta-analysis of twenty-two randomized trials involving GCs bursts in 3200 children documented 850 adverse reactions, including mood, gastrointestinal, circulatory, and endocrine disruptions. 22 In addition, descriptive research on over 1 million children who were prescribed GCs bursts has proved truly alarming in concluding that this treatment increases the risk of pneumonia or sepsis by about 100% within 1 month of starting the therapy at issue. 23 Fortunately, sepsis is a rare event, but pneumonia is a common finding among sick children.
To summarize, GC short courses conformed to the asthma guidelines in 2 patients, and it is doubtful whether they also conformed to the urticaria guidelines in 1 more patient, which totals 3 out of 62 treatments, or around 5% of the cases. These findings extend previous reports on the overuse of GCs in primary care, 24 which, in studies from other countries, accounts for 63% of total prescriptions, 25 particularly among young physicians or for patients under 15 years old. 26 There are several reasons for overtreatment: one is defensive medicine and another is the preference for receiving more medication by people with risk aversion. Since 90% of consultations end with a prescription in some regions, we must admit that a large part of Medicine is placebo. 27 According to our anecdotal experience, a high proportion of children in our health region have received improper GCs bursts prescriptions, which should not be an alternative to reduce the number of dissensions between clinicians and patients.
Limitations
Several limitations should be taken into consideration in our analysis of these cases. Data on non-compliance with prescribed medication are unknown in studies based on registry data. Many factors influence the decision to prescribe GCs; however, most of these, such as health literacy characteristics, parental and physician attitudes toward drugs, and differences in clinical guidelines or drug regulatory policies, were not examined in our study. Well-known differing directions in inpatient versus outpatient prescribing rates may lead to a wrong estimate of the amount of GCs overprescription since this case series was limited to children who sought health care in the community.
Asthma-like symptoms are common in young children, but diagnosing asthma at this stage in life is challenging due to the variability of wheezing phenotypes and a bunch of other reasons too. Therefore, this case series has focused on wheeze, which indicates airflow limitation, mainly due to mucosal swelling, mucus deposition, or bronchoconstriction. Wheezing has been used synonymously in clinical contexts to describe conditions such as bronchiolitis, bronchitis, and asthma. There is no agreed-upon definition of wheeze. This paper accepts wheezing as a high-pitched intrathoracic sound recorded by a healthcare professional that requires rapid symptom relief. 28
Conclusion
Until personalized treatments based on the molecular signature of each exacerbation are available, we not only acknowledge but also highlight that GCs bursts play a role in treating a group of children with severe wheezing or skin conditions. On the other hand, the results of this case series point to the need to reduce the overuse of GCs against acute cutaneous or respiratory conditions that do not pose a great threat to children in the outpatient setting. This approach is deemed particularly appropriate to adopt once we know that GCs use does not improve toddlers’ wheezing but does increase the risk of pneumonia by 100% in the short term. Further studies are needed to validate these findings in other pediatric populations and to strive to rebalance a worldwide trend toward higher rates of GCs short-course prescriptions.
Footnotes
Author Contributions
SV and MM conceived the study and SB and IP contributed towards planning and design of the study. A-ET and AF collected all the clinical data which was supervised by SB. SV and SB wrote the first draft of the paper and the other authors contributed to editing and finalizing the document. IP performed the statistical analysis. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.