
Abstract
Objectives:
To identify determinants of under-five child mortality in Somaliland using Cox Proportional Hazard models, focusing on socioeconomic, environmental, and maternal factors influencing survival time.
Introduction:
Under-five mortality is a critical health issue in Somaliland. This first-of-its-kind study investigated local risk factors.
Methods:
A retrospective analysis of the 2020 Somaliland Demographic and Health Survey (SLDHS) data was conducted. Cox Proportional Hazards models were employed to assess factors associated with time-to-death in children under 5.
Results:
Significant risk factors included reliance on wells (Adjusted HR = 3.96, P = .034) or other non-piped water (AHR = 3.31, P = .016), male-headed households (AHR = 2.29, P = .036), female child sex (AHR = 6.24, P = .024), and later birth order (AHR = 3.34, P = .012). Conversely, older maternal age (25-49 years) was strongly protective (P < .001).
Conclusion:
The study highlights the factors of under-five mortality. Interventions targeting interventions focusing on improving access to clean water, gender equity, and support for young mothers to reduce child mortality in Somaliland.
Keywords
Introduction
Under-five mortality remains a significant public health concern in Sub-Saharan Africa, with rates higher than global targets. Several common factors influencing child survival were identified across studies, including breastfeeding practices, birth intervals, and socioeconomic status. Children who were never breastfed had a higher risk of mortality. Short birth intervals (<24 months) were associated with increased mortality risk.1-3 Socioeconomic factors such as wealth index and maternal education also played a role. Additionally, factors like birth order, family size, and place of residence were significant predictors.2-4 Children’s intellectual and physical development is crucial throughout the first 5 years of life. 5 The under-five mortality rate is the probability that an infant will die before reaching the age of 5, expressed per 1000 live births. It remains a public health problem particularly in low-income countries despite the high impact of interventions made.3,4 Malnutrition continues to be a major global public health issue and a significant cause of child morbidity and mortality. 6 Although the under-five child mortality rate has decreased globally, from 5.9 million child deaths in 2015 to 5.3 million in 2018, there is still a high mortality rate in African nations, with Ethiopia having the highest rate at nearly 1/12 (81 deaths per 1000 live births), which is roughly 7 times higher than in European nations. 4
In 2021, it is estimated that approximately 5 million children under the age of 5 will lose their lives globally (UNICEF, WHO, World Bank Group, and United Nations, 2023). This represents a significant decline in the global under-five mortality rate, which has dropped from 12.5 million deaths in 1990 to 5 million deaths in 2021. 7 More than 25% of all under-5-year-old child deaths worldwide take place in Africa. 8 Somaliland (133/1000 live births), Chad (127/1000 live births), the Central African Republic (124/1000 live births), Sierra Leone (114/1000 live births), Mali (111/1000 live births), and Nigeria (104/1000 live births) were the top 6 African nations with the highest under-five child mortality rate in 2016, accounting for more than 50% of under-five mortality in Sub-Saharan African (SSA) countries and roughly 1/5 of under-five mortality globally. 8
With 1 child out of every 11 live births dying before the age of 5, the SSA continues to have the highest under-five child mortality rate in the world.9,10 So, the death of children under the age of 5 continues to be a major public health issue in the SSA. 11 According to the United Nations report, the head of the report indicated that Somaliland has one of the most severe maternal mortality rates globally. It is estimated to range from 105 to 140 deaths per 1000 live births.7,12 Somalia has made progress in reducing child mortality rates but still faces challenges in reducing under-five mortality. The under-five mortality rate decreased by 64.7% from 173 fatalities per 1000 live births in 2005 to 112 in 2021, but this rate is not as rapid as needed, and a significant portion of Somaliland infants still die before turning 5, highlighting the need for further efforts.
This study is the first of its kind in Somaliland to investigate the risk factors for under-five mortality. It provides valuable insights into Somaliland’s child health and survival, helping organizations, healthcare professionals, and policymakers work to reduce the rate. The research, based on the 2020 Somaliland Demographic and Health Survey, is crucial for conducting evidence-based research and informing targeted initiatives. It is the first study of its kind in Somaliland and provides a wealth of health and demographic data collected from a representative sample of people and households. This study’s main goal is to use the extensive information from the Somaliland Demographic and Health Survey (SLDHS) 2020 to gain a new understanding of the risk variables influencing under-five mortality in Somaliland.
A frail healthcare system and restricted access to high-quality healthcare services are the results of decades of violence and instability. Designing focused treatments and policies to enhance child health outcomes in the area requires an understanding of the risk factors linked to under-five mortality in Somaliland. Earlier research has examined the factors that contribute to child mortality in nearby nations like Ethiopia, Kenya, South Africa, and other African countries.8,13
The purpose of this study was to evaluate the possible predictor factors that contributed to Somaliland’s children under 5 having a lower survival time to death. The results of this study will help establish initiatives to extend the survival span of children under 5 in Somaliland, and it will also serve as a basis for future research. Somaliland, a country in the Horn of Africa, has particular difficulties concerning the survival and health of children because of its complicated political and socioeconomic environment. Therefore, the study aims to identify the primary determinants of child mortality in Somaliland using Cox Proportional Hazard models. It also explores how socioeconomic factors, such as maternal education and access to medical care, affect under-five mortality rates. The study also investigates the impact of environmental factors, such as clean water and sanitation services, on child mortality. The findings can inform strategies to reduce infant mortality and improve child health outcomes, ultimately contributing to sustainable development and child welfare in Somaliland.
Materials and Methods
Study Area
This study was conducted in Somaliland, East Africa, which borders Djibouti, Ethiopia, Somalia, and the Gulf of Aden. Covering 176 119.2 km², it has a mixed climate with both wet and dry seasons. Somaliland consists of 6 regions: Awdal, Marodijeh, Sahil, Togdheer, Sanaag, and Sool. With an estimated population of 4.2 million, the majority are Somali Muslims. Despite some economic growth since declaring independence, Somaliland faces slow progress due to a lack of international recognition, which limits investment and aid. Livestock remains a key livelihood for both rural and urban populations. 14
Study Design and Setting
A retrospective study design was utilized. This study utilized secondary data analysis from the 2020 Somaliland Demographic and Health Survey (SLDHS). The survey included a nationally representative sample of Somaliland households. It was conducted with the support of the Ministry of Health (MoH), Office of Statistics, the Ministry of Planning, and various partner organizations, including UNFP. The data collection period spanned from February 1, 2018, to January 31, 2019 and A total of 17 686 individuals were included in the survey.
Variables of the Study
Outcome Variable
The primary response variable was the time to death for each child, measured in months from birth until the end of the follow-up period. Events were defined as child deaths occurring between birth and 59 months (1 = died). Children who remained alive at the end of the follow-up period and had not yet reached 5 years of age were classified as censored (0 = censored).
Explanatory Variables
The primary factors connected with time-to-death among children under the age of 5 are type of birth child’s (single, multiple), region (regions), residence (urban, rural), source of drinking water (Piped born water, well, other source) toilet facilities (Flush/Pour Flush Toilet, Pit Latrine, other), sex of household head (female, male), wealth index combined (lowest, second, middle, fourth and fifth) birth order (first, second and above) sex of child (male, female), duration of breastfeeding (Ever breastfeed but not breastfeeding no, never breastfeed), place of delivery (her home, other home, government, referred to health center, MCH HC, primary health unit (PHU), mobile clinic, other private medical center and other) exclusively breastfeeding (yes, no), mother’s age (in year; 34 and below, 35-40, 41 and above), and child vaccinated (no, yes, do no know), Size of Child at Birth (very large, larger than the average, average, smaller than average and very small), age of mothers at first birth (>18, ≤18), mother current age (15-24, 25-34, and 35-49) and mother education (no education, primary, secondary and higher); they were chosen for this investigation from the available similar studies on the topic.
Statistical Analysis Method
The data for this study were obtained from the SDHS 2020 individual (women) record file using STATA version 17 software. The extracted dataset was recorded and cleaned by checking frequencies, listing, and sorting to identify any missing values. Descriptive statistics were used to summarize socio-demographic characteristics. The study employed the Cox Proportional Hazards model to analyze the determinants of under-five child mortality in Somaliland. Hazard ratios (HR) were estimated to assess the impact on the survival of under-five children. A Kaplan–Meier survival curve was utilized to assess the time (in months) until the Under-Five Children. Data analysis was conducted using R version 4.4.3.
Cox Proportional Hazard Model
The Cox proportional hazards model is a semi-parametric approach to hazard function modeling. It enables the incorporation of covariates while leaving the baseline hazard function unspecified and is constrained to take only positive values. Cox proportional hazards analysis was used to assess the strength and direction of the relationships between predictors and the hazard of Under-Five Children. This regression method was chosen because the data contained missing observations, and its distribution was uncertain. The Cox model allowed for model evaluation without requiring assumptions about the underlying data distribution. 15

Variables were evaluated in unadjusted and adjusted models, and significance was determined at P < .05.
Results
Descriptive Statistics
Table 1 presents the socio-demographic characteristics of under-five children in Somaliland and their survival status at the time of the survey. The majority of children were from the Sanaag (32.2%) and Sool (30.4%) regions, with the highest under-five mortality observed in Woqooyi Galbeed (6.8%) and the lowest in Sool (2.0%). Most children lived in nomadic settings (48.2%), where mortality was higher (3.6%) compared to urban areas (1.4%). Children from households using pipe-borne water had the lowest mortality (1.8%), while those relying on wells had the highest (3.9%). Similarly, mortality was lowest among those with flush toilets (2.9%) and highest among pit latrine users (3.5%). Female-headed households reported lower child mortality (2.1%) compared to male-headed ones (4.3%). Wealth also played a role, with the poorest households experiencing higher mortality (3.8%) than those in middle and higher wealth categories. First-born children had slightly higher mortality (3.8%) than later-born children (2.7%), and female children experienced slightly higher mortality (3.4%) than males (2.4%). Children who were never breastfed had lower mortality (1.7%) compared to those who had been breastfed but were not currently breastfeeding (3.1%). Additionally, under-five mortality was slightly higher among children born to mothers aged 18 or younger (3.0%) and among younger mothers aged 15 to 24 years (3.1%). Overall, the descriptive statistics suggest that under-five mortality in Somaliland is influenced by factors such as region, residence, water and sanitation access, household wealth, and maternal and child characteristics.
Descriptive Statistics of Socio-Demographic Characteristics of Under-Five Children in Somaliland.

Log Rank Test
The log-rank test is used in this study to compare the survival times of children under 5 across different groups. It helps identify significant differences in time to death before fitting the Cox proportional hazards model. This supports the study’s goal of examining the timing and the determinants of under-five mortality in Somaliland.
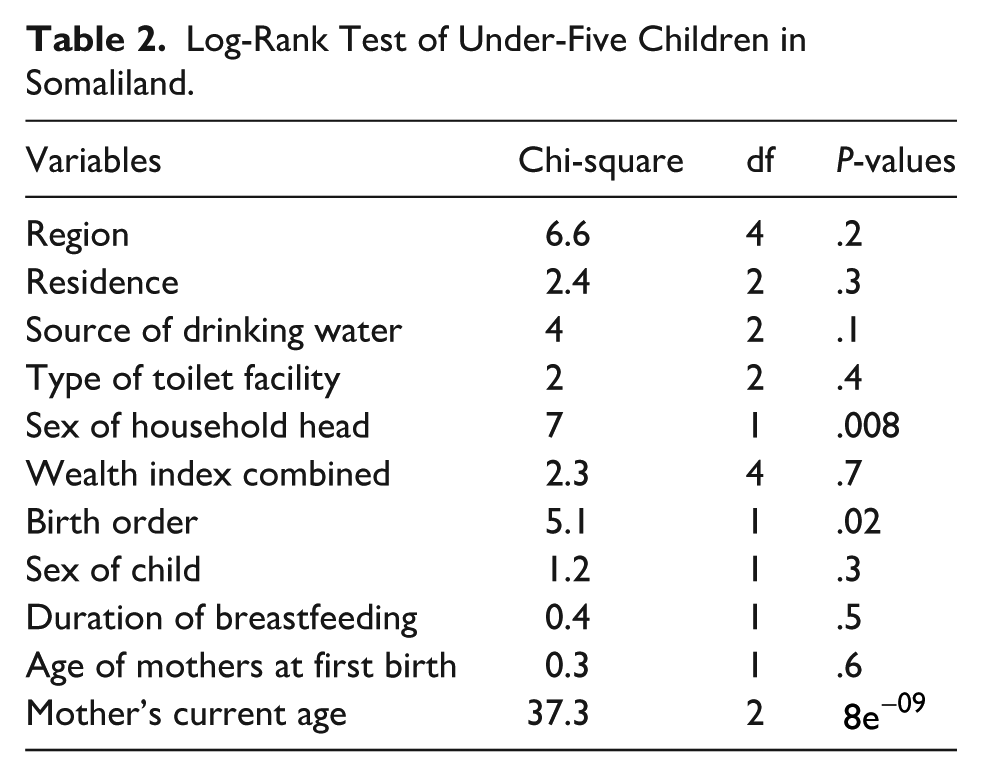
Table 2 presents the results of the log-rank test assessing the association between various socio-demographic variables and the survival time of under-five children in Somaliland. The log-rank test compares survival distributions across different groups, with a significant p-value indicating a statistically meaningful difference in survival times. From the table, sex of the household head (Chi-square = 7.0, P = .008), birth order (Chi-square = 5.1, P = .02), and mother’s current age (Chi-square = 37.3, P < .001) show statistically significant associations with under-five survival, suggesting that these factors influence child mortality. Specifically, children from male-headed households and those with certain birth orders appear to have different survival probabilities, and maternal age plays a highly significant role. On the other hand, variables such as region (P = .2), residence (P = .3), source of drinking water (P = .1), toilet facility (P = .4), wealth index (P = .7), sex of child (P = .3), duration of breastfeeding (P = .5), and age at first birth (P = 0.6) are not statistically significant, indicating that differences in survival time among these groups are not large enough to rule out random chance. this suggests that the sex of the household head, birth order, and maternal age are factors associated with under-five mortality, warranting further investigation in multivariate models like the Cox proportional hazards model.
Log-Rank Test of Under-Five Children in Somaliland.
Cox Proportional Hazard Regression Model
Table 3 presents the results of the Cox Proportional Hazards (PH) model, which examines the determinants of time to death among under-five children in Somaliland. The analysis provides both unadjusted and adjusted hazard ratios (HR), along with their corresponding p-values and 95% confidence intervals (CI), to identify factors significantly associated with child mortality. In Figure 1 the Kaplan-Meier survival curves show significant differences in survival probabilities for under-five children in Somaliland. Some regions, like Woqooyi Galbeed, show higher child mortality rates. Both male and female children have similar survival probabilities, but males have slightly lower survival probabilities at later time points, possibly due to higher health risks. Household water sources also impact survival, with children relying on “Other” sources having slightly lower survival probabilities than those using pipe-borne water or wells. Maternal age also plays a role, with children born to younger mothers having lower survival probabilities compared to those born to older mothers. These results suggest regional disparities in child survival, potential gender-related differences, the importance of clean water access, and the impact of maternal age on child health outcomes. Further statistical analysis could confirm these differences.
Unadjusted and Adjusted Hazard ratios (HR) of the Risk Factors of Corresponding P-values Cox PH Time to Death and Its Determinants of Under-Five Children.

Significant at P-value < .05.
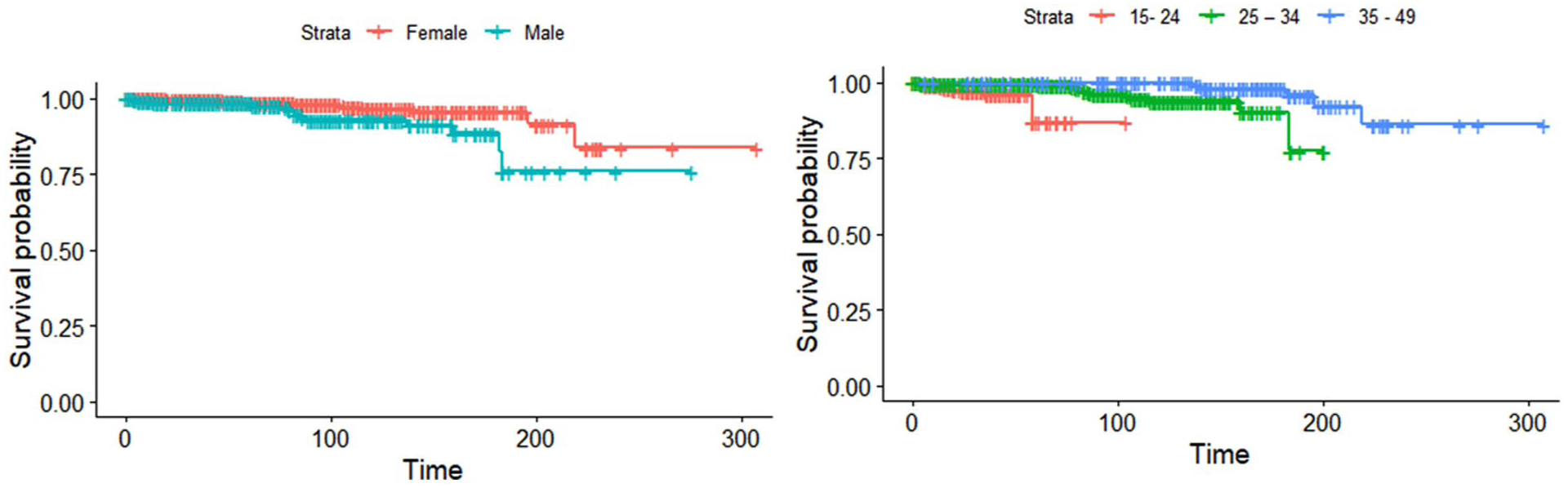
Kaplan Meier plot of regions, sex of household head, source of drinking water, and age of mothers.
Region and Residence do not show statistically significant associations with child mortality in either the unadjusted or adjusted models. However, rural and nomadic residences exhibit higher hazard ratios compared to urban areas, though these differences are not statistically significant (P > .05). This suggests that children in rural and nomadic areas may face higher mortality risks, but the findings are inconclusive. Access to drinking water significantly impacts child mortality. Children relying on wells or other sources (non-pipe-born water) have significantly higher hazard ratios in the adjusted model (HR = 3.96, P = .0336 for wells; HR = 3.31, P = .0163 for other sources) compared to those with access to pipe-born water. This highlights the critical role of safe drinking water in reducing child mortality. The type of toilet facility does not show significant associations with child mortality, except for “other” types of facilities, which have a marginally significant protective effect in the adjusted model (HR = 0.21, P = .0582). This suggests that improved sanitation may contribute to lower mortality, though the evidence is not strong.
Male-headed households are associated with significantly higher child mortality compared to female-headed households in both unadjusted (HR = 2.61, P = .0106) and adjusted models (HR = 2.29, P = .0363). This finding underscores the potential protective role of female-headed households in child survival. Wealth status does not significantly influence child mortality, as none of the wealth quintiles show statistically significant hazard ratios. This suggests that economic status alone may not be a decisive factor in child survival in this context. Children who are second-born or higher have a significantly higher risk of mortality compared to first-born children in the adjusted model (HR = 3.34, P = .0124). This indicates that birth order may play a role in child survival, possibly due to resource allocation or maternal attention.
Female children have a significantly higher risk of mortality compared to male children in the adjusted model (HR = 6.24, P = .0241). This finding highlights potential gender-based disparities in child survival, which may be influenced by cultural or social factors. Never Breastfeeding practices do not show a significant association with child mortality, suggesting that other factors may play a more critical role in survival outcomes. The age of mothers at first birth does not significantly affect child mortality. However, the current age of mothers is a strong predictor of child survival. Mothers aged 25 to 34 and 35 to 49 have significantly lower hazard ratios compared to younger mothers (15-24 years) in both unadjusted and adjusted models (P < .001). This indicates that older mothers may provide better care or have more resources to ensure child survival. The Cox PH model identifies several significant determinants of under-five mortality in Somaliland, including access to safe drinking water, sex of the household head, birth order, sex of the child, and maternal age. These findings highlight the importance of addressing socio-economic, environmental, and cultural factors to reduce child mortality in the region.
Model Diagnostic Cox PH Regression Model
The model diagnostics for the Cox Proportional Hazards (PH) regression, including the Schoenfeld residuals test, assess whether the PH assumption holds for each covariate. In this study, the diagnostics confirm that the effects of predictors on under-five mortality remain constant over time. This ensures the reliability of the Cox model results, directly supporting the study in identifying valid determinants of time to death among under-five children in Somaliland.
Table 4 presents the results of the proportional hazards (PH) assumption test, which is crucial for validating the Cox Proportional Hazards model. The test evaluates whether the hazard ratios for each variable remain constant over time. The results show that the PH assumption holds for all variables, as none of the P-values fall below the .05 significance level. For instance, region, residence, source of drinking water, type of toilet facility, sex of household head, wealth index, birth order, sex of child, age of mothers at first birth, and mothers’ current age all satisfy the PH assumption. The duration of breastfeeding shows a marginal P-value of .053, suggesting a potential but non-significant violation of the assumption. The global test confirms the model’s validity with a chi-square statistic of 22.6370, confirming the hazard ratios are consistent over time. These findings reinforce the reliability of the Cox Proportional Hazards model and the determinants of under-five child mortality identified in Table 3.
Test Proportional Assumption.

Figure 2 shows the Schoenfeld residual plots for some covariates in the Cox proportional hazards model that examines under-five child mortality in Somaliland. These figures are utilized to assess the proportional hazards (PH) assumption for every covariate. Every subplot displays residuals versus time for a given covariate, together with a smoothed trend line and confidence intervals. An important diagnostic in this context is the p-value from the Schoenfeld individual test, which evaluates the null hypothesis that each covariate’s effect remains constant over time, thereby assessing the proportional hazards assumption. This is because all the p-values are greater than the conventional threshold of 0.05. The factors of region (P = .2947), residence (P = .3435), water source (P = .1297), and maternal age at birth (P = .9671) reveal non-significant p-values, suggesting that their effects on the risk of child mortality before the age of 5 are not significantly different across time. The residual plots also contain smooth curves that stay mostly within the confidence limits and do not show systematic patterns, which further confirms the PH assumption. The Cox proportional hazards model is thus appropriate for this analysis, and the covariates considered meet the assumption of proportional hazards.
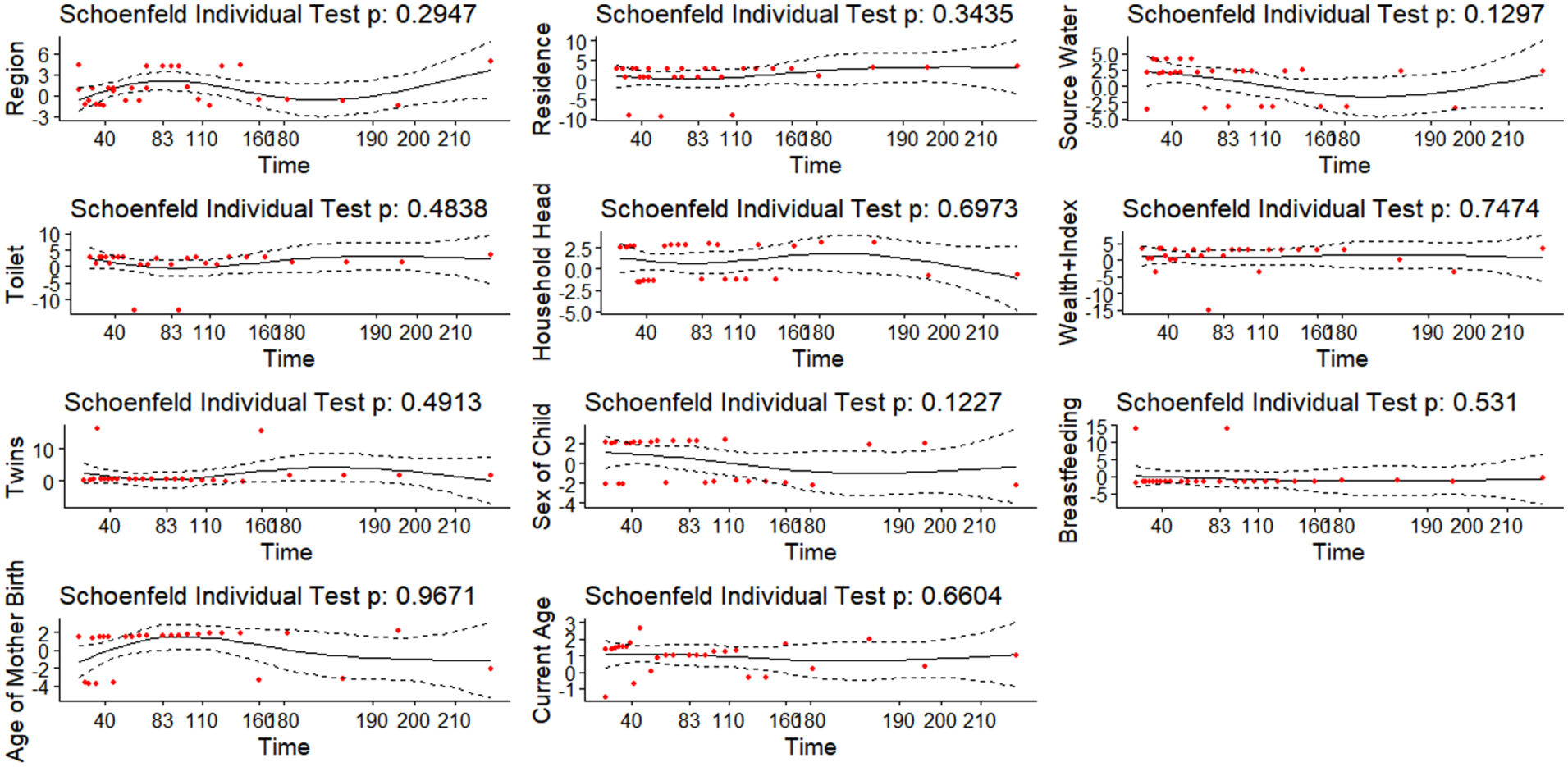
Schoenfeld plot of under-five child mortality in Somaliland.
Discussion
The studies suggest that regional and residential differences in child mortality exist; their statistical significance may vary across contexts and require further investigation to understand underlying determinants. Under-five mortality remains a significant concern in Ethiopia, particularly in rural and less developed regions. Several studies have identified the determinants of child mortality, including family size, preceding birth interval, birth order, breastfeeding status, and source of drinking water.16,17 Longer birth intervals and breastfeeding were associated with reduced mortality risk. Maternal factors such as age at first birth and education level also play a role. 18 Regional disparities were observed, with children in Addis Ababa having a lower mortality risk compared to other regions. Rural residence was associated with a higher mortality risk. 19 Interventions focusing on child spacing, breastfeeding promotion, improving access to safe drinking water, and poverty eradication programs, especially in rural areas, are recommended to reduce under-five mortality. 16 Recent studies on under-five mortality in Ethiopia reveal concerning trends, particularly in pastoral and rural regions. The overall incidence rate of under-five mortality in pastoral areas was found to be 8.4%. 4 The determinants of child mortality include birth interval, breastfeeding status, family size, and geographical region. Children born after longer birth intervals and those who were breastfed had significantly lower mortality risks. Multilevel analyses indicate significant variations in child survival times between regions and households, suggesting unobserved heterogeneities. Rural residence, male children, and poor families were associated with higher mortality risks.17,20 Despite overall improvements, regional disparities persist, with Afar, Somali, and Harari regions showing higher risks. 21 Access to clean water and improved sanitation significantly reduces child mortality and increases life expectancy across multiple studies. Analysis of Demographic and Health Surveys from South Asian countries shows that improved water and sanitation access is associated with lower child mortality, particularly in the post-neonatal period. 22 A global study of 100 countries found that safe drinking water facilities have a stronger impact than sanitation on reducing child mortality and improving life expectancy. 23 These findings underscore the importance of clean water and sanitation in achieving global child mortality reduction goals.
Recent studies have examined the impact of household headship on child health outcomes in low- and middle-income countries. Contrary to the query’s assertion, 24 found no significant differences in immunization coverage or stunting prevalence between male-headed households (MHHs) and female-headed households (FHHs) across 95 countries. Similarly, 25 reported comparable rates of malaria prevention, testing, and positivity among children under 5 in Ghanaian MHHs and FHHs. However, 26 observed that children in Jamaican FHHs received larger resource shares than those in MHHs. 27 found higher odds of childhood anemia in Ghanaian MHHs compared to FHHs. These mixed findings suggest that the relationship between household headship and child health outcomes is complex and may vary depending on the specific context and health indicator examined. Similar studies examining the relationship between household wealth and child mortality in sub-Saharan Africa have yielded mixed results. While some research found a significant association between higher wealth and lower under-five mortality in semi-urban areas of Burkina Faso, 28 others observed no significant effect of wealth on child mortality in rural regions.28,29 A comprehensive analysis across 30 sub-Saharan African countries revealed variations in the joint distribution of wealth and under-five mortality over time. 30 Recent studies have examined the relationship between maternal age and under-five mortality in low- and middle-income countries. However, some studies found that mothers aged 25 to 34 had lower mortality risks compared to younger mothers. 31 These findings highlight the complex relationship between maternal age and child mortality in developing countries.
Conclusion
In conclusion, this study utilized the time to death and its determinants among under-five children in Somaliland using the Cox Proportional Hazards model. The findings highlight several significant socio-demographic factors influencing child survival. Access to clean drinking water emerged as a crucial determinant, with children from households relying on wells or other non-piped water sources facing a significantly higher risk of mortality. Household headship also played a role, with Male-headed households and female children associated with higher mortality risks, highlighting potential gender-based disparities in care and resource allocation. Additionally, birth order and the child’s sex were significant factors, with later-born children and females experiencing higher mortality risks. Maternal characteristics, particularly the mother’s age at the time of the survey, had a strong protective effect against child mortality, indicating that older mothers may provide better care and resources for child survival. Other factors, such as wealth index, residence, and sanitation facilities, did not show statistically significant associations with mortality risk in this study. The test for the proportional hazard assumption confirmed the validity of the Cox model, ensuring the reliability of the estimated hazard ratios. These findings underscore the need for targeted interventions to improve child survival, particularly by enhancing access to clean drinking water, addressing gender disparities in child mortality, and supporting younger mothers with resources to improve child health outcomes. Policymakers and healthcare providers should focus on these critical determinants to reduce under-five mortality and improve child well-being in Somaliland.
Footnotes
Ethical Considerations and Consent for Publication
Author Contributions
A.A.Esse, A.A.Osman : Writing – original draft, Visualization, Software, Resources, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization.A.N.Abdi, M.A. Hussein, A.M.Yousuf, A.H.Muse: Writing – review & editing, Visualization, Software, Resources, Project administration, Methodology, Investigation, Formal analysis, Supervision. All authors reviewed and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.