
Abstract
Background:
Autism Spectrum Disorder (ASD) is a neurodevelopmental condition affecting about 1 in 160 children globally. Caring for children with ASD can be challenging, requiring effective coping strategies.
Objective:
To explore coping strategies and resources used by caregivers of children with ASD in a Ghanaian healthcare setting.
Methods:
A qualitative phenomenological approach with an exploratory descriptive design was used. Ten caregivers of children with ASD at the Greater Accra Regional Hospital’s neurology clinic were purposively selected. Data were collected through semi-structured interviews and analyzed thematically using the ABC-X model of family stress.
Results:
Caregivers mainly adopted emotion-focused coping strategies, such as acceptance, optimism, prayer, and seeking knowledge. These were supported by individual resilience, familial assistance (especially from spouses and siblings), and communal support from religious groups and healthcare providers.
Conclusion:
Caregivers rely heavily on emotion-focused strategies and support systems. Strengthening these supports at individual, familial, and communal levels is essential.
Introduction
Autism Spectrum Disorders (ASDs) are neurodevelopmental conditions characterized by impairments in social interaction, communication, and repetitive behaviors. 1 Globally, ASDs affect tens of millions. 2 Ghana’s estimated prevalence of 38.7% is notably higher than global rates. 3 In contrast to high-income countries, Ghana faces unique challenges in diagnosis, treatment, and care, compounded by misconceptions and limited resources. As ASD typically manifests in early childhood, children often experience functional impairments and maladaptive behaviors, increasing caregiving demands. 4
Caregivers are responsible for managing diagnosis, coordinating healthcare, supporting behavior, and assisting with daily activities. These responsibilities are intensified by comorbid conditions, which further complicate caregiving.5 -7 According to Liu et al, 8 the caregiver burden reflects the multifaceted strain experienced over time, often with negative consequences. This burden can significantly reduce caregivers’ health-related quality of life 9 and impose psychological and financial strains, leading to mental health challenges such as stress, depression, and anxiety.10,11
Contributors to caregiver stress include behavioral management challenges, inadequate professional support, and negative societal attitudes toward ASD. In Ghana, cultural beliefs attributing ASD to spiritual causes result in stigma against both children and their caregivers.4,12,13 Moreover, access to specialized services remains limited, and support systems are often inadequate, worsening caregiver stress.14 -16
As ASD diagnoses rise, more caregivers are at risk of burnout due to the enduring nature of caregiving demands. 17 Caregiving is thus a life-altering experience with far-reaching consequences. To cope, caregivers must adopt effective coping strategies to manage daily and external stressors.18 -20 Coping strategies, as defined by Lazarus and Folkman, 19 involve cognitive and behavioral efforts to manage stress and are critical in alleviating caregiver burden. Taylor and Stanton 21 also described coping resources as referring to the personal, social, and environmental assets individuals use to manage stress. Lazarus and Folkman 19 distinguished between 2 main coping strategies: problem-focused coping, which targets the source of stress, and problem- and implementing strategies to mitigate or eliminate them whereas emotion-focused coping involves managing the emotional responses associated with stressors. 22
Family stress theorists, such as those behind the original and revised ABC-X models, highlight the critical role of individual, familial, and communal resources in managing the demands of caring for a child with a disability.23,24
The ABC-X model, developed by Reuben Hill in the 1940s, is a theoretical framework used to analyze family stress and coping. It posits that a family’s level of crisis (X) results from the interaction between a stressor event (A), the resources available (B), and the family’s perception of the stressor (C).25,26 The model emphasizes that whether a stressor leads to a crisis depends not just on the event itself, but also on the family’s internal strengths and how they interpret the situation. Over time, the model has been refined to include broader social contexts and was later expanded into the Double ABC-X model to better capture the complexity of family stress and resilience.26 -28
Given the multifaceted stressor faced by caregivers of children with ASD,5,29 understanding how caregivers develop resilience is critical to identifying effective support mechanisms, tailoring culturally relevant interventions, and promoting the psychological well-being and long-term coping capacity of families caring for children with ASD. Despite increased awareness of caregiver stress in ASD, limited research has examined culturally specific coping mechanisms in sub-Saharan Africa.
In Ghana, where formal support systems are limited, familial and communal coping resources often play a vital role in managing caregiving stress. However, the literature on coping is predominantly shaped by Western studies,30 -32 which may not adequately capture the lived experiences and cultural contexts of caregivers in low-resource settings. Although some Ghanaian studies have highlighted the challenges encountered by caregivers of children with Autism Spectrum Disorder (ASD),12,13,29 few have applied a structured theoretical framework, such as the ABC-X family stress model, to systematically examine the coping resources and strategies utilized by these caregivers. This has created a significant research gap in understanding context-specific, culturally grounded mechanisms of coping and adaptation in environments marked by limited support and high stigma.
Guided by the ABC-X model, this study aims to explore the individual, familial, and communal coping resources and strategies that caregivers in Ghana employ to manage the complex and ongoing stressors associated with raising children with ASD. By applying this model, the study seeks to generate a theoretically informed and contextually relevant understanding of family resilience in autism caregiving.
Materials and Methods
Theoretical Underpining
The ABC-X model provides a robust theoretical framework for understanding how families respond to stress, making it particularly suitable for exploring the coping resources of family caregivers of individuals with ASD. Caring for a child or family member with autism often involves chronic stress stemming from behavioral challenges, healthcare demands, financial strain, and social isolation.5,29 The ABC-X model offers a comprehensive lens through which to examine these complex dynamics. In particular, the model is valuable for assessing the resources available to families (B), such as emotional support, access to services, financial stability, and family cohesion, which can serve as protective factors that buffer the effects of stress and promote adaptive coping.28,33
Study Design
The study adopted an exploratory, descriptive qualitative design embedded in an interpretative phenomenological paradigm. This approach focuses on analyzing individuals’ lived experiences, aiming to interpret their personal accounts and identify underlying structures within these narratives. 34 This design allowed participants to share their experiences regarding how they navigate the complex and demanding caregiving process for children with ASD. The study was guided by the ABC-X model and its revised form (Double ABC-X model),23,24 which is commonly applied in family crisis research. Specifically, the B component of the model was used to explore the resources available within and outside the family system that caregivers utilize to cope with the challenges of caregiving for children with ASD.
Research Setting
Participants were recruited from the Regional Hospital in the Greater Accra Region of Ghana, a secondary-level public healthcare facility that receives referrals from primary-level healthcare centers within and beyond the region. The hospital’s pediatric department provides specialized services for children from birth to 18 years old and operates clinics dedicated to conditions such as asthma, sickle cell disease, and neurological disorders. The neurology clinic specifically caters to children with cognitive impairments, including cerebral palsy, attention deficit hyperactivity disorder and ASD. The facility is equipped with specialized healthcare professionals, including speech and occupational therapists, to support children with ASD. Additionally, a playroom is available within the pediatric department to create a child-friendly environment. The neurology clinic serves approximately 200 to 250 pediatric patients per month, receiving referrals from the Greater Accra Region and beyond.
Participants and Inclusion Criteria
Participation in this study was restricted to family caregivers who sought care, treatment, or review services for their children diagnosed with ASD at the hospital’s neurology clinic. The inclusion criteria required that caregivers be biological parents or blood relatives of the affected children, with the children being between the ages of 2 and 18 years with a confirmed ASD diagnosis, regardless of severity. Caregivers had to be at least 18 years old at the time of participation. Professional caregivers, facilitators, or non-family members employed to provide care for children with ASD were excluded from the study.
Research Instrument
A semi-structured interview guide was developed to facilitate in-depth discussions with caregivers. The guide was informed by the B-construct/domain of the ABC-X model, ensuring that questions were designed to explore the coping resources available to caregivers within their family and social environments. The questions were targeted at personal adjustment, hopefulness, and efforts to gain knowledge. It also examined the role of faith, family support, and external community help. These questions captured individual, familial, and communal strategies aligned with the “B” component of the ABC-X model. To enhance the reliability of the instrument, a pretesting process was conducted with 3 caregivers at a children’s hospital in the Greater Accra Region. Observations from this pretesting were used to refine the interview guide; however, the pretesting data were not included in the final analysis.
Participant Recruitment and Data Collection Procedure
A purposive sampling technique was used to recruit 15 participants who met the inclusion criteria. Recruitment was conducted on scheduled neurology clinic days. Caregivers of children officially diagnosed with ASD were approached and provided with detailed information about the study, including its purpose, procedures, and ethical considerations. Caregivers who voluntarily agreed to participate signed an informed consent form before inclusion in the study.
All interviews were conducted face-to-face in a private consultation room at the neurology clinic to ensure confidentiality. Each interview lasted approximately 90 minutes. A semi-structured interview guide was used to facilitate discussions. Interviews were audio-recorded with the participant’s consent, and short notes were also taken to capture key insights. Data saturation was achieved by the 15th interview, as no new themes or significant findings emerged beyond this point.
Data Analysis
This study employed Braun and Clarke’s 35 6-step thematic analysis to explore shared coping strategies among caregivers, ensuring depth and credibility. Unlike Interpretative Phenomenological Analysis (IPA), which focuses on individual experiences, thematic analysis was better suited to the study’s goal of identifying common patterns since it emphasizes idiographic, case-by-case interpretation; hence, it was utilized in this study to identify shared patterns across participants. The thematic analysis also allowed for capturing common coping strategies rather than deeply individualized meanings. Six team members (AJ, S-DV, DA, MA, LL, and DW) contributed to the analysis, with AJ and S-DV leading coding, and others reviewing and refining themes. Disagreements were resolved through collaborative discussions to ensure consistency and rigor. In this study, steps were taken to minimize potential biases in the thematic analysis. Multiple coders were involved to reduce researcher and confirmation biases, with regular team discussions and peer debriefing to ensure objective interpretation. Diverse participant voices were represented across themes to avoid selection bias, and findings were carefully contextualized to prevent overgeneralization. Additionally, full transcripts were revisited to ensure accurate interpretation, enhancing the credibility and trustworthiness of the analysis.
Methodological Rigor
Methodological rigor was ensured by addressing all 4 components: credibility, dependability, confirmability, and transferability as outlined by Guba and Lincoln, 36 along with researcher reflexivity. Credibility was established through prolonged engagement, member checking, and verbatim transcription. Dependability was achieved by maintaining a transparent methodology and conducting independent coding reviews. Confirmability was strengthened through an audit trail and reflexive practices to minimize researcher bias. Transferability was supported by providing rich contextual descriptions for applicability to similar settings. Researcher reflexivity was maintained through continuous self-awareness of potential biases and their influence on data collection and interpretation, further enhancing the study’s trustworthiness.
Ethical Issues
The study received ethical approval from the Ethics Review Committee of the Ghana Health Service with approval number - [GHS-ERC 043/06/22]. Permission was obtained from the Director of the Greater Accra Regional Hospital and the Head of the Neurology Clinic before conducting the study. All participants provided written informed consent before participation, including consent for audio recording of the interviews. Interviews were conducted in a private setting, and participants’ identities were kept anonymous by not disclosing their real names.
Findings
Socio-Demographic Characteristics of Participants
We reached saturation upon interviewing the 15th caregiver. All 15 participants were females, direct biological parents of the affected children, married, and within the age range of 31 to 45 years. Out of the 15 participants, 9 had a tertiary level education, and only 6 had a Junior High School (JHS) level of education. Out of the 15 participants, 9 hold formal employment. Out of the 15 children who were diagnosed with ASD, 7 of them were females, whereas the remaining 8 were males. The number of years participants had cared for their children ranged from 2 to 5 years. Ten out of the 15 participants were Christians. The information on the sociodemographic characteristics of the participants is summarized in Table 1.
Socio-demographic characteristics of participants.

Age completed in years.
All respondents were married.
Junior School High.
Themes and Subthemes
Table 2 presents 3 major themes and 6 subthemes. The sub-themes are namely individual or internal, familial, and communal resources, fall under the B component or construct of the ABC-X model.
Themes and sub-themes derived from the study.
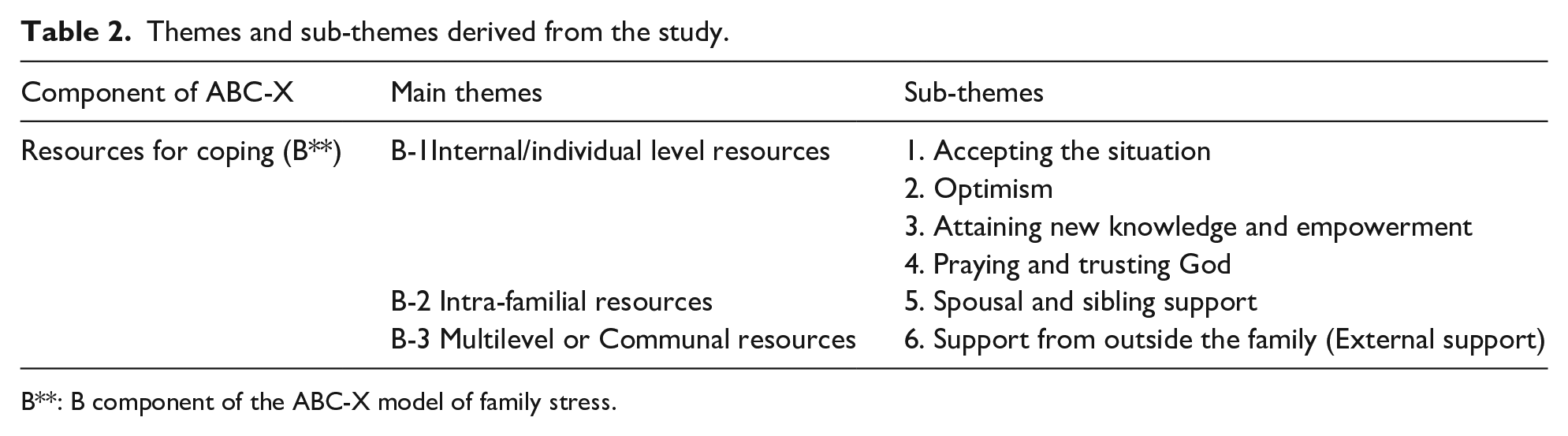
B**: B component of the ABC-X model of family stress.
Resources and Coping Mechanisms Utilized by Caregivers of Children With ASD
According to the participants, the challenges and stressors associated with caring for children with ASD are numerous and occur daily. The behavioral problems, intellectual disabilities, and the need to seek better healthcare and educational services for their children all compound their caregiving responsibilities. As a result, caregivers require coping strategies and resources to manage these challenges and avoid crises. The participants agreed that without such mechanisms, they are more likely to experience burnout, psychological stress, and emotional strain. The coping strategies discussed by the participants primarily focused on how they manage the child’s condition, and the stress associated with it.
B1. Internal/Individual and Psychological Resources
The participants described several individual-level or internal resources that they rely on to cope with the stresses and crises of caregiving. These resources stem from their personal values, belief systems, and spirituality. Among the internal coping mechanisms activated by the participants were accepting the diagnosis of ASD, praying to God, and maintaining optimism about the possibility of improvement.
Accepting the Situation
Initially, the participants experienced denial, struggling to accept that their children had ASD despite the clear signs. This denial affected their ability to seek proper care and services for their children. They expressed feelings of confusion, anxiety, and worry. However, once they came to terms with their children’s diagnosis and accepted the reality of the situation, they experienced a sense of relief and began to hope for positive outcomes. Acceptance of the diagnosis enabled the caregivers to confidently seek solutions, including healthcare services and therapy at the health facility. Below are the accounts shared by some participants:
I did not have peace. I was worried and very anxious. Until I realized that the earlier I accept the situation and move on the better it would be for my child. That was when I stopped being anxious. I have now come to terms with the situation. I have accepted the fact that my child has a challenge and I have found a better treatment to work toward her improvement. I am doing my very best to adhere to all guidelines the hospital has given to us. Both my husband and I started doing that for her.
Optimism
Optimism, being a psychological resource denoting the degree to which an individual generally expects positive experiences in the future, was utilized highly by the participants in this study. The participants reported that they behaved healthily and positively, facing the future with a promising viewpoint. According to them, they have high hopes that their children will improve gain some level of independence and achieve their full potential soon.
I try to find a way to deal with every problem as and when it occurs. I always know and hope that it will be well. My child is improving. I know very soon she would do some of these things by herself. I also know she would be able to read and behave just like her peers. I heard her saying a few words to her brother. The therapist also said she is improving with her speech. I have the hope that very soon he would engage us in conversation and tell us all that is on her mind and what she feels about things around her.
Attaining New Knowledge and Empowerment
According to the participants, not knowing much about ASD and its manifestations contributed to their stress. To be able to cope, they relied on information from health service providers, to equip themselves to play the caregiving role with minimal stress and difficulties. Others relied on self-teaching strategies by getting information from medical and social literature sources. All these helped them to develop skills and strategies to reduce the burden of caregiving and also provide the needed care for their children with ASD. It was observed that attaining knowledge about the condition of ASD put some caregivers in a better position to handle their children.
Initially, I was lost. I didn’t know what this disease was and what I should expect. I then decided to search, learn and teach myself better ways to handle my child. . … Reading a lot, was what I did. I had to do a lot of research on the issue and that is how I coped They invited all of us who were at the clinic that day to participate in that program. The therapists taught us a lot of things. I learned simple ways to handle him. It’s been working well for me. It was very good I was part of that program. It gave me a lot of insight.
Prayer and Trusting in God
Prayer, which is known to be an emotion-focused strategy, according to the participants, is the way to connect to God. It helps them to demonstrate faith in their God. Caregivers in this present study mentioned that prayer helps them to get relief, usually in times of anxiety, fear, and worry. They resort to praying and believing in God to overcome and manage the challenges associated with caring for their children with ASD.
Sometimes it is only prayer that helps. Nothing else. I always put my trust in God. For that one I pray, there is no other way out, I just pray and have faith that it will be well I also pray with him and he has become used to it, I pray with him every time and I know God will hear our prayer Prayer helped to overcome the fear and worry. I have the better inner strength to care for him My reverend father assists in prayers and tells me what to do,
B2. Intra-Familial Resources
The family is the first environment of socialization of the child with ASD and the primary context of their care, having the potential to meet their needs, to support and promote their developmental potential. According to participants in this study, the support from all other members of the family makes the caregiving burden a little bit lighter on the mothers who are the main care providers in the family.
Spousal and Sibling Support
The participants mentioned support from their spouses and other siblings of children with ASD.
Both my husband and I started doing that for him. We have been in this task together, right from the time our child was diagnosed. My husband has learned to calm him down better than I ever do. As a family, we received the diagnosis without knowing about it and not knowing what to do. With time, we have all accepted and loved him like any other member of this family. His brothers are always around him, teaching him to read and even paint. Because everyone in the family is willing to assist in doing something for him, the stress is not so much on me as the mother of this house.
In some cases, caregivers with children with ASD are left without any family support. One participant mentioned that the absence of support from close family members makes her feel lonely and helpless. According to her, the burden becomes too heavy, and that affects the care she provides for her child.
I always wished that my child did not have this problem,. . .. I am all alone in this. I feel helpless and lonely. No one is there to help. Sometimes I just watch her. not being able to help her.
B3. Multi-Level or Communal Support
According to participants of this study, social support systems involve a network of people, friends, and peers that one can turn to for emotional and practical support. Most of the participants in this study made use of these social networks to cope with caregiving difficulties.
Support From Outside the Family (External Support)
Participants disclosed that they received strong support from religious leaders, friends, professionals or specialists, and healthcare workers who were involved in the care of their children. These supports came in the form of words of encouragement, sympathy, prayer, and professional advice.
My pastor and friends at the church keep assuring me that the child will be well. I am also in the charismatic group of my church. The members have always sympathised with me and encouraged me to believe in God. They always pray with us The therapist and the nurses call to check on him from time to time. They encouraged me not to miss the appointments. They said they are hoping for improvement, so I should not be discouraged.
Discussion
This exploratory study investigated the coping resources and strategies utilized by caregivers of children diagnosed with ASD. Fifteen (15) caregivers who sought treatment, review, and specialist services for their children at the Neurology Department of the Regional Hospital in the Greater Accra Region were interviewed. The study aimed to understand the resources caregivers rely on to navigate the challenges associated with their caregiving responsibilities.
Caregivers of children with ASD dedicate significant time and effort to support their children, assuming primary responsibility for essential daily tasks such as toileting, dressing, feeding, therapy, and transportation to medical appointments. 29 Their role as primary caregivers is both physically and emotionally demanding, often requiring continuous, round-the-clock care without respite. 29 The absence of strong support systems further exacerbates this burden, increasing the risk of emotional and physical burnout. 17
Findings from this study indicate that caregivers predominantly relied on emotion-focused coping strategies to manage the challenges associated with their caregiving roles. As described by Saya, 37 emotion-focused coping involves regulating emotional responses to stressors rather than directly addressing the source of the stress. Previous studies have also demonstrated that individuals facing significant stressors frequently adopt emotion-focused coping strategies.31,38 In alignment with the ABC-X model proposed by family stress theorists,24,39 caregivers in this study employed coping mechanisms at the individual, familial, and communal levels.
Individual-Level Coping Strategies
At the individual level, acceptance emerged as a common coping mechanism. Many caregivers reported having come to terms with their children’s diagnosis, acknowledging and accepting their reality. This finding is consistent with prior research, including a systematic review by Al-Oran et al 38 and an exploratory study by Luong et al, 40 both of which identified acceptance as a frequently used coping strategy among caregivers of children with ASD.
Another key emotion-focused strategy identified in this study was prayer and faith in God. Participants reported that engaging in prayer provided relief from stress, anxiety, and worry, helping them cope with the emotional burden of caregiving. This aligns with previous findings that religious engagement and positive attitudes toward faith contribute to personal well-being, improved health outcomes, and reduced distress.41,42 Similarly, a systematic review by Al-Oran et al 38 highlighted prayer as a widely utilized coping strategy among caregivers of children with ASD. Religious coping, particularly private religious practices such as prayer, is among the most common strategies for managing caregiving-related stress and crises 43
Optimism also played a crucial role in caregivers’ coping strategies. Participants expressed hope that their children’s conditions would improve, particularly in terms of speech and intellectual abilities. Optimism has been identified in previous research as a key coping mechanism among caregivers of children with ASD. 44 Optimistic individuals tend to confront challenges proactively, utilizing both problem-focused and emotion-focused coping strategies to manage crises. 45 Moreover, optimism has been shown to positively influence psychological and physical well-being, life satisfaction, and overall health. 46 Additionally, caregivers actively sought knowledge and information about ASD, demonstrating a proactive approach to caregiving. Many caregivers have turned to therapists, healthcare professionals, and online resources to better understand the condition and improve their caregiving strategies. Access to reliable information not only reduces caregivers’ sense of powerlessness but also equips them with effective strategies to foster their children’s development.
This finding is consistent with a study conducted among Malaysian caregivers, which found that caregivers sought knowledge from various sources to enhance their ability to care for their children. 47 However, the Malaysian study revealed a combination of emotion-focused strategies like prayer and acceptance with practical, problem-focused support from employers, and the community. This highlights a more diverse and multi-level coping system beyond the individual and familial levels.
Familial and Communal Support
In addition to individual-level coping mechanisms, caregivers in this study benefited from familial and communal support systems. Participants reported receiving support from spouses, siblings of the affected child, peers, religious leaders, and healthcare professionals. These findings are in line with prior research demonstrating that caregivers of children with ASD rely on external support to manage stress. 48 Social support plays a critical role in building resilience, offering strength during stressful periods, and fostering overall well-being. 49 Studies have established a strong link between social relationships and various aspects of health and wellness among caregivers of children with ASD. For instance, Bishop-Fitzpatrick et al 50 found that social and external support positively impact the overall quality of life for families of children with ASD. Similarly, McGrew and Keyes 22 highlighted that strong support systems can buffer stress, reduce caregiving burdens, lower depression levels, and enhance overall caregiver health. In this study, all caregivers were women; this aligns with a similar study in Ghana, where 97% of caregivers were women. 51 In Ghana, cultural norms assign caregiving roles primarily to women, which explains the absence of fathers in this study. Although not present at the hospital, fathers were reported to provide support at home, and this was reported as familial support by the participants.
The study found that caregiving support mainly came from the nuclear family, highlighting a shift from extended to nuclear family structure in Ghana. 52 While the extended family remains important for major life events, it is now less involved in daily caregiving, explaining the greater support reported from spouses and siblings compared to the extended family. This study found limited evidence of community-level support for families of children with ASD. This is likely due to the deep stigma surrounding ASD in Ghana. The condition is often misunderstood and linked to spiritual or supernatural causes, such as curses or ancestral punishment,12,13 leading to social isolation and limited public support. 29 To avoid discrimination, many families keep the diagnosis private, which further limits community involvement in caregiving. The participants reported that the nurses and therapists were cordial, offered emotional support and encouraged them to adhere to treatment and appointments. This finding reflects the essential role played by nursing and other professionals in providing comprehensive and effective care for children with ASD and their families 53
The study mainly reported positive coping strategies, which may reflect social desirability bias. Given the strong stigma surrounding ASD in Ghana,12,13 participants may have emphasized inner strengths while withholding negative caregiving experiences. This limitation is noted in the discussion. Future research should create safe spaces to elicit more balanced narratives.
Aligning the Study’s Findings with the ABC-X Model
Caregivers of children with ASD draw on a range of coping resources that align with the “B” component of the ABC-X model, which emphasizes the role of resources in managing family stress. At the individual level, caregivers rely on personal strengths such as acceptance, optimism, self-empowerment through knowledge, and spiritual coping, all of which shape their perception of stress and promote resilience. Intra-familial resources, particularly support from spouses and siblings, provide emotional and practical assistance, enhancing the family’s capacity to adapt. At the communal level, external support from extended family, neighbors, religious groups, and organizations further strengthens caregivers’ coping mechanisms. Collectively, these multilevel resources interact with caregivers’ perceptions (C) and help determine whether the caregiving stressor (A) leads to crisis (X) or successful adaptation, highlighting the importance of contextually grounded support systems in resource-limited settings like Ghana.
Limitations of the Study
The study is limited by the inclusion of only caregivers who were engaged with the healthcare system, potentially excluding those who face greater barriers and rely solely on informal support. As a result, the findings may not reflect the full range of coping experiences among all caregivers of children with ASD. Additionally, the study was conducted at a single healthcare facility in southern Ghana. This setting may not represent the diverse cultural and resource contexts across the country. Extending recruitment to cover smaller clinics and rural settings is recommended. This study revealed limited sample diversity, primarily involving married women and biological mothers. (limited number of fathers, single mothers, etc.) The study also could not assess how factors such as educational status, the child’s age, and disease severity influence caregivers’ coping strategies. Future mixed methods research is recommended to explore how a broader range of sociodemographic characteristics shapes coping mechanisms among diverse caregiver populations. Social desirability bias may also have influenced the findings due to the application of face-to-face interactions.
Conclusion
The study concludes that caregivers of children with Autism Spectrum Disorder (ASD) in southern Ghana predominantly rely on emotion-focused coping strategies such as acceptance, optimism, prayer, and seeking knowledge to manage the challenges of caregiving. These strategies are primarily supported by individual, familial, and communal resources, aligning with the ABC-X model of family stress and coping. Despite limited formal support systems, caregivers draw strength from internal resilience, family involvement, and community networks to navigate their caregiving roles. The findings highlight the critical need to strengthen support structures and promote culturally relevant interventions to enhance caregiver well-being.
Footnotes
Acknowledgements
We acknowledge the staff of Greater Accra Regional Hospital. We also express our special thanks to all the caregivers who voluntarily participated in this study.
Ethical Considerations
The study received ethical approval from the Ethics Review Committee of the Ghana Health Service. (Approval Number: GHS-ERC 043/06/22). Permission was obtained from the Director of the Greater Accra Regional Hospital and the Head of the Neurology Clinic before conducting the study. All participants provided written informed consent before participation, including consent for audio recording of the interviews. Interviews were conducted in a private setting, and participants’ identities were kept anonymous by not disclosing their real names.
Author Contributions
Appah J., Conceptualization, Methodology, Data collection, Data Analysis; Senoo-Dogbey V.E, Methodology, Supervision, Writing-Original draft preparation, Writing-Reviewing & Editing. Wuaku D.A., A.D & L.L., Supervision, Writing- original draft, Writing-Editingand reviewing. All authors contributed to the article and approved the submitted version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data for this study is available from the corresponding author upon reasonable request.