
Abstract
Objectives. Important factor in caring for ASD patients is the successful cooperation between the physician and the parent. Methods. The online survey has been conducted. For statistical analysis the t-student test and the U-Mann Whitney test were performed to compare 2 variables, then the Kruskal-Wallis test or ANOVA as well as The Pearson correlation and Sperman’s rank correlation were performed. Results. 80.5% of respondent’s PHPs did not notice the child’s developmental difficulties. 22.02% of respondents can speak to their PHP about a child’s difficulties. PHPs take different strategies to make patient contact with the healthcare system easier. We discovered statistically significant differences in the assessment of PHPs’ abilities depending on the physicians’ specialty, the children’s age, the age at ASD diagnosis. Conclusion. The care for autistic patients provided by Polish PHPs is insufficient and the topic needs to be addressed immediately.
Introduction
Autism Spectrum Disorder (hereafter referred to as “ASD”) is a heterogenous, lifelong neurodevelopmental condition which prevalence is steadily increasing now. Since 1943, when Leo Kanner published the first description of children with autism spectrum, 1 the understanding of ASD pathogenesis and knowledge of complex etiology have evolved leading to conclusions that many factors such as genetic, epigenetic, metabolic, hormonal, immunological, or neurophysiological contribute to autistic phenotype. 2 The process of understanding has been reflected by changes in diagnostic criteria in both: DSM and ICD classifications.3-5
ICD-11, the classification that is currently implemented into Polish medical practice, focuses on 2 core criteria for ASD. To receive an autism spectrum diagnosis according to ICD-11, an individual’s behavior needs to be characterized by (1) “persistent deficits in the ability to initiate and sustain reciprocal social interaction and social communication” and (2) “a range of restricted, repetitive, and inflexible patterns of behavior, interests or activities that are clearly atypical or excessive for the individual’s age and sociocultural context.” The additional criterion that the patient must meet is the impact of symptoms on personal, family, social, educational, occupational, or other important areas of functioning. 6 In ICD-11 it is recognized and highlighted that some individuals with ASD may start experiencing distress or difficulties in social situations in adolescence or adulthood when social demands increase. 7 Even though first symptoms of autism such as poor eye contact, difficulties in social responsiveness, or repetitive behaviors may be noticed even in infants or toddlers, the mean age of ASD recognition globally has been estimated as 43 months. 8 One of the reasons for the delay may be the fact that the autism spectrum assessment is a complex process that involves the usage of standardized, specialized tools, and should be led by experienced clinicians with a special interest in neurodevelopmental disorders. 9
The prevalence of autism spectrum disorder is steadily increasing around the world according to research performed in different parts of the globe. In USA 1:36 8-year-olds are recognized with ASD. 10 In 2020, Sacco et al 11 performed the literature review on autism prevalence in 9 European countries showing the rate between 0.3% and 2.7% for different places. 11 Due to the lack of a coherent autistic database in Poland, the prevalence of ASD in the country remains unknown. Although in one research performed in 2017 in the Pomeranian region of Poland the prevalence was estimated as 0.3%, the conclusion led to the statement that more investigation is needed. 12 It may result from both: under-diagnosis and under-reporting of ASD in Poland. 13
Early diagnosis of ASD and effective, comprehensive care for autistic patients and their families including evidence-based therapies and complex focus on the whole family system remains the main factors contributing not only to the improvement of patient’s well-being, cognitive, and social abilities 14 but also to reducing parental stress level and, in consequence, to better family system functioning.15,16 The complex care also needs to cover the diagnosis and effective treatment of physical and mental comorbidity, including the higher rate of intellectual disability, depressive and anxiety disorder, obsessive-compulsive disorder, ADHD, gastrointestinal issues, and epilepsy in comparison to the non-ASD population.17-19 Due to the mentioned reasons, the primary healthcare providers are perfectly positioned to meet the complex needs during regular checkups or additionally arranged pediatric visits to perform screening tests for autism, settle current needs for assessment or support, organize tests for comorbidity or discuss caregivers’ or family needs. 20 Such an attitude toward the complexity of care for autistic patients meets many barriers. 21 The most important factors to be highlighted are the poor access to primary healthcare, 22 the shortage of physician knowledge, 23 and the family or individual knowledge limitations 24 or stigma preventing autistic individuals and the members of their families from engaging with the healthcare system. 25
In the process of complex care for autistic patients, one of the most crucial factors is parental well-being and the effective cooperation between caregivers and specialists including primary healthcare physicians. Unaddressed parental needs may result in disengagement from treatment and poor treatment outcomes for the child. 26 Moreover, the cooperation between caregivers and physicians should be consolidated starting from the prevention stage. Research indicates that early prevention can limit the negative impact of ASD-related symptoms and difficulties on chosen somatic complications such as dental problems. 27 This is one of the reasons why the relationship between caregivers of ASD individuals and physicians as well as the parental view on primary healthcare specialists should be assessed and improved.
To assess the level of comprehensive care for autistic children provided by Polish Primary Healthcare Physicians in parental view the online survey has been prepared. The research covered 3 aspects of comprehensive care for ASD individuals in the Polish primary healthcare setting: the physicians’ competencies to diagnose autism spectrum disorder and comorbidity, as well as the competencies to support different aspects of child support. The third aim was to assess the strategies undertaken by primary healthcare physicians to make the contact with healthcare system easier and more accessible for autistic individuals and their families.
Materials
The survey was performed based on 159 anonymous answers to the online questionnaire originally designed by the research authors by means of Google Forms. To collect sufficient data from different regions of the country the online method was chosen.
The study group consisted of autistic individuals’ caregivers—147 female and 12 male. Participants came from different kinds of living places—villages (28.93%), towns with up to 20 000 inhabitants (23.27%), towns with 20 000 up to 100 000 inhabitants (16.98%), and cities with more than 100 000 inhabitants (30.82%). Among the participants’ children, there were 132 boys and 27 girls. The physicians who take care of participants’ children were divided into 2 cohorts—the pediatricians and the general practitioners. The demographic characteristics of the participants are presented in the Table 1 below.
Demographic Characteristics of the Participants.

Methods
This was a survey study with the use of a custom, ad hoc questionnaire consisting of 18 multiple-choice questions. For the purpose of this study, an online survey was prepared. ICD-11 criteria as well as the knowledge of ASD diagnosis and comorbidity relevant to the Primary Healthcare Physicians were taken under consideration. The members of associations consisting of autistic adults and parents of autistic children and adolescents received the first draft of the questionnaire and were asked for feedback. Based on their suggestions, the items about specific strategies taken by physicians were added.
In the first part of the survey, the demographic characteristics were collected: parents’ data including their gender, age, and the living place, children data including their sex, current age, and the age of the ASD diagnosis (the time from the ASD diagnosis was also counted based on provided data), formal diagnosis (referring to ICD-10 which is still formal diagnostic classification in Poland to be replaced by ICD-11 in nearest future) and comorbidity as well as physicians data focusing on their specialty and time they have the child under supervision. For the second part of the survey, based on a literature review, the original questionnaire was designed. The questionnaire consisted of 18 items divided into 4 categories to assess the level of complex care for autistic individuals provided by primary healthcare physicians in parental view (marked as “DIAGNOSIS,” “SUPPORT,” “STRATEGIES,” and “GENERAL”). The “diagnosis” category (items 1-5) referred to the physicians’ ability to notice alarming autistic symptoms 28 , using the proper screening measures (such as M-CHAT-R/F) 29 and advising parents on further diagnostic procedures as well as diagnosing comorbidity. 30 The “support” category (items 7; 9-12) focuses on the assessment of the physician’s ability to support the family in the process of lifelong therapy and regular evaluation consisting of questions referred to collecting psychological documents, advising on new forms of therapy and discussing child’s current behavioral and social difficulties as well as family needs. 31 The “strategy” category (items 13-17) focused on practice behavior used by physicians to make contact with the medical system easier for autistic individuals and their families. The strategies included seeing the autistic patient by the same doctor, as well as seeing the patient on time, adjusting the sensory environment to the individual’s needs, and explaining the performed procedure to the patient.32-34 The “general” category consisted of 3 statements (items: 6, 8, 18). To assess the level of comprehensive care for autistic patients the original 0 to 3 points coding algorithm was suggested, where 3 means the physicians’ behavior or strategies highly contributing to child and family support and 0 means an inadequate level of support in the category. The points were summed up in 3 particular categories as well as in general (counting all 18 items). The statements are divided into categories and the specific coding algorithms are listed in the table below (Table 2). The questionnaire used in the study was not validated.
Original Questionnaire With Coding Algorithm.

The online questionnaires were collected between October 4, 2023 and October 19, 2023 (The form was active for 16 days). The link to the survey was sent to parents of autistic individuals directly, as well as to the centers and institutions taking care of ASD families daily. The link was also presented on the Facebook groups gathering parents of autistic children. Due to the wide accessibility to the link, the response rate is unknown.
The inclusion criteria were being a parent of at least 1 autistic child (regardless of the parental and child’s age), speaking Polish (the questionnaire was prepared in Polish), and having any experience with the Polish Primary Healthcare System. We gathered 167 questionnaires of which 8 uncompleted forms were excluded.
Statistical Analysis
From the first part of the survey, demographic characteristics are exposed in Table 1. Data are presented as counts, percentages, and (for the age of participants and their children) mean, median, and range. From the second part of the survey, the percentage distribution of possible answers is shown in Table 3. The answers were subsequently coded as mentioned in Table 2, the results were summed up in particular categories as well as in general and presented as mean, percentages of the maximum possible score, standard deviation, and range for all participants and different kinds of chosen variables (Tables 4-6). Percentage rates of maximum possible scores in general and in particular categories were used to compare the results among categories and to verify the parental assessment of the Primary Healthcare Physicians’ (PHPs) abilities to take comprehensive care for autistic children and their families. For the statistical analysis, the normal distribution was excluded for all data except for parental age based on the Shapiro-Wilk test. To verify the comparison of variables, the t-student test (for normally distributed data) and the U-Mann Whitney test were performed for 2 variables (Table 5) and the Kruskal-Wallis test or ANOVA for multiple independent samples (Table 6). The Pearson correlation and Sperman’s rank correlation were verified for chosen data with and without normal distribution respectively (Table 7). The threshold of statistical significance was set at P < .05. The statistical analysis has been performed using StatPlus v.8.
The Distribution of Answers for the Questionnaire Among All Participants.

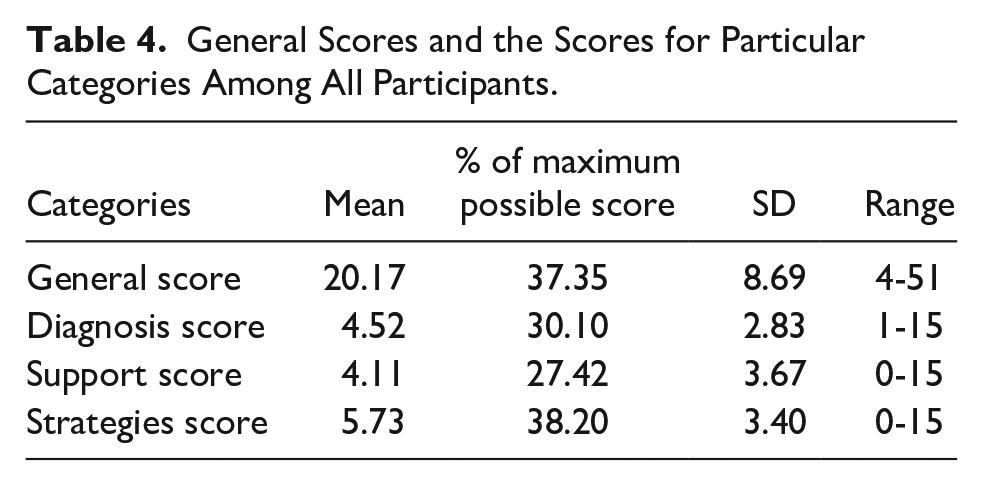
General Scores and the Scores for Particular Categories Among All Participants.
The Assessment of PHPs Comprehensive Care Depending on Chosen Variables.

The General Score of the Questionnaire Depending on Children’s Diagnosis.

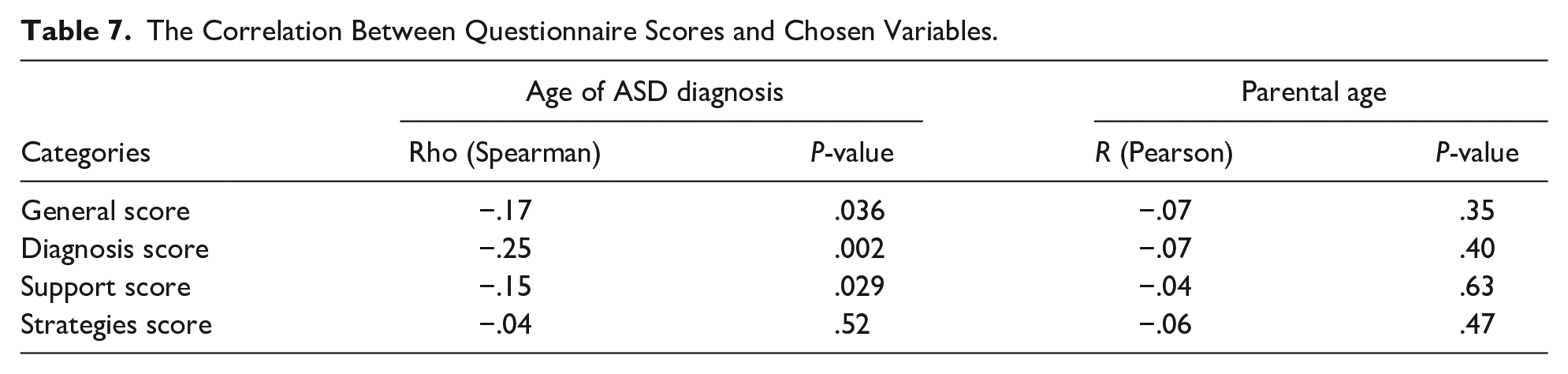
The Correlation Between Questionnaire Scores and Chosen Variables.
Ethical Approval and Informed Consent
Ethical approval was obtained from the Bioethical Committee at the Medical University of Gdansk (the approval number: KB 511/2023) which complies with the Helsinki Declaration. Written informed consent was taken at the beginning of the questionnaire from all participants. Every participant could read the aim of the study as well as was informed about the anonymity of the questionnaire. There was also the possibility to withdraw the answers at any time during the questionnaires collection.
Results
In total, 159 parents of autistic children took part in the survey with the vast majority of female respondents (92.45%). The mean age of parents was 39.09 (26-60). The majority of participants’ children were male, with a mean age of 8.4 (2-19). Most children were diagnosed with childhood autism (55.35%) and had at least 1 additional diagnosis (71.07%). The primary healthcare physicians taking care of participants’ children were pediatricians and general practitioners (69.81% and 30.19% respectively). All demographic characteristics are presented in Table 1.
Table 3 presents the distribution of answers to the questionnaire among all participants.
Most of the respondents claimed that PHP did not notice the child’s developmental difficulties as the first specialist (80.5%) with 44.02% of them stating PHP downplayed the symptoms parents had noticed. Less than 10% of respondents’ children (7.55%) had autism screening tests performed by PHP. When respondents’ children were suspected of autism spectrum disorder, 25% of PHPs were able to advise parents on the further diagnostic procedure and 18.87% of them started the diagnostic process on comorbidity. 25.79% claim that their PHP has sufficient knowledge of diagnosis, therapy, and comprehensive care for autistic patients. Most PHPs have access to children’s psychological and educational documentation (61.01%). From a parental perspective, only 10% of PHPs feels anxious in contact with autistic patients on every or most appointments.
Most PHPs do not discuss children’s and families’ difficulties daily. Only 22.02% of respondents can speak to their PHP about a child’s social and behavioral difficulties on most appointments. Most of participants’ PHPs never speak to them about the current support and therapies the child takes part in (56.60%) or about new methods of therapies (76.73%) as well as about difficulties experienced by the whole family system (77.36%).
Different strategies are taken by PHPs to make the contact with healthcare system easier for autistic patients and their families. Around 75% of children are seen by the same PHP on most appointments. 40.25% of children are seen by PHPs on time with only 10% of children seen as the first patient of the day. 71.70% of participants claim that PHPs never adjust the sensory environment to a child’s needs and 51% answer that the elements of physical examination are explained to the children by PHPs. 88.68% of respondents believe that PHPs address the children with respect on every or most appointments.
All participants’ answers—after scoring and summing up—revealed that the general assessment of the comprehensive care for autistic children by the PHPs is insufficient with the level of 37.35% of the maximum possible score. Among the particular categories, the highest score is for strategies taken by PHPs (38.20%). The diagnostic abilities, as well as support initiatives, are rated on the level of 30.10% and 27.42% respectively (Table 4).
There is a statistically significant difference between the assessment of diagnostic abilities of general practitioners and pediatricians (scores 5.96 vs 3.89, P < .001) with the higher score for general practitioners and with no differences for the rest of the categories (Table 5). The parents of younger children (2-6years old) perceive the PHPs significantly better in general (the scores on the level of 22.59 vs 18.78, P = .03), as well as in the diagnostic field (scores 5.62 vs 3.88, P = .02) than parents of older children. There is also a statistically significant difference in perceiving PHPs’ diagnostic abilities depending on the period children spent under the physician care (higher score for the abilities of PHPs looking for the children for less than 5 years—scores on the level of 5.38 vs 3.78 respectively, P < .001). There is also a significant negative correlation between the age of ASD diagnosis and the scores for diagnosis and support categories as well as general perception (Table 7).
We did not find statistically significant differences between general and particular scores for the parents and children’s gender, the place family lives or children’s comorbidity (Table 5) as well as the children’s specific diagnosis (Table 6). There is no support of correlation between the questionnaire’s results and parental age (Table 7).
Discussion
Demographic Data
The demographic characteristics presented in Table 1 shows the majority of females taking part in the survey. The proportion results probably from the higher involvement of mothers in taking care of autistic children, what finds the confirmation in the literature review.35,36 There is also the majority of male autistic children in the study mirroring the general trend in the proportion of autistic boys and girls worldwide 37 resulting from the underestimation of female autism and the camouflage effect rather than from true disproportion. 38 In the study, similarly to other research, 39 almost 3 in 4 children have additional diagnosis which makes the issue of taking care of autistic patients even more complicated and complex. The structure of physicians indicated in the study is parallel to the general trend of replacing pediatricians with general practitioners whose involvement in taking care of the pediatric population is growing nowadays in Poland in primary healthcare settings.
Effective Diagnosis and Support of Autistic Patients
The topic of autism diagnosis seems to be one of the most important challenges in the primary healthcare settings. No reliable data are indicating the age of ASD recognition among Polish children, however, in current study, the mean age of the diagnosis reaches 55 months and is significantly higher than global data stating 43 months as the average age of recognition. 8 Moreover, the early signs of autism may be present in infants 40 what makes the window between the first signs and definite diagnosis even more urgent topic.
In the current study, the significant majority of PHPs were not the first specialist noticing early autism signs. Almost half of participants claimed that PHPs downplayed the symptoms that were indicated by parents. Such attitude can contribute to diagnostic delays and increase parental frustration with healthcare system and decrease the level of trust in PHPs. 41
There are reliable tools, such as M-CHAT-R/F that are recommended in early autism screening in children between 16 and 30 months by the American Academy of Pediatrics. 42 Unfortunately, there are no official Polish recommendations on the early screening for ASD, even though the tool is accessible for free and performing the M-CHAT-R/F protocol engages little or no physician’s attention as the paper is intended to be filled by parents themselves. Nevertheless, in the current study, early autism screening was performed in only a few cases. The reason, according to research among Polish primary healthcare physicians, may lie in the lack of primary healthcare physicians in Poland and the overload of physicians’ offices during the infectious season. 43
The complexity of care demands also knowledge on further steps in the autism diagnosis, not only the screening process. Among participants, only a quarter of them felt satisfied with the advice given by PHP on the diagnostic process. The complexity of the autism diagnostic path involving not only medical examination but also a few psychological and educational steps differing based on variables such as age and the intensity of child’s symptoms may cause misunderstanding among specialists who are not involved in the ASD assessment on a daily basis, PHPs among them. 44 The lack of understanding may be deepened by the comorbidity such as ADHD, OCD, or other psychiatric conditions making a heterogenous clinical presentation of autistic patients even more challenging. 45
The general practitioners’ diagnostic abilities were assessed significantly higher in comparison with pediatricians. In Poland, GPs are usually doctors who work only in primary healthcare settings and are specifically dedicated to recognizing early signs of disorders and difficulties whereas pediatricians often work in General Practice part-time combining it with working in a hospital environment.
There is also a correlation between the higher level of PHPs’ abilities assessment and the younger age of the ASD diagnosis. The phenomenon may result from the unambiguity of symptoms in early childhood that are difficult to be underestimated and downplayed by specialists. It leads to the early reaction of parents and physicians, faster recognition of autism, and, in consequence, better cooperation between caregiver and doctor when both are consistent in seeing alarming symptoms and compatible in reaction.
The early diagnosis of autism and comorbidity seems to be the beginning of the complicated, complex process of taking care of the autistic patient on a daily basis. The assessment of the PHPs’ abilities to support the children with autism and their families is very severe in parental view. The parents feel mostly unsatisfied with the level of support provided by primary healthcare physicians in terms of discussing actual problems other than medical conditions, such as educational support, new forms of therapy, or the family’s well-being. While the diagnostic abilities may be based on clinicians’ experience and the fact they assess many children with different kinds of developmental difficulties on a daily basis, the ability to support the whole family system demands specific knowledge and particular skills. It seems to be related to the poor assessment of PHPs’ knowledge of ASD in the parental perspective. Only 1 in 4 caregivers believe their physicians know enough about autism. There is only one Polish research assessing pediatricians’ knowledge about autism that revealed inadequacy in the topic that may result from poor undergraduate and postgraduate education of PHPs. 46
The Assessment of Support Strategies
Some of the possible strategies aiming to reduce the frustration of autistic patients and their families in contact with healthcare systems result from the specificity of autistic symptoms whereas other are associated with general specifics of working with children and adolescents. Undoubtedly, autistic patients have difficulties with sensory processing resulting in hyper- or hyposensitivity to specific stimuli. 47 The lack of social understanding and the difficulties with theory of mind may also cause challenging behaviors in GP’s office while waiting in the queue. Changes in the clinician between different appointment is prone to cause social difficulties and influence the patient’s well-being. Among strategies that are taken by PHPs, the participants indicate having the same doctor on most appointments and explaining the medical procedures to the child as the most frequent strategies. One of the least popular strategies is adjusting the sensory environment to the specific sensory profile of the patient. The strategy may be difficult in practice as there is no one way of acting and successful sensory adjustment requires knowing the patient’s sensory issues before.
Limitation of the Study
Due to the online version of the questionnaire, the authors of the study were not able to verify how the ASD diagnoses were conducted for the participants’ children.
The questionnaire used in this study was not validated. Validation of the survey improves the accuracy and reliability of the data collected and based upon the results. To reduce this bias, the questions and answers were designed by experts and were distributed among medical professionals. Moreover, the questionnaire was written in professional language to minimize the possibility of misunderstandings.
The sample size was not calculated for this study. Determining an appropriate sample size is essential for ensuring the study’s ability to detect relationships with adequate statistical power. We endorse performing this step in future survey research to achieve the statistical significance of the findings. In our study, we have collected a large number of questionnaires (159) and were rather focused on the exploration of recent trends in the care for autistic children provided by Polish Primary Healthcare Physicians in parental view. Therefore, we did not define any primary outcome and did not calculate the needed sample size.
Conclusion
Taking comprehensive care for autistic children and their families in the primary healthcare setting becomes a growing necessity as the prevalence of ASD constantly increases. The complexity of caring demands not only taking care of child’s somatic condition but also for the family’s social and mental well-being. Moreover, effective caregiver—physician communication is associated with higher parental satisfaction with the complexity of care, satisfactory adherence to therapeutic recommendations, and increase level of parental trust in primary healthcare enabling parents to discuss issues associated with the whole family system’s wellbeing with the primary healthcare physicians.
The assessment of the comprehensive care for autistic patients and their families provided by the PHPs in Poland that were conducted in the research is definitely insufficient in the parental perspective and the topic needs to be addressed immediately. Unfortunately, in Poland where the study was conducted, there are many barriers in taking complex care of autistic patients in primary healthcare settings. The lack of PHPs, overload of the primary healthcare system, or inadequate training in developmental disorders seem to be of the most importance. Regardless, some initiatives aiming to increase the level of knowledge between PHPs and their abilities to support autistic patients on a complex level need to be undertaken. The doctors must be able to see the early signs of autism and comorbidity, be aware of the social and behavioral difficulties associated with autism and keep up with trends in therapy and possible ways of psychological and educational support as well as know strategies that make the contact with healthcare system easier for the autistic children.
As the ASD rate is increasingly rising, some changes in Polish undergraduate and postgraduate medical education should be implemented. Students and physicians on different levels of education need to be taught about ASD and, what seems to be even more crucial, have access to practical classes on early autism recognition including the use of standardized screening measures such as M-CHAT or STAT as well as learn about the comprehensive care for autistic patients including therapies, comorbidity, supportive strategies.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X241258657 – Supplemental material for The Assessment of Comprehensive Care for Autistic Children Provided by Polish Primary Healthcare Physicians in Parental View
Supplemental material, sj-docx-1-gph-10.1177_2333794X241258657 for The Assessment of Comprehensive Care for Autistic Children Provided by Polish Primary Healthcare Physicians in Parental View by Patryk Domarecki and Katarzyna Plata-Nazar in Global Pediatric Health
Supplemental Material
sj-pdf-2-gph-10.1177_2333794X241258657 – Supplemental material for The Assessment of Comprehensive Care for Autistic Children Provided by Polish Primary Healthcare Physicians in Parental View
Supplemental material, sj-pdf-2-gph-10.1177_2333794X241258657 for The Assessment of Comprehensive Care for Autistic Children Provided by Polish Primary Healthcare Physicians in Parental View by Patryk Domarecki and Katarzyna Plata-Nazar in Global Pediatric Health
Supplemental Material
sj-pdf-3-gph-10.1177_2333794X241258657 – Supplemental material for The Assessment of Comprehensive Care for Autistic Children Provided by Polish Primary Healthcare Physicians in Parental View
Supplemental material, sj-pdf-3-gph-10.1177_2333794X241258657 for The Assessment of Comprehensive Care for Autistic Children Provided by Polish Primary Healthcare Physicians in Parental View by Patryk Domarecki and Katarzyna Plata-Nazar in Global Pediatric Health
Footnotes
Acknowledgements
The authors would like to thank all the people who were engaged in the process of preparation of the questionnaire especially the members of the autistic society who commented on the first draft of the form as well as everyone who shared the link to the questionnaire. Special appreciation goes to all parents who decided to fill out the questionnaires.
Author Contributions
Concept of the research: PD, KPN; Acquisition, analysis, and interpretation: PD, KPN; draft of the first manuscript: PD; critical revision of the first manuscript: KPN; answer to the peer-review process: PD, KPN.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.