
Abstract
Objective:
To report the incidence and survival patterns for children, adolescents, and young adults (CAYA) cancer survivors over the past 20 years.
Methods:
CAYA (under 25 years old) cancer survivors from 17 Surveillance, Epidemiology, and End Results (SEER) registries from 2000 to 2020 were analyzed. A joinpoint regression model was used to analyze the incidence and 5-year survival rate.
Results:
The overall age-standardized cancer incidence (ASIR) of CAYA cancer was 19.26 per 100 000 in 2000 and 21.47 per 100 000 in 2020 in SEER17. The incidence rate of CAYA cancer increased over time. The most common cancer types were leukemia, lymphoma, brain and other nervous system, endocrine system, and male genital system cancer, accounting for over 60% of CAYA cancer cases. The 5-year relative survival rate of CAYA increased from 80.40% in 2000 to 87.80% in 2015.
Conclusions:
There were more CAYA cancer survivors at risk of long-term sequelae.
Keywords
Introduction
According to statistics from the World Health Organization (WHO), approximately 400 000 children and adolescents (0-19 years old) worldwide are diagnosed with cancer every year. 1 In the United States, more than 15 000 children and adolescents were diagnosed with cancer in 2023. 2 Early detection and intervention for various cancers have contributed to improved survival rates. 3 In high-income countries, the 5-year survival rates for children, adolescents, and young adults (CAYA) diagnosed at age 25 or younger have exceeded 80%, indicating that CAYA are surviving cancer more frequently today than in the past. 4
Survivors of cancer in CAYA have unique characteristics and face challenges regarding reproductive health. However, a comprehensive overview of recent patterns of CAYA cancer in the US over the past 20 years has not been reported. This study utilized population-based data from the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) program to characterize temporal patterns in the incidence of CAYA cancers in the US from 2000 to 2020. The primary objective was to characterize the temporal patterns in CAYA cancer overall and by organ system. The secondary objective was to assess temporal patterns in CAYA cancer stratified by sex, age group, and race and ethnicity. These results can provide scientific evidence for cancer preventive strategies in CAYA cancer patients regarding their future risk for long-term sequelae, especially in terms of fertility prospects.
Methods
We obtained the data from the SEER, which is publicly accessible (https://seer.cancer.gov/). SEER is supported by the Surveillance Research Program (SRP) and Population Sciences (DCCPS). Data from 17 SEER registries (Incidence-SEER 17 Registries 2000-2020) were used to identify cancer cases in individuals younger than 25 years from January 1, 2000, to December 31, 2020, only malignant. These 17 SEER registries cover approximately 26.5% of the U.S. population based on the 2020 census, including San Francisco-Oakland SMSA, Connecticut, Hawaii, Iowa, New Mexico, Seattle (Puget Sound), Utah, Atlanta (Metropolitan), San Jose-Monterey, Los Angeles, Alaska Natives, Rural Georgia, California excluding SF/SJM/LA, Kentucky, Louisiana, New Jersey, and Greater Georgia. 5
SEER STAT software 8.4.2 was utilized to estimate cross-sectional incidence rates and the 20-year mean annual percentage change (APC) in incidence rates, as well as the 5-year relative survival rate, stratified by sex (male and female), race (American Indian/Alaska Native, Asian or Pacific Islander, Black, White, Unknown), and age groups (0, 1-4, 5-9, 10-14, 15-19, 20-24). We used the International Classification of Diseases for Oncology, Third Edition (ICD-O-3; WHO 2008) to classify cancer sites.
Bar charts were used to compare changes in cancer incidence between 2000 and 2020 and 5-year relative survival rates between 2000 and 2015. A forest plot was used to show the 20-year APC stratified by sex, race, age, and cancer site. A joinpoint regression model was established to simulate the trend of cancer incidence and 5-year survival rate in CAYA. P-value less than .05 was considered statistically significant. R 4.4.3 was employed to create bar charts, forest plots, and charts showing changes in cancer incidence and survival rates. The R package included ggplot2, splines, rms, stringr, reshape2, forcats, and forestplot.
Ethical Approval and Informed Consent
This cohort study was conducted in accordance with the Declaration of Helsinki. The study was exempt from institutional review board review because no confidential patient information was involved per the 2018 Revised Common Rule (45 CFR §46).
Result
Sociodemographic Characteristics of Cancers Among People Younger Than 25 Years From 2000 to 2020
Between 2000 and 2020, the SEER 17 data file included 129 384 CAYA patients younger than 25 years with cancer in the USA, with 67 873 (52.46%) being male and 61 511 (47.54%) females. Table 1 presents the overall counts of CAYA cancers diagnosed during this period, stratified by age, sex, and race. More than 50% of CAYA cancer patients were aged 14 to 25 years old, and 79.26% were White. Additionally, the gender ratio was consistent across all age and race groups (Table 1).
Sociodemographic Characteristics of CAYA Cancers among People Younger than 25 Years From 2000 to 2020. a
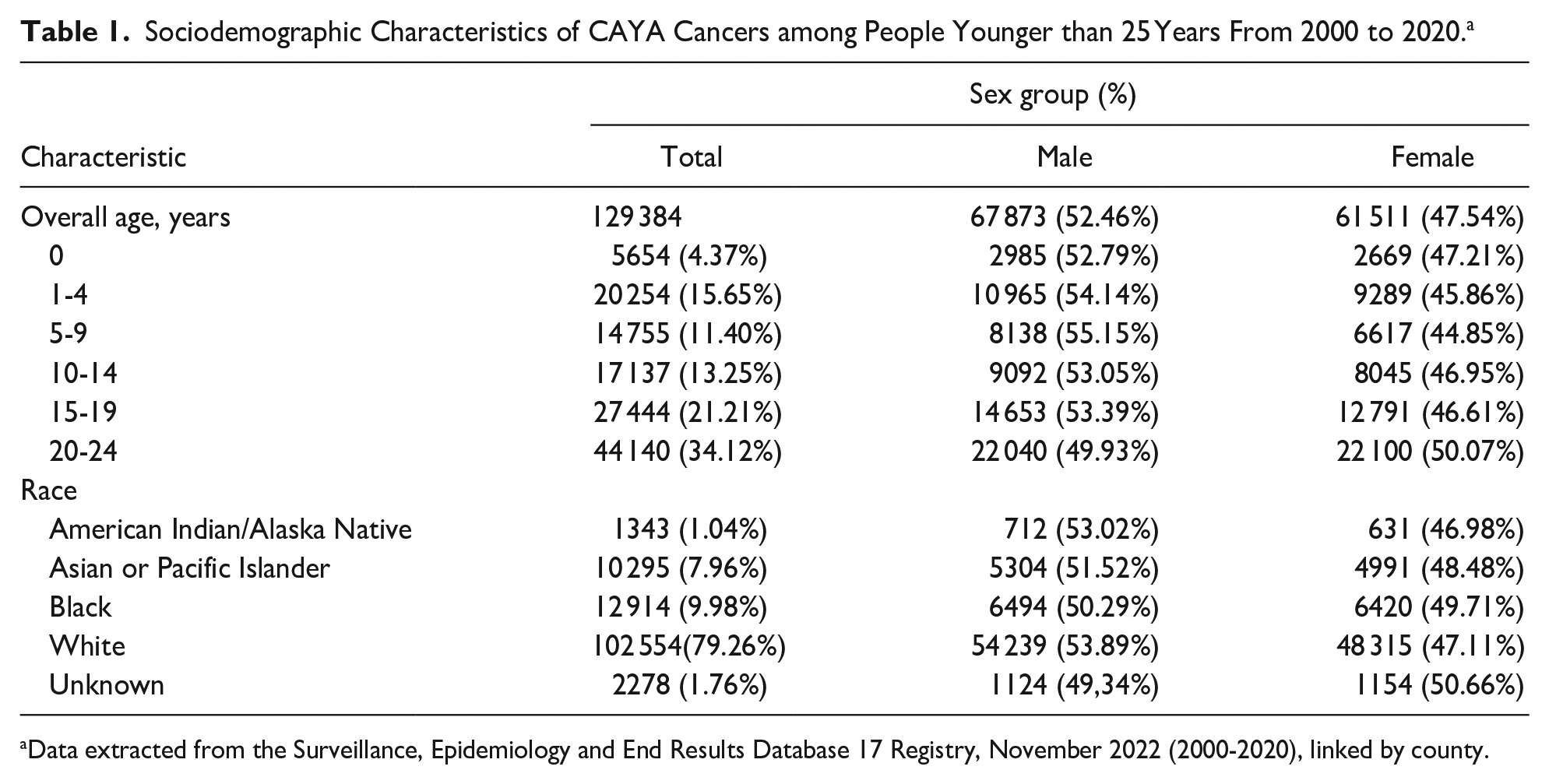
Data extracted from the Surveillance, Epidemiology and End Results Database 17 Registry, November 2022 (2000-2020), linked by county.
Incidence of Cancers Among People Younger Than 25 Years From 2000 to 2020
As shown in Table 2 and Supplemental eFigure 1, the age-standardized incidence rate (ASIR) of cancer among individuals younger than 25 years was 19.26 cases per 100 000 individuals in 2000 and 21.47 cases per 100 000 individuals in 2020. The overall incidence of CAYA cancer increased significantly, with an annual percentage change (APC) of 0.72% (95% CI, 0.49%-0.96%; P < .001).
Incidence of Cancers Among People Younger Than 25 From 2000 to 2020.

Abbreviations: APC, annual percentage change; ASIR, age-standardized incidence rate.
P value of APC from 2000 to 2020.
From 2000 to 2020, the ASIR of cancer among individuals younger than 25 years increased in Asian or Pacific Islander individuals (APC 1.23%; 95% CI, 0.76%-1.70%; P < .001), Black individuals (APC 0.61%; 95% CI, 0.18%-1.04%; P = .008), and White individuals (APC 0.68%; 95% CI, 0.42%-0.94%; P < .001), and decreased in American Indian/Alaska Native individuals (APC, −0.60%; 95% CI, −1.58% to 0.39%; P = .22). The ASIR of cancer among individuals younger than 25 years increased notably in the age groups of 10 to 14 (APC, 1.29%; 95% CI, 0.90%-1.67%; P < .001), 15 to 19 (APC, 0.99%; 95% CI, 0.75%-1.23%; P < .001), and 20 to 24 (APC, 0.61%; 95% CI, 0.34%-0.88%; P < .001).
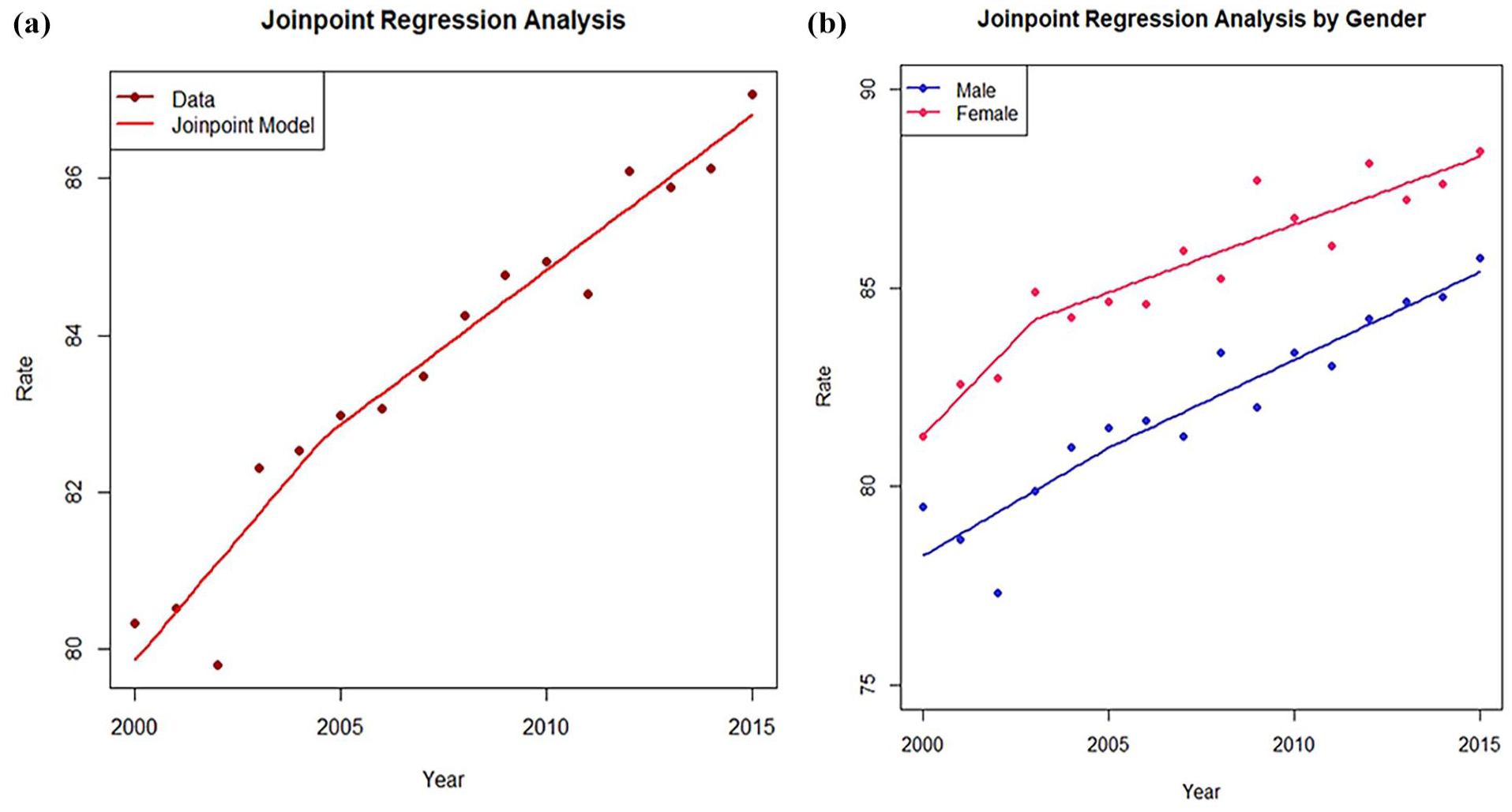
The incidence of cancer among individuals younger than 25 years has increased in both males (APC, 0.70%; 95% CI, 0.47%-0.93%; P < .001) and females (APC, 0.75%; 95% CI, 0.45%-1.04%; P < .001). The trends in the incidence rate of cancer increased from 2000 to 2015 and decreased after 2015, but the incidence rate of cancer in 2020 was still higher than that in 2000 among individuals younger than 25 years. Grouped by sex, both males and females followed a similar trend, with the incidence rate of cancer higher in males than in females (Figure 1).

The trend in incidence rate of cancer from 2000 to 2020 among people younger than 25. (a) The incidence rate of cancer from 2000 to 2020 among people younger than 25. (b) The incidence rate of cancer from 2000 to 2020 among people younger than 25, stratified by sex.
Additionally, the cancer that saw a decline in incidence from 2015 to 2020 mainly included respiratory system (0.31-0.27), bone and joints (0.94-0.86), soft tissue including heart (1.26-1.06), skin excluding basal and squamous (0.96-0.61), urinary system (0.79-0.74), eye and orbit (0.35-0.27), brain and other nervous system (3.07-2.59), endocrine system (2.89-2.42), myeloma (0.02-0.01), leukemia (4.46-4.30), Kaposi sarcoma (0.06-0.03), and miscellaneous (0.97-0.78).
Leading Causes of Cancer Among People Younger Than 25 Years From 2000 to 2020
The total number of cancer cases among individuals younger than 25 years was 5253 in 2000 and 6021 in 2020. The leading causes of CAYA cancer during these 20 years were similar. Leukemia/lymphoma was the most common cancer in the USA in 2000 (1902 cases) and in 2020 (2094 cases), followed by brain and other nervous system cancer in 2000 (791 cases) and in 2020 (710 cases), endocrine system cancer in 2000 (466 cases) and in 2020 (696 cases), and male genital system cancer in 2000 (362 cases) and in 2020 (468 cases), accounting for 67.02% in 2000 and 65.45% in 2020 of total cancer cases, respectively. There is a gender difference in the leading cause of CAYA cancer in 2020. The top 5 cancers in males included leukemia, lymphoma, male genital system cancer, nervous system cancer, and endocrine system cancer, accounting for 75.4% of total cancer cases in males in 2020, whereas the most common cancers in females were leukemia, endocrine system cancer, lymphoma, nervous system cancer, and digestive system cancer, accounting for 63.75% of total new cancer cases in females (Supplemental eTable 1).
In addition, the incidence of cancers in the digestive system (APC, 5.44%; 95% CI, 4.46%-6.43%; P < .001), male genital system (especially testicular cancer, APC, 1.02%; 95% CI, 0.60% to 1.44%; P < .001), endocrine system (especially thyroid cancer, APC, 2.60%; 95% CI, 2.01%-3.19%; P < .001), and leukemia (APC, 0.57%; 95% CI, 0.31%-0.84%; P < .001) increased most significantly. Instead, the incidence of cancer in skin excluding basal and squamous cancer (APC, −3.03%; 95% CI, −3.73% to −2.33%; P < .001) and female genital system (especially cervical cancer, APC, −0.65%; 95% CI, −1.14% to −0.15%; P = .01) declined obviously (Table 3, Supplemental eTable 2 and eFigure 2).
Incidence of Cancers Stratified by Cancer Site Among People Younger Than 25 From 2000 to 2020.

Abbreviations: APC, annual percentage change; ASIR, age-standardized incidence rate.
P value of APC from 2000 to 2020.
Five-Year Relative Survival Rate of Cancers Among People Younger Than 25 From 2000 to 2015
For both sexes combined, the overall 5-year relative survival rate of cancer among individuals younger than 25 years increased from 80.40% (95% CI, 78.84%-81.87%) in 2000 to 87.80% (95% CI, 86.65%-88.86%) in 2015. Both males and females saw an increase in the 5-year relative survival rate, with females younger than 25 years reaching a 5-year relative survival rate of 89.86% in 2015, higher than that of males (85.58%) (Table 4, Figure 2). The 5-year relative survival rate of cancer for all races younger than 25 years was higher than in 2000, but the survival rate for Blacks was relatively low. For all age groups younger than 25 years, the 5-year survival rate has been increasing from 2000 to 2015, but the rate for the 0 to 1 year age group is lower than for other age groups (Table 4, Supplemental eFigure 3).
Five-Year Relative Survival Rate of Cancers Among People Younger Than 25 From 2000 to 2015.

Confidence interval: Log(−Log()) Transformation. The level is 95%.
The relative cumulative survival increased from a prior interval and has been adjusted.
The change of 5-year relative survival rate of cancers among people younger than 25 years from 2000 to 2015. (a) The change of 5-year relative survival rate of cancers among people younger than 25 years from 2000 to 2015. (b) The change of 5-year relative survival rate of cancers among people than younger 25 years from 2000 to 2015, stratified by sex.
As mentioned above, for both sexes combined, the leading causes of cancer among individuals younger than 25 in the USA included leukemia/lymphoma, brain and other nervous system cancer, endocrine system cancer, and male genital system cancer. In 2015, the 5-year relative survival rate of leukemia (72.53%, 95% CI, 67.54%-76.89%), lymphoma (93.38%, 95% CI, 91.02%-95.13%), brain and other nervous system cancers (79.07%, 95% CI, 73.53%-83.58%), endocrine system cancers (98.98%, 95% CI, 97.61%-99.56%) increased dramatically compared with 2000. Moreover, the 5-year relative survival rate of male genital system (94.89%, 95% CI, 92.10%-96.71%) and female reproductive system tumors also increased (87.51%, 95% CI, 80.79%-92.00%) (Table 5, Supplemental eFigure 4).
Five-Year Relative Survival Rate of Cancers Stratified by Cancer Site Among People Younger Than 25 From 2000 to 2015.
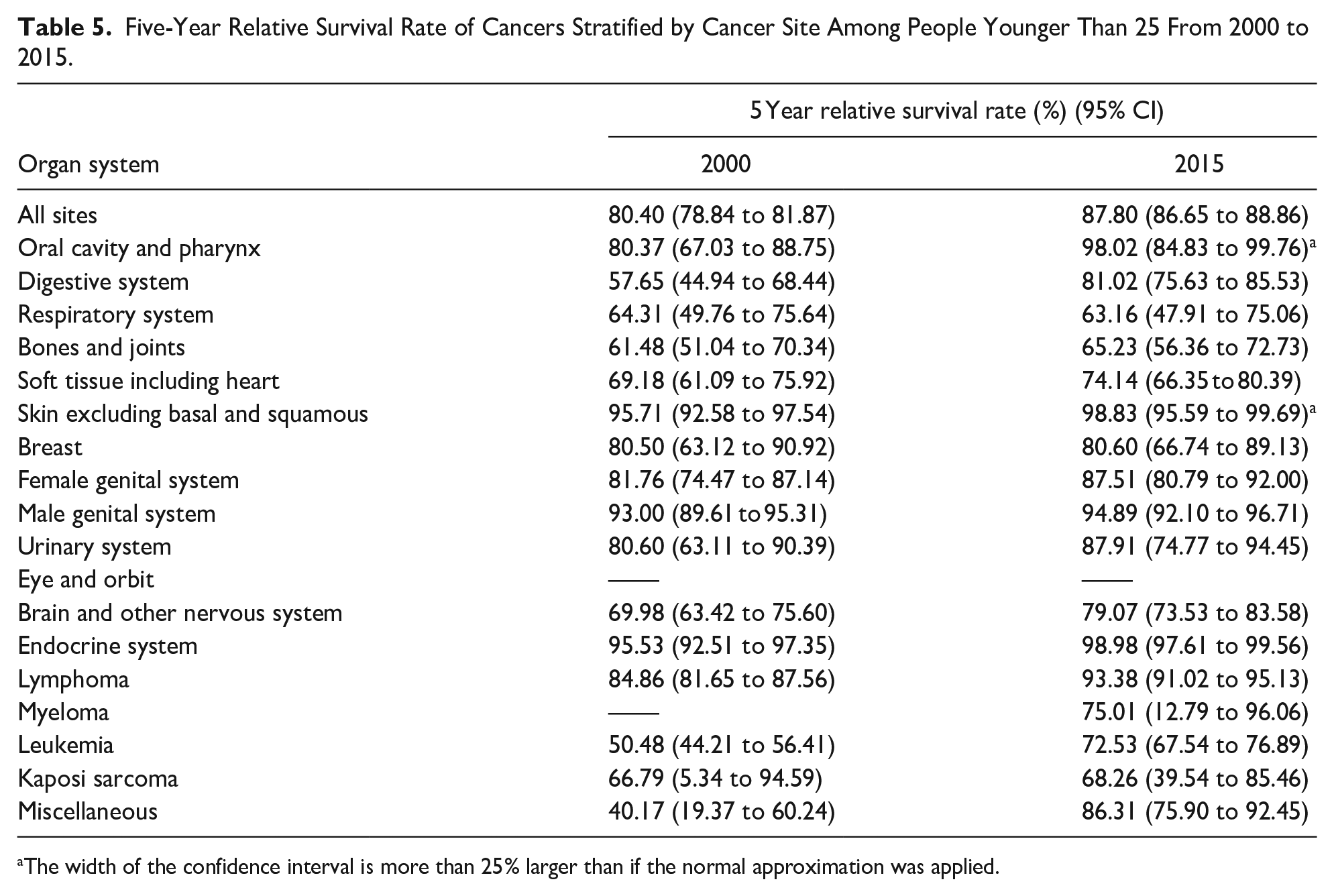
The width of the confidence interval is more than 25% larger than if the normal approximation was applied.
Comparatively, CAYA cancers with lower survival rates in 2015 included respiratory system cancer (63.16%, 95% CI, 47.91%-75.06%), bone and joint cancer (65.23%, 95% CI, 56.36%-72.73%), and Kaposi Sarcoma (68.26%, 95% CI, 39.54%-85.46%) (Table 5). Additionally, cranial nerves/other nervous system cancer in males and liver/intrahepatic bile duct cancer in females had low survival rates, at 50.2% (95% CI, 18.4%-76.3%) and 50.0% (95% CI, 20.8%-73.6%), respectively (Supplemental eTable 1).
Discussion
In this population-based study, data from 17 SEER registries in the United States were collected to analyze cancer cases in individuals under the age of 25 from 2000 to 2020. To our knowledge, this is the first report on the incidence and long-term overall survival patterns for CAYA cancer survivors in the past 20 years in the USA. The overall ASIR of CAYA cancer was 19.26 per 100 000 in 2000 and 21.47 per 100 000 in 2020. The trends in the incidence rate of CAYA cancer increased, with the incidence rate in males higher than that in females. Additionally, the overall 5-year relative survival rate of CAYA cancer increased from 80.40% (95% CI, 78.84%-81.87%) in 2000 to 87.80% (95% CI, 86.65%-88.86%) in 2015, with the 5-year relative survival rate for females under 25 years reaching 89.86%, higher than that for males (85.58%). Cancers are becoming more common in younger populations, and rising 5-year survival rates are leading to a growing number of cancer survivors.
With the advancement of cancer research, the concept of early-onset cancer has emerged, often defined as cancers diagnosed in adults under 50 years of age. 6 Previous studies on cancer incidence have often focused on early-onset cancers, typically under the age of 50. 7 Among individuals under 50 years old, breast, thyroid, and colon and/or rectum cancers are more common than other sites. 7 However, breast and thyroid cancers are not common in individuals younger than 25, whereas leukemia, lymphoma, brain and other nervous system cancers, male genital system cancers, and digestive system cancers are more prevalent, accounting for more than 50% of all sites in CAYA individuals. This suggests that there are different characteristics of tumor onset in CAYA individuals. In the following Table 6, we summarized the incidence and survival rates of common cancers among individuals of different ages and regions. In recent years, the common sites of CAYA tumors have changed compared to before, with the blood system, nervous system, and male genital system becoming more common. In our study, we observed that leukemia, lymphoma, brain and other nervous system cancers, endocrine system cancers, and male genital system cancers were the top 5 cancer types, collectively accounting for more than 60% of all CAYA cancer cases. Additionally, there was a notable increase in digestive system cancers, while the incidence of skin cancers excluding basal and squamous cell carcinoma, as well as female genital system cancers, declined. Various factors are associated with cancer in CAYA individuals, including intrauterine radiation exposure, 8 transplacental exposure to environmental carcinogens, 9 smoking during pregnancy, 10 exposure to environmental tobacco smoke, 11 and inherited genetic factors. 12 The increasing obesity rate among young people may be one of the reasons for the rising of colon and rectum cancer incidence. 13 However, it has to be acknowledged that the majority of the increase in the incidence rate of appendiceal cancer is likely an artifact due to the reclassification of appendiceal carcinoids/neuroendocrine tumors as malignant. 14 The same reason may also apply to miscellaneous, but unfortunately, we have not found any relevant reports.
Comparative of Common Cancer and Survival Rates in CAYA Cancer Patients.

Abbreviations: The SEER Database, Surveillance, Epidemiology, and End Results Database; EUROCARE, European Cancer Registry Based Study on Survival and Care of Cancer Patients; KCCR, Korea National Cancer Incidence database in the Korea Central Cancer Registry; CNS, central nervous system; PBCR: The Brazilian Population-Based Cancer Registry.
5-relative survival rate, 2012 to 2016.
Relative survival rate, population weighted.
5-relative survival rate, 2016.
The advancement of auxiliary examination techniques such as ultrasound, CT, and MRI, along with the application of puncture biopsy, has led to a rapid increase in the incidence of thyroid cancer, although concerns about overdiagnosis exist.19,20 Public health efforts targeting melanoma have resulted in a decline in its incidence among CAYA individuals.21,22 The significant decrease in the incidence of cervical cancer can be attributed to the widespread use of the HPV vaccine.20,23 However, some cancers, like osteosarcoma, have not seen significant treatment breakthroughs, 24 leading to minimal changes in survival rates.
The overall 5-year relative survival rate of CAYA cancer increased from 80.40% (95% CI, 78.84%-81.87%) in 2000 to 87.80% (95% CI, 86.65%-88.86%) in 2015. With advancements in treatment technology, such as genome-based and immunologic-based treatments, the cure rate of cancer in CAYA individuals has improved.25,26
The higher survival rates have led to an increase in CAYA cancer survivors, who face dual challenges transitioning from precancerous states to survivors and from childhood or adolescence to adulthood. 27 Apart from cancer affecting their growth, 28 two-thirds of CAYA survivors are at a particular risk of long-term sequelae from the cancer itself or the therapies used. 29 Compared to healthy individuals, adolescent and young adult (AYA) cancer survivors are at a higher risk of poor health-related quality of life due to a higher burden of total chronic health conditions (CHCs). 30
Larger epigenetic age accelerations were measured among children and adolescent cancer survivors associated with early-onset obesity, morbidity burden in general, and late mortality. 31 Children and adolescent cancer survivors, especially those from low- and middle-income backgrounds, are more likely to experience physical late effects, including hypothyroidism, metabolic syndrome, gonadal dysfunction, cardiac dysfunction, and even secondary primary cancer.32,33 Psychological problems are also more severe in young cancer patients. 34 Additionally, CAYA cancer survivors are at risk of delayed cancer diagnosis. 35 Collectively, these individuals require more psychological and social support. 36
While CHCs and secondary primary cancer pose significant threats to long-term survival, fertility issues may be a more pressing concern for specific populations, such as young patients. In the Dutch childhood cancer survivor cohort, 3-quarters of the 1317 male survivors reported a desire to have children. 37 In addition, the reproductive problems of unmarried survivors are related to their younger age at diagnosis. 38 Common cancer treatments such as radiotherapy and chemotherapy can impair reproductive health and fertility.39 -44 Compared to healthy individuals, cancer survivors are 80% more likely to experience diminished fertility after cancer treatments. 45 Female cancer survivors are particularly vulnerable to fertility damage due to the destruction of ovarian function. 46 Premature ovarian insufficiency (POI), which impacts fertility and estrogen production, and the prevalence of POI in CAYA survivors of cancer ranged from 2.1% to 82.2%. 47 POI can manifest as acute ovarian failure (AOF) in the years following cancer treatment, leading to either the cessation of menstruation or the failure to achieve natural menarche. POI can also result in premature menopause after cancer treatment, leading not only to infertility but also to premature aging of the body. The risk of AOF and POI depends on factors such as age, cyclophosphamide equivalent dose (CED), and the quantity of radiation (RT). For example, with a high CED, the risk of AOF is greater than 5% for individuals aged 1 to 20 with a dose to the least affected ovary (LAO) of less than 2 Gy, and the risk of POI by age 20 approaches 100%. 48 Children born to female cancer survivors are at an increased risk of being born preterm and with low birth weight.49,50 Similarly, some male cancer survivors experience reduced sperm count and azoospermia due to treatments such as high cumulative radiation.41,51 For instance, when the mean testicular dose exceeds 1 Gy, the rate of oligospermia increases to over 90% at 12 months. 52 These cancer survivors often experience depressed mood due to the damage to their reproductive function, which can be particularly severe in females compared to males. 53 Therefore, the reproductive health of young cancer survivors is a critical aspect of their overall well-being that cannot be ignored. In summary, compared with other groups, the focus of care for young cancer survivors is to manage the potential long-term consequences of treatment, especially the protection of fertility. 54
Oncofertility focuses on addressing the intersection of oncology and reproductive medicine to preserve or restore the reproductive function of cancer survivors. 55 Fertility preservation (FP) involves specific medical interventions to protect the fertility of individuals at risk of infertility due to their disease or its treatment. This can include cryopreservation of oocytes, embryos, ovarian tissue, sperm, and testicular tissue. 56 The gold standards of FP in female cancer patients are oocyte and embryo vitrification. With the advancements in assisted reproductive technology (ART), an increasing number of female cancer survivors have been able to have offspring. 57 Other FP techniques for females include ovarian tissue cryopreservation58,59, in vitro maturation (IVM) 60 and stem cell regeneration. 61 Stem cells currently under study for FP include embryonic stem cells (ESCs), 62 human pluripotent stem cells (hPSCs) 63 and mesenchymal stem cells (MSCs). Further, MSCs contained human amniotic epithelial cells (hAECs), 64 umbilical cord mesenchymal stem cells (UC-MSCs), 65 human placenta-derived mesenchymal stem cell (hPMSC). 66 Anti-Müllerian hormone (AMH) decreased or undetectable after treatment in cancer survivors can be regarded as an indicator of ovarian function. 67 For male cancer patients, the FP gold standard is sperm cryopreservation, with cryopreservation of testicular tissue and in vitro spermatogenesis as complementary options. 57 Spermatogonial stem cells (SSCs), which have the ability to self-renew and differentiate, are considered an ideal tissue for cryopreservation. 68 Additionally, raising awareness among young cancer survivors about the potential long-term reproductive effects of cancer treatment is a priority in current care. 69 Therefore, more efforts should be focused on FP for young cancer survivors to help preserve their fertility and improve their quality of life after cancer treatment.
To our knowledge, this is the first report on the cancer incidence and survival rates among individuals younger than 25 years old in SEER17 over the past 20 years. However, this study has some limitations. Firstly, the majority of participants were White, there may be cases of ensuring medical services and missing reports in other race. 70 Secondly, the study did not consider the impact of the coronavirus disease 2019 (COVID-19) pandemic, as there was a lag in statistical data. Some studies have indicated that COVID-19 may affect the incidence and survival rates of cancer.71,72 Finally, our study was based on the SEER database, and as cancer incidence can vary by region, further research is needed to explore the incidence and survival of cancer in individuals under 25 years old globally.
Conclusion
The incidence of cancer among individuals under 25 years old is increasing in the United States, and the 5-year relative survival rate has also improved compared to previous years. It is crucial for public health and medical services to prioritize the care of CAYA cancer survivors to prevent late sequelae related to reproduction.
Supplemental Material
sj-docx-1-gph-10.1177_30502225251370801 – Supplemental material for The Incidence and 5-Years Relative Survival Rate of Cancer Among People Younger Than 25 Years in the US, 2000 to 2020: A SEER-Retrospective Study and Fertility Preservation Considerations
Supplemental material, sj-docx-1-gph-10.1177_30502225251370801 for The Incidence and 5-Years Relative Survival Rate of Cancer Among People Younger Than 25 Years in the US, 2000 to 2020: A SEER-Retrospective Study and Fertility Preservation Considerations by Chengqi Xiao, Min Ji and Dongmei Lai in Sage Open Pediatrics
Footnotes
Author Contributions
DML, CDX was involved in data acquisition, analysis and manuscript drafting. DML and MJ revised the manuscript. All authors contributed to the article and approved the submitted version.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Natural Science Foundation of China (82271664), the Research Projects of Shanghai Municipal Health Committee (202240343); the interdisciplinary program of Shanghai Jiao Tong University (YG2022ZD028), Shanghai Key Laboratory of Embryo Original Diseases (Shelab2022ZD01).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.