
Abstract
Idiopathic hypoparathyroidism is a rare endocrine disorder characterized by hypocalcemia secondary to inadequate parathyroid hormone secretion. Hypocalcemia-related cataract is most often observed in patients with postoperative hypoparathyroidism, whereas primary hypoparathyroidism-related cataract is rare and displays slow progression. Cataract usually occurs in people aged 18 to 50 years. Here, we describe a 17-year-old boy with bilateral cataract and a history of hypocalcemic tetany who was diagnosed with idiopathic hypoparathyroidism. Phacoemulsification with implantation of a monofocal aspherical intraocular lens was performed in the right eye; 6 months later, it was performed in the left eye. Elevated phosphorus and diminished calcium were observed in blood and aqueous humor. A deep anterior chamber, relatively thin central corneal thickness, large white-to-white distance, and thin lens were also observed. During follow-up, neither eye displayed intraocular lens decentration; best-corrected visual acuity was 20/20 in both eyes. These findings suggest that ophthalmologists should be vigilant when hypocalcemic tetany and cataract are present, especially in adolescents and young adults.
Keywords
Introduction
Idiopathic hypoparathyroidism is a rare endocrine disorder characterized by hypocalcemia secondary to inadequate parathyroid hormone secretion. Hypoparathyroidism most commonly results from parathyroid gland injury or surgery (i.e., acquired hypoparathyroidism). Hereditary forms of hypoparathyroidism are syndromic (e.g., autoimmune polyglandular syndrome, DiGeorge syndrome, hereditary deafness, and renal dysplasia syndrome) or non-syndromic (caused by mutations in genes such as parathyroid hormone, glial cells missing homolog B [GCMB], calcium-sensing receptor [CASR], and sex determining region Y-box 3 [SOX3]). 1 Manifestations of long-term hypocalcemia include bilateral cataracts, basal ganglia calcification, and dental hypoplasia. 2 Hypocalcemia-related cataract is most often observed in patients with postoperative hypoparathyroidism, whereas primary hypoparathyroidism-related cataract is rare and displays slow progression. 3 The age at cataract surgery generally ranges from 18 to 50 years. 4 Here, we describe an adolescent with bilateral cataract and a history of hypocalcemic tetany who was diagnosed with idiopathic hypoparathyroidism.
Case report
A 17-year-old boy was admitted to our hospital with a 1-year history of painless and progressive blurred vision. He had experienced occasional muscle cramps and tetany since the age of 6 years; he occasionally received intravenous calcium supplementation without vitamin D3. He had no symptoms of renal or intestinal disease, no history of epilepsy or convulsions, no history of thyroidectomy, and no known comorbidities. He reported no photosensitivity, arthralgia, or oral ulcerations; he also reported no systemic diseases (e.g., diabetes and hypertension). His family history was unremarkable. He had a positive Chvostek’s sign and a positive Trousseau’s sign. Physical examination revealed no evidence of rickets or enamel hypoplasia, no deformity, and no cognitive deficiency. Ophthalmological examination revealed bilateral cortical cataracts (Figure 1a–c), but no other ocular abnormalities. Electrocardiography findings were normal. Head computed tomography showed no signs of calcification. The ocular and biochemical findings are summarized in Tables 1 and 2. The results of other systemic investigations (e.g., liver and kidney function, complete blood count, erythrocyte sedimentation rate, blood glucose, and sexually transmitted infections) were unremarkable. Finally, there were no signs of diabetes mellitus, autoimmune thyroiditis, autoimmune parathyroid destruction, or autoimmune polyglandular syndrome. After comprehensive assessment, the patient with diagnosed with cataract and hypoparathyroidism. With parental consent, intravenous calcium and oral vitamin D3 were administered; the serum calcium level reached 2.02 mmol/mL before cataract surgery. Phacoemulsification with implantation of a monofocal aspherical intraocular lens was performed in the right eye; 6 months later, it was performed in the left eye. Ion concentrations in aqueous humor collected during surgery are shown in Table 2. These concentrations were compared with values in aqueous humor from 10 patients with age-related cataract who did not exhibit systemic diseases. Postoperative ocular examination findings are depicted in Figure 1d–f and Table 1. During 1 year of follow-up, neither eye displayed intraocular lens decentration or posterior capsular opacification. This case report adheres to the CARE guidelines 5 and patient details have been de-identified.
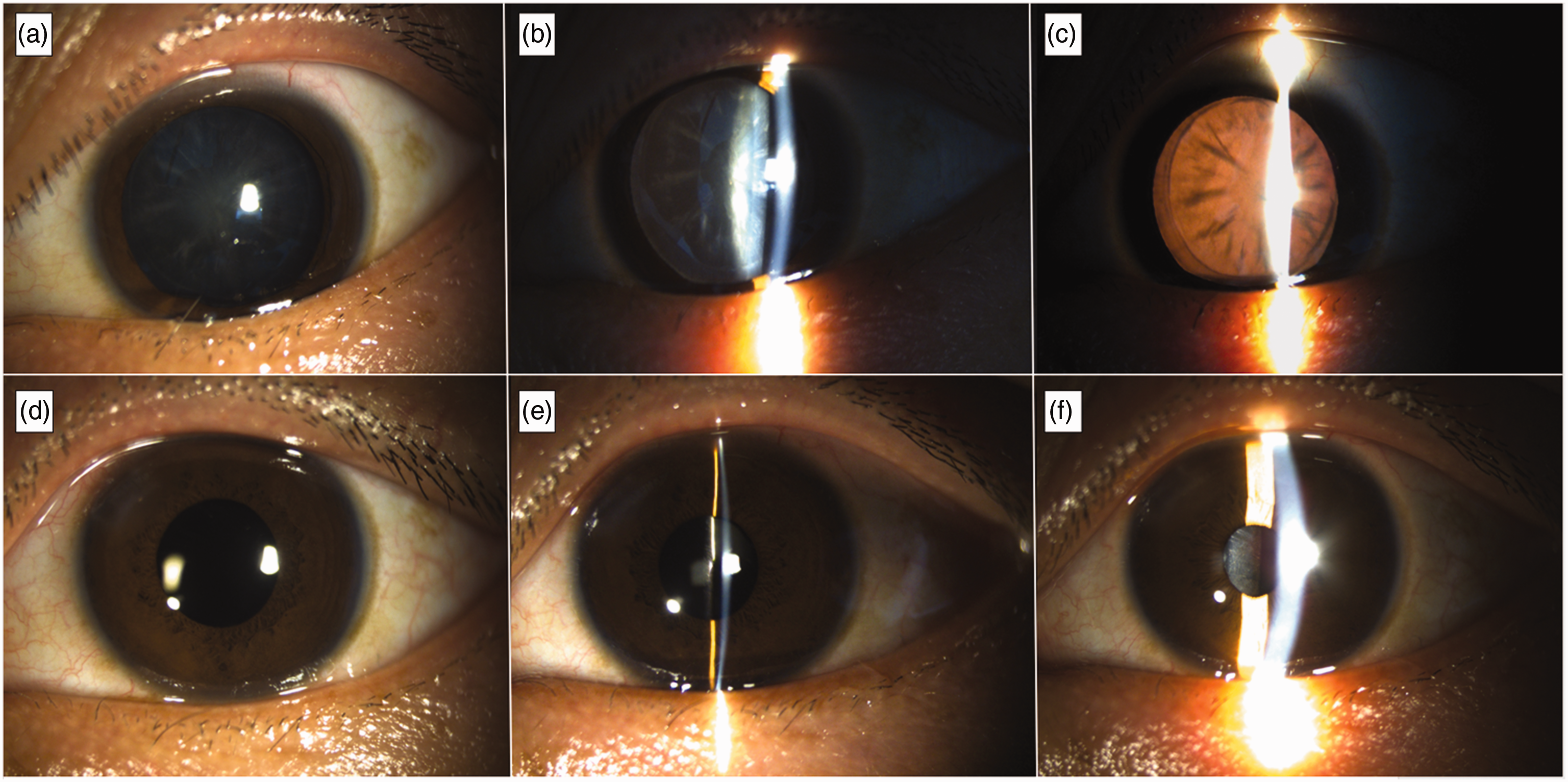
Slit lamp images of cataract in the patient’s left eye. (a–c) Initial presentation: multiple cortical flakes are visible in the lens and (d–f) One day after phacoemulsification and intraocular lens implantation: no cortical flakes are visible.
Ocular findings.
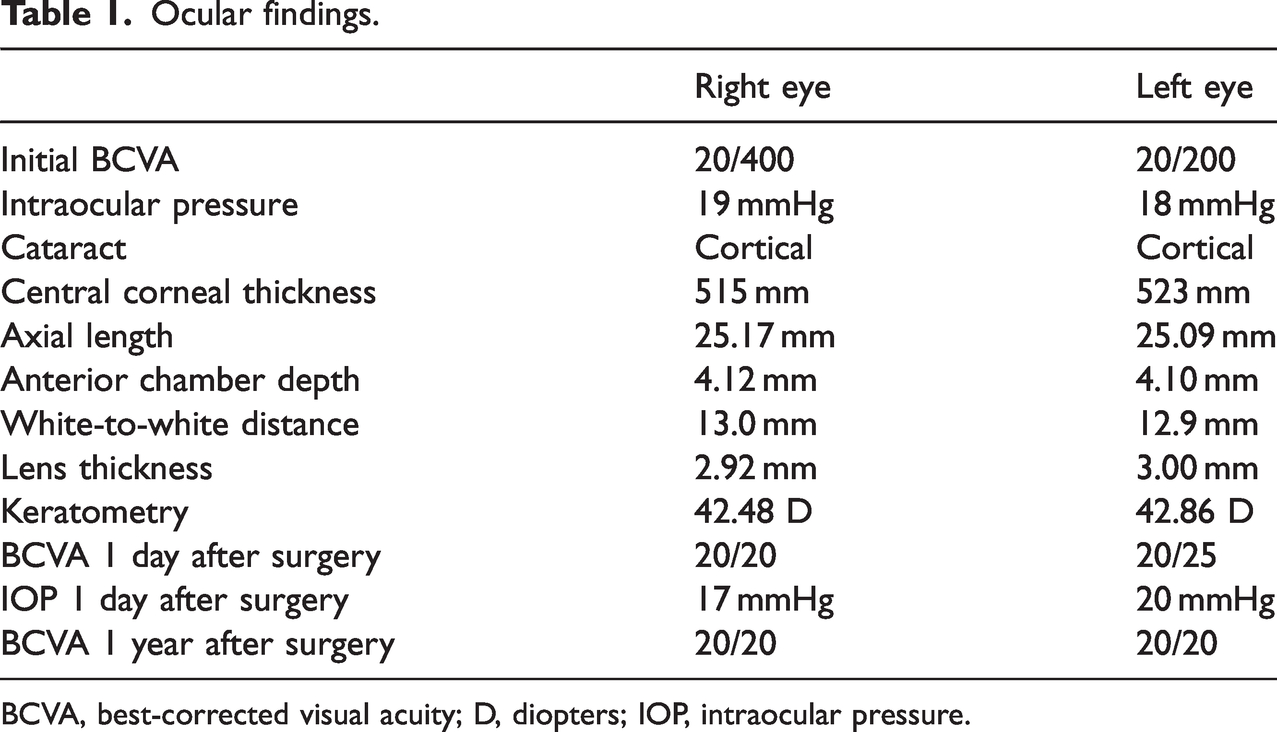
BCVA, best-corrected visual acuity; D, diopters; IOP, intraocular pressure.
Blood and aqueous humor biochemical findings.

*: control eyes comprised aqueous humor samples from 10 patients with age-related cataract who did not exhibit systemic diseases.
Discussion
Although cataract in adolescents and young adults is uncommon (except for congenital cataract), it can occur secondary to ocular trauma, intraocular inflammation, uncontrolled diabetes mellitus, galactosemia, hereditary copper metabolism defects, chronic hypocalcemia, and hypoparathyroidism. 6 Hypoparathyroidism is a rare cause of cataract, especially in young adults; however, it can affect multiple organ systems, including the lens. Cataract development is associated with the duration of hypocalcemic symptoms, chronic hypocalcemia and hyperphosphatemia, and the rate of change in the calcium-phosphorus ratio.7,8 Hypoparathyroidism-related cataract formation is suspected to result from membrane damage caused by low levels of calcium in aqueous humor. 9 The lenticular Na+/K+ pump is inhibited, leading to an inward flux of sodium and water; subsequently, lens fibers swell and dystrophic calcification occurs. Cataract can rapidly progress in patients with autoimmune hypoparathyroidism and acute liver and renal failure. Hyperphosphatemia and vitamin D administration can also contribute to cataract progression.10,11 In the present case, 10 years had passed since the initial onset of hypocalcemic tetany; diminished calcium and elevated phosphorus were observed in our patient’s aqueous humor, compared with values in aqueous humor from patients with age-related cataract. Lenticular calcium levels are also reportedly elevated in patients with cataract, suggesting that calcium and its metabolism play key roles in cataract pathophysiology. 12
Thinner central corneal thickness (CCT) and significantly greater anterior chamber depth have been observed in patients with hypoparathyroidism; these findings are associated with serum calcium levels. 3 CCT is an indicator of corneal endothelial function. In patients with hypoparathyroidism, CCT is significantly correlated with the serum 25-hydroxyvitamin D level, which is important in the maintenance of corneal integrity.3,13,14 Patients with primary hyperparathyroidism display increased CCT and intraocular pressure, as well as positive correlations of intact parathyroid hormone levels with CCT and intraocular pressure. 15 Our patient also had a deep anterior chamber and relatively thin CCT. Notably, he had a large white-to-white distance, which has not been reported in patients with hypoparathyroidism; prospective studies are needed to explore the underlying pathogenesis.
Because cataract with primary hypoparathyroidism develops slowly, it usually appears in older patients. 7 Here, we described a 17-year-old boy with cataract that severely affected visual acuity; he required surgical treatment. Symptoms of hypocalcemia began 10 years before the onset of blurred vision, but the diagnosis of hypoparathyroidism was not made until he visited our hospital. Previously, the patient had not received vitamin D3; he had received intravenous calcium gluconate solely to manage tetany. This treatment approach may have contributed to the early onset of vision-threating cataract. When repeated episodes of hypocalcemic tetany occur, physicians should consider systemic diseases (e.g., hypoparathyroidism), particularly among younger patients. Ophthalmologists should be vigilant when adolescents and young adults display cataract, and they should be aware of the potential for hypoparathyroidism to cause bilateral cataracts.
Footnotes
Acknowledgement
We thank Yanjun Wang, PhD for assistance with the diagnosis and treatment of hypoparathyroidism.
Author contributions
HZ performed the surgery and prepared the manuscript; LY and JX collected and analyzed aqueous humor samples; MZ revised the manuscript for important intellectual content; XL interpreted the results and revised the manuscript. All authors read and agreed with publication of the manuscript.
Data availability
The data used to support the findings of this study are available from the corresponding author upon request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
This study protocol was approved by the Ethics Committee of the Second Hospital of Jilin University (approval no. 2023-yanshen-128). The ethics committee waived the requirement for consent to participate from patients with age-related cataract. The parents of the patient described in this case report consented to publication of this report. This study adhered to the tenets of the Declaration of Helsinki. The authors declare that the CARE guidelines/methodology were followed.
Funding
This work was supported by the China Natural Science Foundation (no. 82000920) and the Natural Science Foundation of Jilin Province (no. 20200201570JC).