
Abstract
Short stay units have been found to decrease congestion in emergency departments (ED), particularly in paediatric demographics, as they offer earlier specialist care and reduced hospital admissions. This study aimed to investigate the potential benefits of a paediatric short stay unit at a secondary metropolitan hospital in Western Australia. A retrospective analysis was conducted on all ED admissions to the paediatric ward in 2022 (N = 938). Most patients (76%) remained in ED for greater than 4-hours, indicating significant congestion. Over half (53%) of patients would have qualified for admission to a short stay unit. Daytime admissions exhibited longer stays than overnight admissions (P = .047), and patients were cleared for discharge on average 2.1-hours before actual discharge time, indicating room for optimisation. This study suggests that a paediatric short stay unit would assist in alleviating ED congestion and improving patient flow in this hospital. Future research should focus on validating these benefits post-implementation.
Keywords
Introduction
Emergency departments (ED) in Western Australia are overburdened with patients, with ambulance ramping regularly making news headlines. The ‘4-hour rule’ is a standardised key performance indicator (KPI) for these departments across Australia, requiring patients be either discharged or transferred to a ward within 4-hours. 1 Delays in ward discharges lead to bed blockages, reduce patient flow and prevent timely access to appropriate hospital beds.1,2 This common issue could be ameliorated through the introduction of a short stay unit assisting to rapidly transit stabilised patients requiring only a short period of observation or simple management.
A significant number of children presenting to ED do not require formal admission to paediatric wards. 3 Similarly, most children admitted to paediatric wards do not require multiday hospital stays. 3 Children who cannot be discharged safely from the ED within 4-hours but require observation or treatment for less than 24-hours would benefit from admission to a short stay unit. Short stay units are efficient and cost effective, particularly for children with acute illness who can be rapidly stabilised and discharged without critical incident. 3 These units lead to earlier management by a specialist led paediatric team, and reduced time spent in a loud, disruptive and potentially traumatic environment, due to exposure of children to adult patient issues encountered in a mixed ED.3,4
Browne and Penna 3 showed 56% of ED paediatric presentations were eligible for admission to a short stay unit after introduction, demonstrating a workload reduction for the general paediatric ward and ED staff. A study involving 220 paediatric patients in Melbourne’s Royal Children’s Hospital found that 65% of children were fit for discharge within 12-hours of admission, with a mean admission duration of 17-hours. 4 This demonstrates that most paediatric patients would be well suited for care in a short stay unit, particularly those requiring only observation or simple management.
A common diagnosis requiring a period of simple observation is a reported head injury. 5 While patients with fractures or neurological abnormalities require formal admission, those with minor symptoms such as drowsiness, amnesia or headache are often fit for discharge after 6-hours of observation.2,5 Further, children with suspected poisoning or potential accidental overdose who remain stable enough for observation are candidates for short periods of observation and simple management. 5 Similarly, a study on asthma patients who had acute exacerbations showed 5 times the cost when admitted to a ward rather than to a short stay unit. 6
Many previous studies have highlighted the benefits of a short stay unit for the paediatric population3,7,8; however, these studies were conducted many years ago and were not based in Western Australia. The current study therefore aimed to investigate the local demographic to gauge applicability of the benefits of a paediatric short stay unit.
The current study was based in a secondary metropolitan hospital in Western Australia which holds a 24-hour mixed ED that sees 65 000 patients annually, 24% of whom are paediatric (aged 0-16 years). The hospital holds a 10-bed paediatric ward with the capacity to accommodate 12 to 13 patients that sees approximately 1220 patients annually, 78% of whom are admitted through ED. Currently, any paediatric patient requiring treatment or observation for more than 4-hours must be formally admitted and transferred to the paediatric ward as there is no short stay unit. The aim of this study was to describe the types of admissions, their duration in the ED and their duration in the ward to demonstrate the viability and possible benefits of the introduction of a paediatric short stay unit.
Objectives
Profile the demographics, diagnoses and outcomes of patients admitted to the paediatric ward through ED.
Profile variations in the timing of patient admissions to the paediatric ward through ED.
Profile the length of stay in ED and in the paediatric ward, to evaluate whether this duration could be substituted safely in a short stay unit.
Profile those with a length of stay up to 36-hours to determine whether earlier discharges could have occurred.
Methods
This study analysed all patients admitted to the paediatric ward through the ED of a secondary public hospital in Western Australia from 1 January 2022 to 31 December 2022, inclusive. Consecutive sampling for the entire 12-month period was utilised with no exclusion criteria (N = 938).
A list of all patients meeting the above inclusion criteria was obtained from the hospital database. These data, enriched with a linked extraction of demographics, diagnoses, time of presentation, admission details and time of discharge, were extracted from the hospital database by the Data and Digital Innovation (DDI) team. The primary focus of the study was to explore cases that spent less than 24-hours in the paediatric ward, as these cases would be eligible for admission to a short stay unit. However, to ensure eligible patients were not excluded unnecessarily acknowledging delays in patient flow, a deeper analysis was conducted on those cases with duration of less than 36-hours to determine if some of these longer admissions would qualify for short stay unit care. For this smaller sample, patients’ hard copy hospital records, including admission notes and discharge summaries, were reviewed to determine whether duration on the ward was unnecessarily lengthened.
Data Analysis
Simple descriptive analysis was performed to obtain most results on the dataset as described below. Chi squared tests of independence were utilised to determine significance of readmission rates and length of stay.
Results
Objective 1: Demographics, Diagnoses, and Outcomes
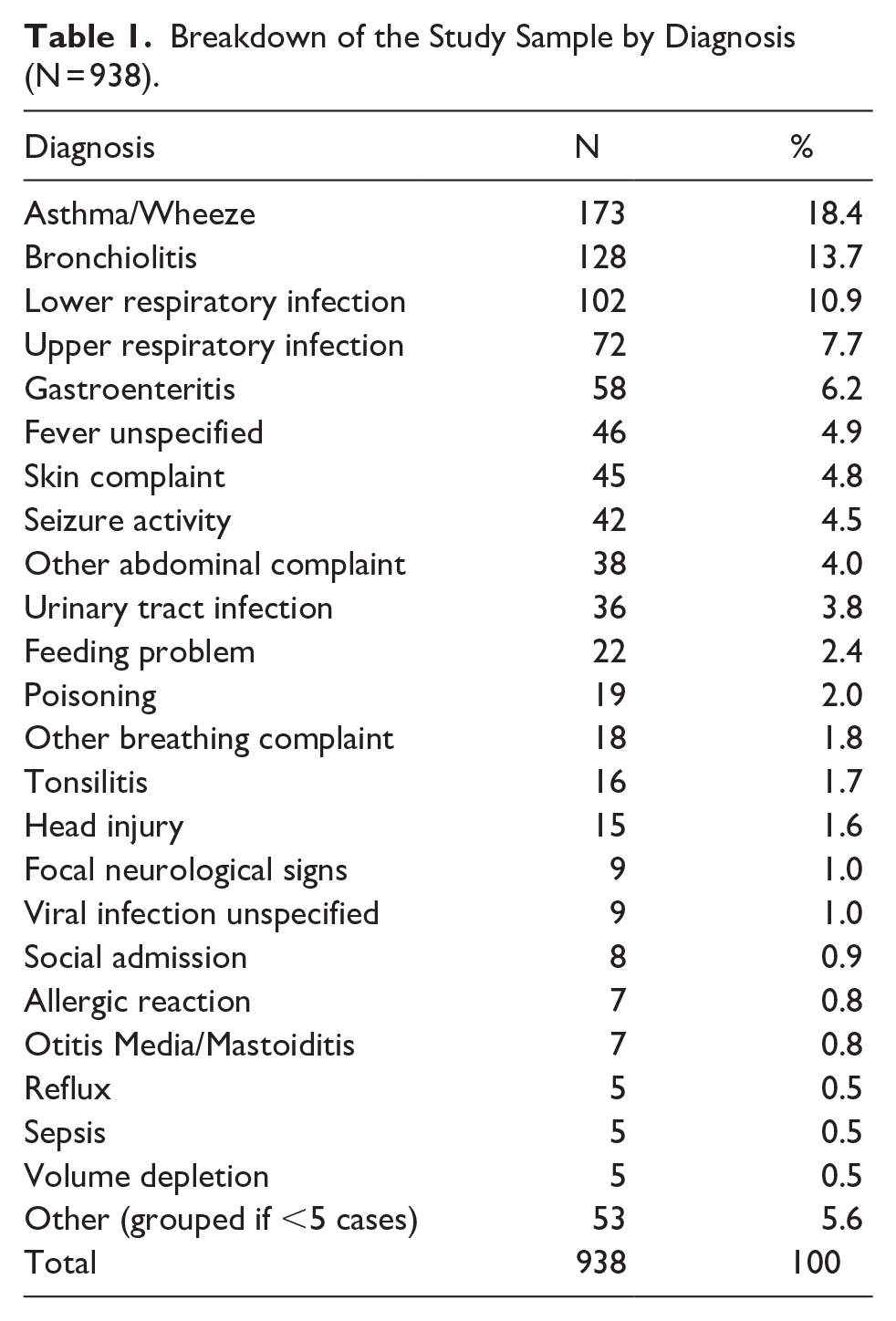
A total of 938 patients were admitted to the paediatric ward from ED in the year 2022. Their ages ranged from 3 days to 16 years and 11 months with an average age of 3 years and 6 months. Of these patients, 46% were male and 54% were female. The reason for presentation is detailed in Table 1. The majority of these patients were discharged home from the paediatric ward (94.9%), with other discharge locations including transfer to a tertiary hospital (3.7%), discharge against medical advice (0.9%) or discharge with child protective service involvement (0.5%).
Breakdown of the Study Sample by Diagnosis (N = 938).
During this period, there were only 5 hospital acquired complications (ICD-10 coded) noted for the cohort, therefore further analysis was not conducted. Instead, readmissions within 28-days were investigated. There were 53 readmissions within 28-days, 41 of which were for the same medical complaint. These complaints were predominantly respiratory in nature, such as viral induced wheeze or bronchiolitis (N = 34). Of these 53 readmissions, 27 were in the patient group that stayed less than 24-hours, whilst 26 were in those with admissions greater than 24-hours (P = .869).
Objective 2: Timing of Admission
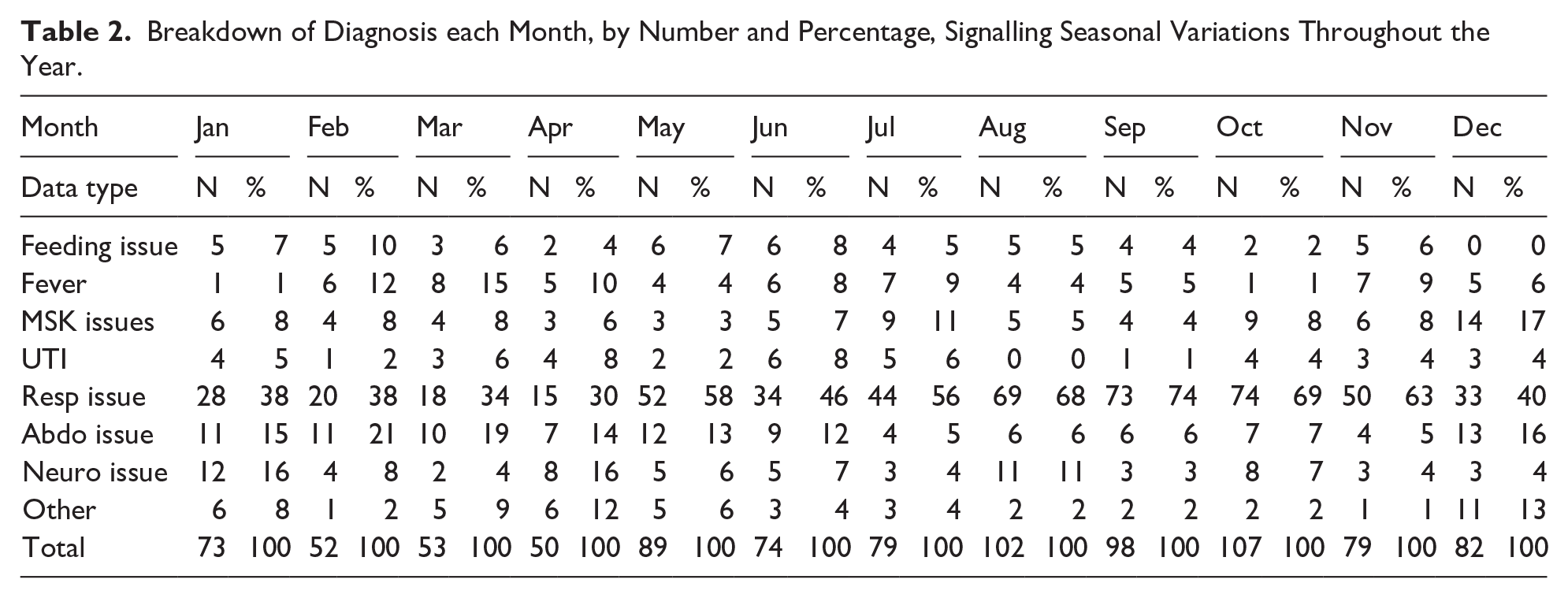
Seasonal and temporal variation of admission numbers were profiled. Presentations were highest in the winter months, as shown in Table 2. This increase in presentations was predominantly due to increasing respiratory issues which rose from 38% of presentations to 74% of presentations during winter. Daytime admissions (06:00-17:59) accounted for 40% (N = 374) of the study sample and had a mean length of stay of 36.4-hours. Overnight admissions (18:00-05:59) described 60% of the sample (N = 564) and had a statistically significant shorter mean length of stay of 32.3-hours (P = .047).
Breakdown of Diagnosis each Month, by Number and Percentage, Signalling Seasonal Variations Throughout the Year.
Objective 3: Duration of Stay
The length of stay in ED and in the paediatric ward is illustrated in Table 3. The majority of ED patients (75%) remained in ED for more than 4-hours, with only 24% meeting the 4-hour KPI (1% missing data). In the paediatric ward, 53% of patients were admitted for less than 24-hours, with 47% needing a longer admission.
Mean, Median and Interquartile Range, in Hours, for the Duration of Stay in Emergency Department (ED) and in the Paediatric Ward.

Total N = 938 for the Paediatric Ward sample, and N = 927 for the ED sample as there were 11 missing datapoints.
Objective 4: Cohort With Length of Stay Less Than 36-Hours
A total of 615 cases were admitted to the ward for less than 36-hours. A power calculation (95% CI, 10% error) determined a sample size of 84 was adequate to obtain generalisable information applicable to the total cohort. Medical records of the randomly selected 84 patients with a length of stay less than 36-hours were reviewed. These demonstrated that 38% required observation only, while 62% included management such as salbutamol burst therapy, intravenous hydration or antibiotics. On average, clearance for discharge occurred 2.1-hours prior to the actual time of discharge (minimum 0.5-hours, maximum 15.7-hours).
Discussion
This study demonstrated that 53% of paediatric admissions from ED remained in the ward for less than 24-hours and would therefore qualify for admission to a short stay unit. It is worth noting this figure is considered conservative as, in the subset sample of admissions for less than 36-hours, all patients could have been discharged sooner if patient flow had been improved. Additionally, this subset analysed demonstrated that over one-third of patients were managed with observation only, which could easily occur in a short stay unit. The main reason for presentation to hospital was respiratory issues (51%) which can range in severity. However, early risk stratification of these patients could identify those suitable for a shorter period of observation, burst therapy or rehydration. Other diagnoses commonly managed in short stay units in the past were found to be frequent in this study sample, including head injury, poisoning, allergies, social admissions and rashes.3,6,7 Importantly, this study also demonstrated no significant increase in readmissions within 28 days for patients who had a less than 24-hour stay. This could suggest that shorter durations of stay do not lead to higher readmission rates, which is supported in past literature.9,10 However, it is worth noting that these shorter durations are often linked to simpler presentations (eg, head injuries, poisonings), whilst longer stays are often associated with greater comorbidities and chronic diseases. It is therefore unclear whether the comparison truly represents safety in earlier discharges or rather reflects different demographic groups.
One of the many advantages of a short stay unit is the improvement in patient flow.1,11 In this study, 75% of the sample remained in ED beyond the 4-hour mark. This is detrimental not only for ED staff but also for patients. A mixed ED with no dedicated paediatric area can be a loud, unsettling, and sometimes traumatic experience for children and their families. This is compounded by prolonged periods managed by staff lacking specialist paediatric training. The implementation of a short stay unit can ensure a more efficient transfer of patients from ED to appropriate care settings, reduce delays in care delivery and alleviate congestion in ED.10,11 By moving patients with short term care needs to a specialised unit, ED staff can focus on more critical cases, reduce wait times and enhance the overall patient experience. Previous studies have illustrated that the introduction of a short stay unit leads to improvement in patient flow, and increased patient satisfaction.3,7,10
Past studies have estimated paediatric short stay unit beds cost one-fifth of ward admission beds. 3 Short stay units are designed to streamline the use of resources, including medical staff, equipment and facilities. This efficiency not only benefits patients but also optimises the allocation of hospital resources, leading to improved resource management.10,12 By avoiding unnecessary long-term admissions and maximising the utilisation of healthcare resources, hospitals can reduce operational costs and enhance financial sustainability.3,12
The current study showed variation in the length of stay based on timing of admission. The reduced length of stay in overnight admissions is expected as discharge planning occurs on morning consultant rounds, for which night admissions are closer in time. Higher admissions in winter months are also expected as respiratory ailments are the primary reason for presentation, and virus transmission is higher in winter. 6 This opens the possibility of a trial period for the introduction of a short stay unit, starting during winter when the paediatric patient load is high, and continuing if found to be beneficial.
The strength in this study lies in the sample size, with all 938 admissions from the year 2022 included in the analysis. Consecutive sampling and extraction from the digital source database limited the potential for collection bias and human error. However, the retrospective nature of this study, alongside the reliance on databases, may limit the accuracy of the data. Missing data and potential inconsistencies in data entry should be taken into consideration when interpreting the results.
This study indicates that most paediatric patients would be eligible for a short stay unit admission, supporting the need for such a unit given the potential cost savings and the success of similar units in other states and countries. Future studies could review outcomes after the implementation of a short stay unit to determine whether the proposed benefits are realised.
Conclusion
The current study found that only 24% of patients met the 4-hour KPI in the ED and that over half (53%) the patients would have qualified for admission to a short stay unit. This shows potential for the creation of a short stay unit to alleviate congestion and improve patient flow. Additionally, daytime admissions had a statistically significant longer stay compared to overnight admissions (P = .047), and patients were cleared for discharge on average 2.1-hours before actual discharge, highlighting opportunities for earlier discharge processes. Peak admission rates in winter, primarily due to respiratory issues, emphasise the need for targeted resources during this period. Establishing a short stay paediatric unit is a strategic move that offers clear advantages for patient care and hospital efficiency. Given the study’s findings and the success of similar units in other regions, a paediatric short stay unit would likely yield significant improvements in patient outcomes and operational performance. Future research could focus on validating these anticipated benefits by examining patient outcomes, cost savings and overall hospital performance post-implementation. Continuous evaluation will ensure that the short stay paediatric unit meets the evolving needs of paediatric patients and the healthcare system.
Footnotes
Acknowledgements
Thanks must go to the Data and Digital Innovation Departments, specifically Alison Sewell and Michael Quan, for their work in extracting the study’s sample from the hospital database.
Ethical Considerations
This study met the criteria of a quality improvement project and was therefore granted ethics approval through the Governance Evidence Knowledge Outcomes (GEKO) committee. The quality activity number for this project was 49448. This approval waived the need for individual informed consent given the retrospective, de-identified and non-interventional nature of this study.
Author Contributions
Christine Burke: Conceptualisation and design, data acquisition and analysis, drafting and revising the manuscript, approval of the final manuscript and accountability for the work. All 5 authors met the criteria of substantial contributions, drafting and revising, approval and accountability. Dale Edgar: Conceptualisation and design, data acquisition and analysis, approval of the final manuscript and accountability for the work. All 5 authors met the criteria of substantial contributions, drafting and revising, approval and accountability. Aharon Friedland: Data acquisition and analysis, approval of the final manuscript and accountability for the work. All 5 authors met the criteria of substantial contributions, drafting and revising, approval and accountability. Janani Prathibha Kariyawasam: Conceptualisation and design, data acquisition and analysis, approval of the final manuscript and accountability for the work. All 5 authors met the criteria of substantial contributions, drafting and revising, approval and accountability. MCG Karunanayake: Conceptualisation and design, approval of the final manuscript and accountability for the work. All 5 authors met the criteria of substantial contributions, drafting and revising, approval and accountability.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.