
Abstract
Introduction:
Testicular torsion (TT) and torsion of the appendix testis or epididymis (TATE) are common causes of the acute scrotum, but differentiating them remains difficult. While meteorological factors have been linked to TT, their clinical significance is unclear.
Methods
We retrospectively analyzed TT and TATE cases diagnosed via surgical exploration at Nagasaki university hospital (June 2018-March 2023). Clinical findings, seasonal variations, and meteorological factors—including temperature, atmospheric pressure, and humidity—were evaluated.
Results
Among 53 cases (31 TT, 22 TATE), TT patients were significantly older (median: 14.0 years, p = 0.026) and more frequent in winter (p = 0.023). TT onset correlated with lower maximum, minimum, and ambient temperatures (p = 0.010, 0.024, 0.006). Over 90% of cases between midnight and 8:00 am were TT.
Conclusion
TT is associated with lower temperatures, winter, and midnight to morning onset. These findings may enhance diagnostic accuracy and clinical decision-making.
Introduction
Acute scrotum refers to the sudden onset of scrotal pain and erythema. The most common causes of acute scrotum include testicular torsion (TT), torsion of the appendix testis or epididymis (TATE), and epididymitis.1,2 Of these, TT involves the twisting of the spermatic cord, leading to ischemic changes in the testes. In severe cases, TT can result in necrosis and the loss of testicular tissue. Recent reports have indicated that the annual incidence of TT among young males is 2.9 to 15.13 per 100,000 individuals, and the rate has increased significantly in recent years.3 -5
The chances of salvaging the testis diminish significantly with delayed treatment after the onset of TT. If treated within 6 hours of onset, the salvage rate exceeds 90%. However, the rate drops to 50% if more than 6 to 12 hours have passed and falls below 10% after 12 to 24 hours. 6 In contrast, even in cases where testicular preservation was achieved following TT, one study suggested that testicular atrophy was observed in all cases when the duration from symptom onset exceeded 6 hours. 7 Factors contributing to the development of testicular atrophy in TT include prolonged pain lasting more than 24 hours and heterogeneity of the testicular parenchyma, as observed on ultrasound. 8
Therefore, prompt hospital visits, rapid diagnosis, clear communication with patients and their parents, and immediate intervention are crucial for maximizing the likelihood of testicular preservation. Scrotal ultrasonography and the Testicular Workup for Ischemia and Suspected Torsion (TWIST) score are commonly used diagnostic tools for TT. 9 In blood tests, an increased white blood cell count (>12,000 cells/mm3) may be observed in TT, which could serve as a supplementary diagnostic indicator. 10 Moreover, a new nomogram has also been developed to further assist in diagnosis. 11
However, it is important to recognize that TT can present with atypical symptoms rather than typical scrotal symptoms, such as abdominal pain only or groin pain caused by TT in the inguinal canal. In cases of such unusual presentations of TT, the time to surgery is often delayed. Notably, in cases presenting with abdominal pain only, a genital examination was not performed at the initial consultation in more than 60% of cases. 12
In fact, differentiating between TT and TATE remains a significant challenge in clinical practice. In cases where it is difficult to distinguish between TT and TATE, surgical exploration via a scrotal incision is often performed to confirm the presence of spermatic cord torsion. While this procedure is generally effective, it is also invasive, and patients and their guardians may hesitate to consent to it because of concerns about its invasiveness. Given that the testicular salvage rate declines with each passing hour in cases of TT, additional tools are necessary to support timely and informed decision-making.
Previous studies have suggested a higher incidence of TT in regions with lower average annual temperatures, implying that meteorological factors may provide useful clues in diagnosing TT. 13 However, these meteorological factors have not been incorporated into the widely used TWIST score. Furthermore, in clinical practice, such factors are rarely considered in decision-making or in discussions with patients and their guardians. This study aims to investigate the association between meteorological factors and acute scrotum by analyzing patients who underwent surgery for acute scrotal conditions, with the goal of improving diagnostic accuracy and clinical outcomes.
Methodology
Study Design and Patients
This retrospective study analyzed patients who underwent surgical exploration for acute scrotum at Nagasaki university hospital between June 2018 and March 2023. The inclusion criteria were as follows: pediatric patients aged 18 years or younger and those who provided consent to participate in the study, either personally or through their guardians. The criteria for exclusion were patients who did not meet the inclusion criteria stated above, as well as those diagnosed with conditions other than TT or TATE following scrotal exploration. Eligible patients with a clearly documented onset time of acute scrotum in their electronic medical records were classified into 3 groups based on the time of onset: 0:00 am to 8:00 am (midnight to morning), 8:00 am to 4:00 pm (morning to late afternoon), and 4:00 pm to 0:00 am (late afternoon to midnight). Among clinical variables, we included demographic variables (age, height, body weight, and body mass index) and clinical presentation variables (laterality of TT or TATE, presence of symptoms such as scrotal pain or erythema) for analysis. Additionally, meteorological data at the time of onset, including maximum, minimum, and diurnal temperature on the day of onset, as well as ambient temperature, atmospheric pressure, and humidity at the specific time of onset, were obtained from the Japan Meteorological Agency database. Seasons were defined as spring (March, April, and May), summer (June, July, and August), fall (September, October, and November), and winter (December, January, and February). The seasonal distribution of TT and TATE cases was analyzed.
Ethics Approval and Informed Consent
This study was approved by Nagasaki university hospital Clinical Research Ethics Committee (Approval No. 23101617, Date: October 24, 2023). Written informed consent was obtained from the patient or their guardians.
Study Outcome
The primary outcome of this study was the difference in seasonal variation and onset time between TT and TATE. The secondary outcome was the difference in meteorological factors, such as ambient temperature, atmospheric pressure, and humidity, at the time of onset.
Surgical Procedure
Surgical exploration was performed by making either a vertical or transverse incision in the scrotum on the affected side. The scrotal contents were then exteriorized through the incision to assess the presence of TT or TATE. In cases of TT, an evaluation of testicular color and blood flow was conducted to evaluate the viability for preservation. Conversely, in cases of TATE, the torsed appendix testis or epididymis was excised.
Follow-up
Postoperative follow-up was conducted in an outpatient setting at 1 week and 6 months after the surgery in both TT and TATE cases.
Statistical Analysis
Categorical variables were presented as percentages. Continuous variables were expressed as mean ± standard deviation (SD) if normally distributed and as median and interquartile range (IQR) if not normally distributed. The normality of the data was assessed using the Shapiro–Wilk test. Continuous variables were compared using Student’s t-test or the Mann–Whitney U test, while categorical data were analyzed using Pearson’s chi-squared test. Trends were assessed using the Cochran–Armitage test. All analyses were performed using JMP Pro for Windows (version 17.2; SAS Institute Inc., Cary, NC, USA), with statistical significance set at p < 0.05.
Results
A total of 53 cases met the inclusion criteria, comprising 31 cases of TT (age range 3-18 years) and 22 cases of TATE (age range 5-18 years). The median age at onset was higher in the TT group than in the TATE group, and significant differences were observed in height and weight between the 2 groups at the time of onset. Physical examination revealed no significant differences in laterality or the presence of scrotal pain between the groups; however, the incidence of scrotal erythema was significantly higher in the TATE group (Table 1).
Clinical Characteristics of Patients With Testicular Torsion (TT) and Torsion of the Appendix Testis or Epididymis (TATE).

Abbreviations: IQR, interquartile range; SD, standard deviation.
From a seasonal perspective, the highest proportion of TT cases occurred in winter (86%), with a clear trend toward an increase in TT cases as winter approached (Figure 1). Both maximum and minimum temperatures on the day of onset were significantly lower in the TT group compared to the TATE group. However, no significant difference was observed in diurnal temperature variation between the groups (Figure 2).

Seasonal distribution rates of testicular torsion (TT) and torsion of the appendix testis or epididymis (TATE). The TT rate was highest in winter (86%) and tended to increase as winter progresses.
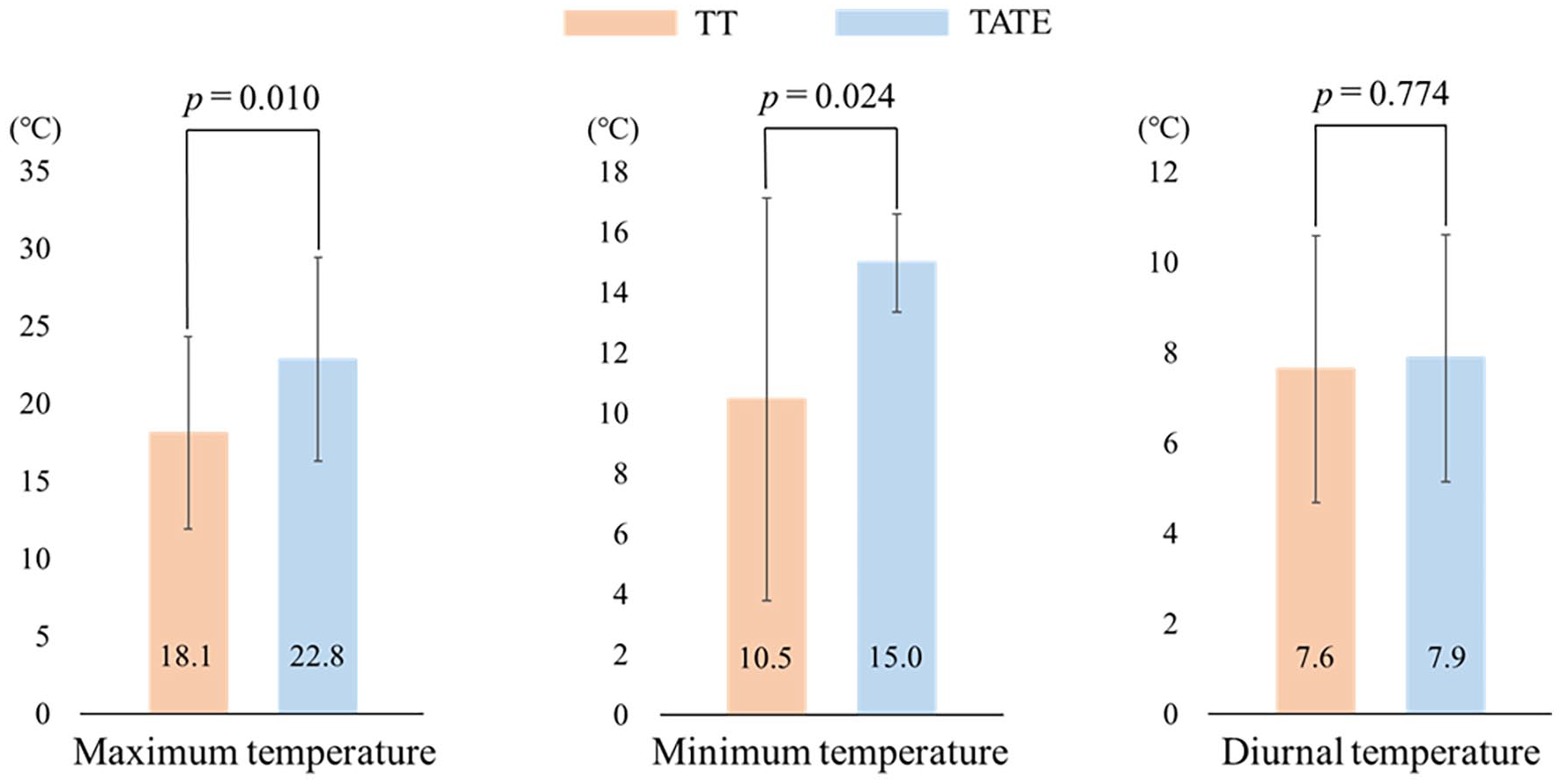
Differences in maximum, minimum, and diurnal temperatures on the day testicular torsion (TT) and torsion of the appendix testis or epididymis (TATE) occurred.
The time of onset was identified in 20 TT and 14 TATE patients. Of the cases occurring between 0:00 am and 8:00 am, the majority (91%) were TT cases, with a clear trend toward an increasing proportion of TT cases as time approached this interval. In contrast, the proportion of TT cases was 50% or less for those with onset outside this timeframe (Figure 3).

Distribution rates of testicular torsion (TT) and torsion of the appendix testis or epididymis (TATE) in the 3 onset time groups. Cases occurring between 0:00 am and 8:00 am were mostly TT and tended to be more frequent.
Regarding meteorological conditions at the time of onset, a significant difference was observed in ambient temperature, while no significant differences were found in atmospheric pressure or humidity (Figure 4).

Differences in ambient temperature, atmospheric pressure, and humidity at the time testicular torsion (TT) and torsion of the appendix testis or epididymis (TATE) occurred.
Discussion
In this study, we found that, compared to TATE, TT occurred at an older age of onset, and the proportion of TT cases among acute scrotum increased as winter approached. Additionally, the ambient temperature at the time of onset was significantly lower in TT cases. It was also observed that the proportion of TT cases was much higher than that of TATE in acute scrotum cases occurring between midnight and 8:00 am.
Previous studies have also reported differences in the age of onset between TT and TATE, with TT being more common in pubertal boys and TATE occurring more frequently in prepubertal boys.14,15 The median age of onset for TT reportedly ranges from 11 to 16 years, while TATE typically occurs between 8 and 11 years,12,14,16 consistent with our findings. A study on the age-specific incidence of TT among young males under 25 years found that the highest incidence rate occurred in the 10 to 14 age group, with 48.25 cases per 100,000 individuals, followed by the 15 to 19 age group at 33.06. 17 One study has also shown that the age group of 12 to 15 years carries a high risk for TT. 2 Although the reasons for the differences in age at onset remain unclear, it has been suggested that the rapid increase in testicular volume during puberty may predispose the testes to rotation, making TT more common during this period. 18 In contrast, vigorous activity or trauma has been proposed as contributing factors for TATE onset. 15
Seasonal variations and ambient temperatures in TT onset have been widely studied, with multiple reports indicating a higher incidence in winter and a greater frequency at higher latitudes compared to that at lower latitudes.19 -24 Lower mean ambient temperatures were also associated with a higher risk of TT. 25 Our results align with these findings, as the proportion of TT cases peaked during winter. This trend was further supported by the significantly lower maximum and minimum temperatures on the day of TT onset compared to that at TATE onset. Similar findings have been reported in recent nationwide studies in Japan. 5 However, some studies have failed to find a seasonal correlation with TT onset.26,27 These discrepancies may be attributable to earlier study periods, smaller sample sizes, and the vast geographical areas of countries such as the United States and Canada, where regional variations in seasonality may exist.
Our study revealed that TT is most commonly diagnosed between midnight and morning, whereas a previous report has shown that TT predominantly occurs between late afternoon and midnight. 28 This difference may be attributed to changes in the sleep habits of Japanese children in recent decades, with later bedtimes and shorter sleep durations becoming more common. 29 It has been suggested that the cremasteric reflex is more likely to occur during sleep in young males, 30 and changes in sleep patterns may explain the shift in TT onset time. Additionally, rising ambient global temperatures due to climate change may also play a role. The study conducted several decades ago 28 reported different meteorological conditions, making it difficult to directly apply those findings to current climatic conditions, where average temperatures have risen significantly. Furthermore, our findings regarding the relationships between ambient temperature, atmospheric pressure, humidity at the time of onset, and the differences between TT and TATE are consistent with the previous report. 14
This study has several limitations. First, it was retrospective in nature. Second, we only included cases with a definitive diagnosis made through surgical exploration, excluding cases of TATE that were diagnosed clinically and managed conservatively. Additionally, the sample size was small, and the appropriate size was neither calculated nor justified. Moreover, the number of cases with precise onset-time data was even smaller. It is also important to note that meteorological conditions vary greatly between regions, limiting the generalizability of our findings. Nevertheless, the trend of increased TT incidence in winter provides valuable information that may be applicable to other regions. Further prospective studies with larger sample sizes are needed to confirm these findings. The collection of region-specific meteorological data will be crucial for a more comprehensive understanding of the relationship between TT onset and environmental factors.
Conclusion
Compared with TATE, TT tends to occur more frequently at colder ambient temperatures, particularly during winter and in the early hours of the morning. Therefore, when evaluating cases of acute scrotum under these conditions, TT should be considered more strongly than TATE as the potential cause. The findings of this study may assist physicians, patients, and their guardians in making informed decisions regarding the management of TT.