
Abstract
Aim:
To glean additional knowledge on children with fever of unknown origin (FUO).
Methods:
Children <18 years old referred to Infectious Disease Service for FUO in a tertiary paediatric hospital were analysed retrospectively from December 2004 to January 2019. Clinical profile, interventions and outcomes were reviewed.
Results:
There were 272 children evaluated (median age 81.5 months, 56.3% males). Causes identified were infections (54.0%), inflammatory (17.3%), haematology/oncological (6.6%), others/unknown (22.1%). The most common infection was typhoid fever. Kikuchi-Fujimoto Disease was the most common inflammatory cause, while haemophagocytic lymphohistiocytosis was the most common haematology/oncological cause. Children ≥ 5 years were more likely to have an inflammatory cause. Cough was associated with infections; mouth ulcers, joint pain and lymphadenopathy with inflammatory disorders. Hepatomegaly, splenomegaly, anaemia and raised C-reactive protein were associated with haematology/oncological conditions.
Conclusions:
We provide insights into knowledge of paediatric FUO and identify clinical associations with infection, inflammatory and haematological/oncological conditions.
Introduction
Fever of unknown origin (FUO) is a diagnostic challenge encountered by paediatricians. Drs Petersdorf and Beesom defined FUO in 1961 as body temperature of ≥ 38.3°C for >3 weeks with failure to establish diagnosis after 3 weeks of inpatient investigation or 3 outpatient visits. 1 Current literature has varied definitions of FUO with the inclusion criteria for fever duration ranging 1 to 3 weeks. It is currently defined as daily fever for ≥38.0°C for ≥8 consecutive days with no apparent cause after initial inpatient/outpatient evaluations.1 -6 This should be distinguished from fever without source (FWS), which is similar to FUO but with a duration of less than a week. 7 The commonest diagnostic groups of FUO are infections, followed by inflammatory and malignant causes. Many diagnoses remain unidentified despite extensive evaluation.
There is no published data on paediatric FUO in Singapore. This study aims to improve knowledge on clinical profile, aetiology and outcomes of paediatric patients referred to the Infectious Disease Service (IDS) for FUO and analyse patterns and associations of symptomatology, physical examination findings and investigations with various diagnostic groups of FUO. It can serve as a guide for general paediatricians in the evaluation and management of children with FUO.
Methodology
The study was conducted in an 830-bed tertiary paediatric hospital in Singapore. We performed a 14-year retrospective review of patients <18 years of age hospitalised at our centre and referred to IDS by a general paediatrician for FUO between December 2004 to January 2019. This study was approved by the Centralized Institutional Review Board. The patients were identified retrospectively from the IDS database. We defined FUO as fever of ≥38.0°C for ≥8 consecutive days with no apparent cause after initial evaluation. We excluded patients with known prior diagnoses of immunodeficiency. The authors have no conflicts of interest to disclose and there has been no financial support for this work that could have influenced its outcome.
We reviewed data for the patients’ clinical characteristics, laboratory and radiological data, diagnosis, treatment and outcomes.
The FUO causes were classified into 4 main diagnostic groups: infection, inflammatory, haematology/ oncological conditions and unknown/others. Statistical analysis was done using SPSS software version 29.0 (IBM, Armonk, New York, USA). Differences between categorical variables were analysed for statistical significance using the chi-square test, and differences between median values across groups were analysed for statistical significance using the Kruskal-Wallis test. P values of <.05 were considered statistically significant.
Results
Demographics
We identified 272 children; 153 (56.3%) male and 119 (43.7%) female. Of this number, 46.7% were Chinese, 23.5% Malay, 16.5% Indian and 13.2% were of other ethnicities. Median age was 81.5 months (interquartile range (IQR) of 36.3-132.0 months). Figure 1 shows the distribution of age groups of children with FUO. Children <5 years formed the largest group in our study (39.0%).

Number of children with FUO in each age group.
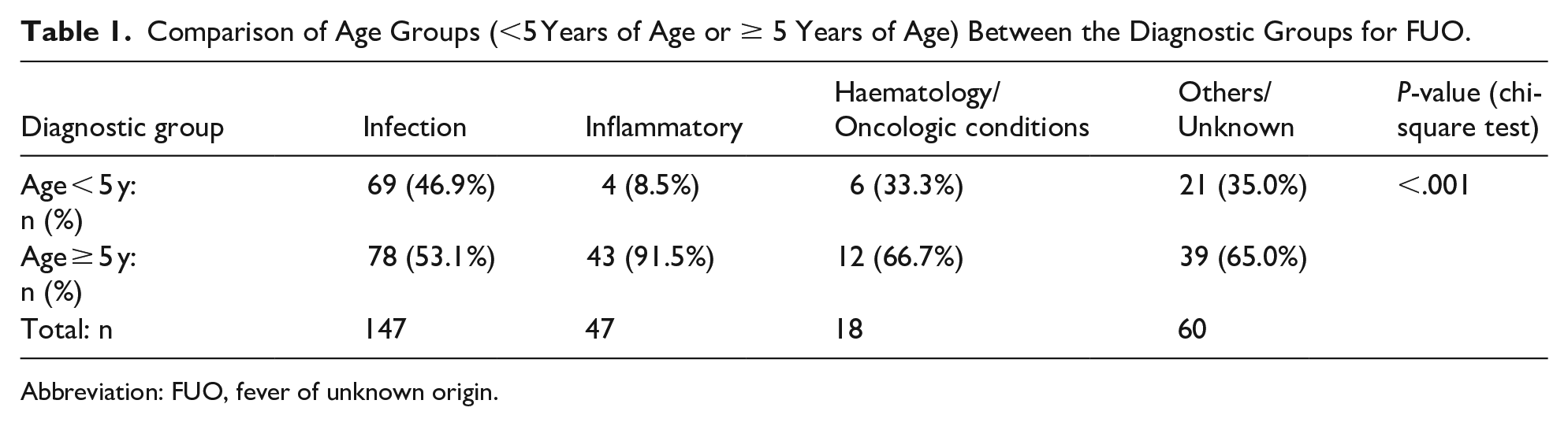
Fever duration before diagnosis ranged from 8 days to 14 months (median of 14.0 days, IQR 12.0-21.0 days). In our study, children ≥ 5 years of age were more likely to have an inflammatory cause of FUO compared to children <5 years of age (P < .001; Table 1).
Comparison of Age Groups (<5 Years of Age or ≥ 5 Years of Age) Between the Diagnostic Groups for FUO.
Abbreviation: FUO, fever of unknown origin.
There were no differences between the diagnostic groups of FUO for gender, race and fever duration (more or less than 14 days).
Presenting Symptoms and Signs
The most common symptoms and physical findings were cough, diarrhoea, rash, oral ulcers, joint pains, lymphadenopathy, hepatomegaly, splenomegaly and arthritis.
Table 2 illustrates the comparison of symptoms/signs between the diagnostic groups for FUO. Cough was more associated with infections (P = .009) whereas mouth ulcers (P = .012), joint pain (P = .004) and lymphadenopathy (P < .001) were associated with inflammatory conditions. Hepatomegaly and splenomegaly were associated with haematology/oncological conditions (both P < .001).
Comparison of Symptoms and Signs Between the Diagnostic Groups for FUO.

Abbreviation: FUO, fever of unknown origin.
Investigations
Table 3 shows a comparison of blood results between the diagnostic groups of FUO. Anaemia and raised C-reactive protein (CRP) were associated with haematology/oncological conditions (P = .03 and 0.017 respectively). Figures 2 and 3 show boxplot comparisons of lowest haemoglobin, and highest CRP respectively between the FUO diagnostic groups. Other laboratory indices were not statistically significant.
Comparison of Blood Results Between the Diagnostic Groups for FUO.

Abbreviations: WBC, white blood cell; Hb, haemoglobin; ANC, absolute neutrophil count; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; ALT, alanine aminotransferase; AST, aspartate aminotransferase; LDH, lactate dehydrogenase; IQR, interquartile range; NS, not significant; FUO, fever of unknown origin.
Highest refers to the highest value during the admission. Lowest refers to the lowest value during the admission.

Boxplot comparisons of lowest haemoglobin counts (in g/dL) between diagnostic groups for FUO.

Boxplot comparisons of highest C-reactive protein levels (in mg/L) between the diagnostic groups for FUO.
Diagnosis
Table 4 shows the frequencies of various diagnoses of FUO across our study.
Shows the Frequencies of Various Causes of FUO.

Abbreviations: FUO, fever of unknown origin; IMS, infectious mononucleosis syndrome; EBV, Ebstein-barr virus infection; CMV, cytomegalovirus infection; HIV, human immunodeficiency virus; NTS, non-typhoidal Salmonella; MAC, Mycobacterium Avium Complex; JIA, Juvenile Idiopathic Arthritis; SLE, Systemic Lupus Erythematosus; HLH, Haemophagocytic Lymphohistiocytosis.
Two patients had 2 overlapping infections concurrently (Mycoplasma pneumoniae and concurrent EBV, Salmonella and concurrent Rickettsia infection).
Twenty-one children had biopsy proven Kikuchi disease.
This child was diagnosed with Evan’s syndrome and treated empirically for febrile neutropaenia with no organism found.
Opportunistic infections included CMV. Clostridium difficile, Mycobacterium avium complex (MAC).
Fifteen out of 20 patients were found to have Mycoplasma pneumoniae pneumonia in the chest infection group.
Specific Infections
Table 4 illustrates the distribution of infections and pathogens. Viral infections comprised only 12.1% of FUO, while bacterial infection was most common (36.8%). The bacterial causes largely comprised of typhoid fever, non-typhoidal Salmonella (NTS; n = 28) and scrub typhus. Typhoid fever was diagnosed through positive Widal-Weil Felix serologies and/or positive blood culture results. Many of our patients with typhoid fever, NTS and scrub typhus had a positive travel history to neighbouring countries. For patients with typhoid fever, 66.7% had travelled recently, mainly to India, Indonesia and Myanmar. While for patients with scrub typhus, 38.5% had recently travelled to neighbouring countries including India, Sri Lanka and Indonesia. One of the patients with NTS (16%) had recently travelled to Malaysia. Mycoplasma pneumoniae comprised a large proportion of chest infections referred for FUO (75.0%). Tuberculosis (TB) caused 8.2% of infective FUO. Of the viral causes, infectious mononucleosis syndrome (IMS) comprised half (48.5%) of viral causes while the other half were due to Human immunodeficiency virus (HIV) infection with opportunistic infections (OI), and prolonged identifiable viral illnesses.
All patients with infective endocarditis (IE) had underlying congenital heart disease (CHD) indicating that IE should be strongly suspected in FUO children with CHD and vice versa. In our centre, it is routine for all patients with a clinical suspicion for IE to obtain a full evaluation with an echocardiogram evaluating for CHD.
Rheumatological/Inflammatory Conditions
Inflammatory causes were diagnosed in 47 patients (17.3%). Majority were diagnosed with KFD (21 children). All patients with formal diagnosis of KFD were diagnosed with histopathology on lymph node biopsy. The cases of suspected KFD with no lymph node biopsy were classified under others/ unknown conditions (see below). The second largest group was Still’s disease (13 children).
Haematology/Oncological Conditions
Eighteen patients (6.6%) were diagnosed with haematology/oncological conditions. Seven of these children were diagnosed with HLH based on international diagnostic guidelines (2.6%). Six patients had haematologic malignancies (4 had leukaemia and 2 had lymphoma). Infectious triggers of HLH included EBV (3) and adenovirus (1). There were no cases of familial HLH or macrophage-activation-syndrome.
Others/Unknown
There were 60 children with no conclusive diagnosis. A description of the cases included in the unknown/others group is illustrated in Table 4. Presumed KFD that were not biopsy proven were included in this category; all responded to a trial of indomethacin/anti-inflammatory medications.
Deaths
There were 4 (1.5%) patients that demised directly related to the cause of FUO. Two patients died from HLH and 2 patients with severe combined immunodeficiency (diagnosed during FUO evaluation) demised from overwhelming sepsis.
Discussion
This is the largest study investigating aetiology, clinical characteristics and outcomes of paediatric FUO in Singapore over 14 consecutive years. Although infections comprised most of FUO causes, there is a shift of diagnoses in current literature to undiagnosed or inflammatory aetiologies due to widely available and faster diagnostic testing for infections. In our study, majority of cases were still infections (54.0%) followed by unknown/other causes (22.1%), inflammatory (17.3%), and haematology/oncological causes (6.6%). Similarly, a systematic review by Chow and Robinson of 1638 children across 18 studies (developing and developed countries) showed that the causes for FUO were distributed as follows: infection (51%), no diagnosis (23%), miscellaneous non-infectious conditions (11%), collagen vascular disease (9%), malignancy (6%). 5 This study defined FUO as fever for >1 week (same as our study). Antoon et al described paediatric FUO in the United States as approximately 50% infective, 10% to 20% collagen vascular disease, and 10% oncologic. 6 A recent single-centre study in Turkey found 40% of paediatric FUO to be infectious, the most common of which was tuberculosis (23%) and followed by inflammatory causes (33%) and malignancy (16.9%). 8 This suggests that our pattern is consistent with worldwide statistics. Interestingly, a recent study in Egypt found a slightly higher incidence of FUO due to collagen vascular diseases (30.9%) than infections (28.2%), though the authors postulate this may have been affected by the fact that 85% of patients received antibiotic treatment prior to hospital presentation. 9
Cho et al and Chien et al’s studies in Taiwan showed 20% to 30% infections, undiagnosed 15% to 20%, malignancy 15% to 20%, collagen vascular diseases 15%. Notably, malignancies were higher in proportion compared to ours.4,10 These 2 studies, however, defined FUO as temperature of ≥38.0°C for >2 weeks and >3 weeks respectively. Our study indicated 54.0% infective cases, about twice their number. We postulate that more stringent definitions on fever duration (extending it to >2 weeks) could sieve out more infectious cases.
Of infections identified, most of our patients had eventual diagnoses of bacterial sources. We have high rates of typhoid fever, NTS and scrub typhus. Many of our patients with typhoid fever, NTS and scrub typhus had a positive travel history (typhoid fever 66.7%, scrub typhus 38.4%, NTS16%). This reflects the burden of travel-related illnesses in Singapore. Mycoplasma pneumoniae pneumonia comprised 75% of pneumonia referred for FUO. Although viruses were less common, half the cases comprised of IMS, majority being EBV-related. All other viruses identified could be detected with nasopharyngeal aspirate (NPA) for respiratory virus multiplex polymerase chain reaction (PCR).
Tuberculosis (TB) was found in only 4.4% of our study of FUO, 8.2% of infections. In studies done in China (Shi et al) and Taiwan (Chin et al) respectively, TB was the most common cause of infection for FUO; approximately 20% of all cases.11,12 Our smaller numbers of TB may reflect a lower incidence of TB in Singapore via containment measures. Contact tracing is likely more feasible in Singapore due to our small population. However, TB is still a relevant cause and should be evaluated if patients fit the clinical spectrum.
We suggest a reasonable initial infective screen for FUO could comprise of blood cultures, EBV serology, NPA for respiratory virus multiplex PCR and rickettsia serology. Urinalysis with cultures and a chest radiograph should also be considered. An association with infection in FUO is presence of cough, as illustrated in our study. This was similar to Kim et al’s study where respiratory symptoms were more prominent in the infective group. 13 Positive travel history is an important risk factor for typhoid fever, NTS and scrub typhus in Singapore. We found that many of our patients with typhoid fever had a positive travel history (66.7%, similar to a Singapore paper published in 2016 where 94% of children admitted for enteric fever in Singapore from January 2006 to January 2012 had travelled to typhoid-endemic countries. 14 As for typhus, if it is endemic, or possibly travel-related, the evaluating physician could consider presumptive treatment for typhus based on clinical presentation as rickettsia serology has a long turnaround time.
All patients diagnosed with IE had underlying CHD. This is congruent with Liew et al’s paper which observed 88.9% of IE in childhood associated with underlying CHD (48.0% had FUO). 15 Clinicians should have a strong suspicion for IE if the child with FUO has an underlying CHD; similarly, all patients diagnosed with IE should be evaluated for CHD.
Our study showed that joint pain, oral ulcers and lymphadenopathy were associated with inflammatory/ rheumatological conditions. This was also reflected by Kim et al where arthritis and lymphadenopathy were more predictive of connective tissue disease and necrotising lymphadenitis (P < .001). 13 We have a high rate of patients with KFD (21 cases, 7.7%). Our percentage of patients with KFD was similar to Kim et al’s study (8%). 13 In a study conducted by Selvanathan et al 24.5% of patients admitted for KFD presented with FUO, with median fever duration of 10 days. 16 Hence, the diagnosis of KFD should be strongly considered in FUO patients with significant painful lymphadenopathy.
Other inflammatory causes included Still’s disease, lupus and Kawasaki disease (KD). We note a low incidence of KD in our population (1.1%), in comparison with other studies: Cho et al and Mahmoudi et al reported KD at 11.9% and 7.4% of paediatric FUO respectively.4,17 Tan et al described the estimated incidence of KD in Singapore at 51.4 per 10 000 children <5 years of age (one of the highest outside Japan). 18 The low incidence of KD in our population causing FUO could be due to a high index of suspicion in our centre as even cases of atypical KD would be detected and managed by general paediatricians without need for IDS referral.
There were 11 patients with malignancy and 7 patients with HLH. Malignancies are reported in only a small percentage of FUO in most studies,1 -6,19 and this was similarly reflected in our study with leukaemia and lymphoma cases accounting for most of them. HLH is a unique disease presenting its own diagnostic challenges with associated high morbidity/ mortality rate. Watts et al described fever in 100% of HLH and splenomegaly in 46.0% of HLH. 20 In our study, splenomegaly and hepatomegaly were associated with haematology/oncological causes of FUO (both P < .001).
Despite extensive investigations, no clear cause was identified in 22.1% of the children in our study. Approximately half were due to presumed prolonged viral illnesses which were self-limiting. Eight were due to presumed KFD, wherein lymph node biopsy was not performed but all responded to empiric treatment with indomethacin. As it is a self-limited illness, clinicians may consider a trial of indomethacin in children with suspected KFD but who decline cervical lymph node biopsy, and they require close follow up to ensure fever lysis and resolution of lymphadenopathy.
Most children had fever resolution with treatment of their condition. Majority of paediatric literature recommend that empiric antibiotics are not indicated as it may obscure diagnosis. Although many patients had unidentified causes of FUO, most were reported to spontaneously improve or resolve without treatment. 10 Similarly, we have observed this in about half of our unknown causes of FUO which were due to presumed prolonged viral illnesses. Exceptions may be the use of non-steroidal anti-inflammatory medications that could help discern infectious from non-infectious arthropathies, 21 which we also have found useful in our cases with KFD.
Death occurred in 4 out of 272 of our patients (1.5%), with 2 deaths from HLH and 2 deaths from newly diagnosed SCID with sepsis. While mortality is low, it is important to identify HLH and immunodeficiency given that deaths occurred in these 2 categories. Our cases with unknown/unspecified causes of FUO had good outcomes with a self-limited course of pyrexia. This was also reflected in other studies such as in Chow et al’s and Kim et al’s of which all patients in the no diagnosis group had resolution with no sequelae.5,13
Attention to uncovering exposures, symptoms, signs or laboratory findings is the most fruitful approach to FUO. Even if FUO remains undiagnosed, most cases still have good outcome, as illustrated by our study. This is in contrast with studies on adult FUO where outcomes are less favourable due to differences in causes, with more malignancy identified.6,22
Limitations in our study include: (1) Constraints in data collection from retrospective records, (2) Potential selection bias as only inpatient cases referred to IDS were included, (3) Comparison with other studies with varying definitions of FUO required detailed examination of their methodology, 4. This is a single tertiary-centre retrospective study, and sample size calculation was not performed.
Nonetheless, the study provides insights into knowledge of paediatric FUO, and associations with infection, inflammatory and malignant or haematological conditions. It serves as a guide for further research and clinical practice, emphasising the need for ongoing studies to evaluate FUO patients over their lifetime.
Conclusion
This study describes the common symptoms, physical exam findings and investigations as well as the frequencies of different causes of FUO in children in Singapore. Symptomatology, physical examination and first-line investigations can help elucidate the likely cause of paediatric FUO and guide further evaluation and treatment.