
Abstract
A 33-year-old man was referred to our hospital with chief complaints of fever, dizziness, and headache. Although he had recurring fever and dizziness for 7 months, neurological examination, magnetic resonance imaging, computed tomography, electrocardiograms, and blood tests were normal. He was diagnosed with functional hyperthermia, cervical vertigo, and tension headache and was treated with oral medication and physical therapy. After treatment, the dizziness and headache resolved; however, the fever and anxiety did not. During follow-up, he noticed differing results from different electronic thermometers. The physician decided to use an accurate analog thermometer, a gallium thermometer, in combination with the other thermometers. The results differed significantly among the thermometers, and the electronic thermometer readings were found to be inappropriately high. The physician made a diagnosis of pseudo-fever, and the patient recognized that the gallium thermometer’s results were the most accurate reflection of his physical condition, resolving his anxiety.
Keywords
Introduction
In Japan, axillary body temperature measurement is generally used in clinical practice and can be an index of core body temperature when recorded correctly: (1) close the axilla completely, (2) take the temperature reading at least 10 min after the axillary temperature gradient reaches thermal equilibrium, and (3) take the measurement at the correct site. 1 Extremely accurate mercury thermometers, which are based on the principle of mercury expansion, have long been used. However, the Minamata Convention on Mercury and the Act on Preventing Environmental Pollution of Mercury prohibited the manufacture, import, and export of mercury thermometers after 1 January 2021; 2 currently, clinical temperature monitoring is generally performed with predictive electronic thermometers. 3 When used in the axilla, the latter have large errors, and the results are reportedly significantly higher than actual temperatures of electronic thermometers’ actual mode or of the mercury thermometers; the mean difference was approximately 0.1°C, whereas the frequency distribution of the difference showed that 26.3% of the differences was ⩾0.3°C. 4 Gallium thermometers have replaced mercury thermometers as analog thermometers and have been available in Japan since January 2021. Galinstan (Ga-In-Sn alloy; 68.5% gallium, 21.5% indium, and 10% stannum), which is used as a substitute for mercury, has lower toxicity and a higher boiling point than mercury, making it safer than mercury. Gallium thermometers are more accurate than other body temperature measurement devices. 5
Anxiety about fever has been observed worldwide as fever phobia, caused by patients’ easy access to thermometers outside the medical institution. 6 Other popularized healthcare devices such as blood pressure and oxygen saturation monitoring devices, weighing scales, and portable electrocardiographs can cause anxiety in patients when used without caution. 7 Furthermore, patients with a history of anxiety are about twice as likely to have a medical visit that is considered inappropriate. 8 Therefore, physicians should appropriately manage patient concerns related to various popularized healthcare devices. 7
We report the case of a patient whose fever did not subside despite the resolution of symptoms and who reported anxiety due to the inconsistency in the results of multiple predictive electric thermometers, which led to the combined use of a gallium thermometer showing no fever, thus resolving the patient’s anxiety.
Case
A 33-year-old man was referred to our hospital with chief complaints of fever, dizziness, and headache. Seven months prior, he visited a primary care clinic for a fever of 38°C, testing negative for C-reactive protein and coronavirus disease 2019 (COVID-19), and his symptoms spontaneously remitted. One month later, he developed fever and dizziness and visited a neurologist; however, no neurological problems or head magnetic resonance imaging abnormalities were found. Subsequently, he repeatedly had a fever of approximately 37°C; hence, he visited a general hospital 2 weeks previously. However, no abnormalities were found in blood test results, electrocardiogram, and head computed tomography; thus, the cause of his fever was unclear. On his first visit with us, he had mild fever, dizziness, and headache; his vital signs (outside of body temperature) were stable (axillary body temperature, 37.0°C; blood pressure, 123/72 mm Hg; pulse, 76 beats/min), and blood tests showed no abnormalities (Supplemental Table S1). The patient was diagnosed with functional hyperthermia, cervical vertigo, and tension headache and treated with eperisone hydrochloride, keishikajutsubuto (Japanese Kampo medicine), and physical therapy. After treatment, the dizziness and headache stopped; however, the fever and anxiety did not resolve completely.
When the physician instructed the patient to record his body temperature at home and conducted a follow-up, the patient reported different readings on predictive electronic thermometers from different manufacturers (MC-681, OMRON Healthcare Co., Ltd., Japan; C232, TERUMO Co., Ltd., Japan; Supplemental Figure S1). Considering the differences between the prediction algorithms of these thermometers, we decided to use an analog thermometer—a gallium thermometer (IX-101L, OnSQUARE Co., Ltd., Japan) (Supplemental Figure S1)—in combination with the other thermometers. The results showed a significant difference between the two predictive electronic thermometers and the gallium thermometer (Figure 1). By comparing the results of temperature measurements with the physical condition, the patient recognized that the gallium thermometer results were the most accurate reflection of his physical condition, and his anxiety related to fever resolved. Nine months after the introduction of the gallium thermometer, the patient had no health problems, and he rarely used the gallium thermometer.

Mean body temperature of the patient using each thermometer (n = 497). Between 16 October 2021 and 5 February 2022, temperatures at home or at work with a gallium thermometer and two electronic thermometers measured at approximately the same timing were recorded 497 times by the patients themselves. Statistically significant differences: p < 0.01, repeated-measures ANOVA and p < 0.01, paired t-test with Bonferroni’s correction. Predictive electronic thermometer A, MC-681; Predictive electronic thermometer B, C232; Gallium thermometer, IX-101L.
Discussion
This case report includes two significant takeaways. First, the use of sensitive thermometers should be considered in patients with a fever of unknown origin. With the COVID-19 global pandemic, daily measurements of body temperature have increased. 9 Considering the widespread use of predictive electronic thermometers, 3 we believe there are several cases of predicted body temperature differing from actual body temperature. To prevent infection spread, work and social activities can be restricted when the patient has a fever. Therefore, physicians can contribute to alleviating patient anxiety and social burden using sensitive thermometers, such as gallium thermometers, to obtain accurate body temperatures. Considering the possibility that the predictive electronic thermometers used by our patient may have deteriorated, we compared them with new thermometers of the same model, finding that one of them had a large difference in the results (Figure 2). Generally, the service life of predictive electronic thermometers is approximately 5 years; however, recognizing that the accuracy of the thermometer is compromised is not easy for patients. Gallium thermometers are inexpensive, accurate, 5 and easy to use, even for elderly people who are familiar with mercury thermometers, without the need to consider electronic problems or battery failure.
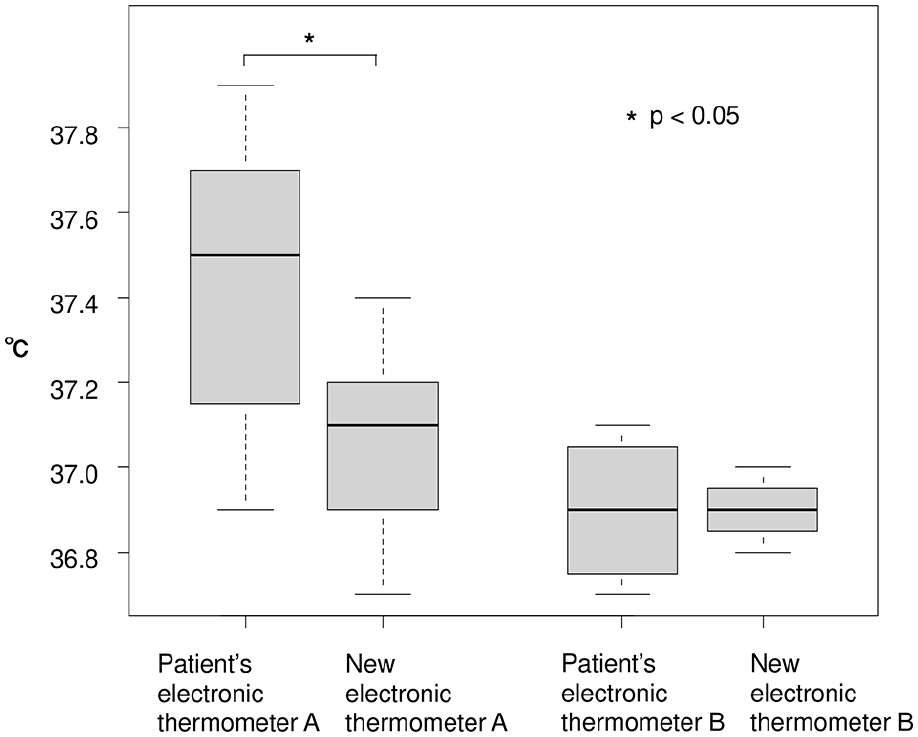
Comparison of patient’s thermometers with new thermometers of the same model. Approximately 3 months after the gallium thermometers were introduced, axillary temperature comparisons of each thermometer were performed for both the left and right axilla at the hospital. Statistically significant differences are observed in the comparison of thermometer A (p < 0.05, Wilcoxon’s rank sum test with continuity correction; n = 8). No statistically significant difference was observed for thermometer B (n = 4). Predictive electronic thermometer A, MC-681; Predictive electronic thermometer B, C232.
Second, it is crucial that physicians properly manage patient anxiety caused by medical device measurements, such as body temperature. The patient visited our hospital with fever as a chief complaint. Fever is a common symptom in both rural 10 and urban areas. 3 Since fever causes anxiety in patients and in the parents of children, 6 it is a significant factor in increased physician visits. Anxiety caused by medical information is not limited to information from popularized devices such as body thermometers and blood pressure and oxygen saturation monitoring devices; it further includes information on the Internet. 7 Thus, with the development of technology, physicians should be aware that information from easy-to-use and popularized devices can trigger anxiety in patients. 7
Conclusion
In conclusion, for patients with fever of unknown origin, an accurate thermometer, such as a gallium thermometer, may be useful in clinical practice. Physicians should recognize the inaccuracy of medical devices and listen to the patients’ concerns regarding the use of medical devices and appropriately handle them.
Supplemental Material
sj-docx-2-sco-10.1177_2050313X221129772 – Supplemental material for Pseudo-fever caused by predictive electronic thermometers: A case report
Supplemental material, sj-docx-2-sco-10.1177_2050313X221129772 for Pseudo-fever caused by predictive electronic thermometers: A case report by Hiroki Maita, Tadashi Kobayashi, Takashi Akimoto, Hiroshi Osawa and Hiroyuki Kato in SAGE Open Medical Case Reports
Supplemental Material
sj-tiff-1-sco-10.1177_2050313X221129772 – Supplemental material for Pseudo-fever caused by predictive electronic thermometers: A case report
Supplemental material, sj-tiff-1-sco-10.1177_2050313X221129772 for Pseudo-fever caused by predictive electronic thermometers: A case report by Hiroki Maita, Tadashi Kobayashi, Takashi Akimoto, Hiroshi Osawa and Hiroyuki Kato in SAGE Open Medical Case Reports
Footnotes
Acknowledgements
The authors thank the patient who approved this report.
Author contributions
H.M. conceived the idea and wrote the original draft of the manuscript. T.K. and T.A. developed the theory of this report. All authors discussed the case and commented on the manuscript. H.M., T.K., and T.A. revised and edited the manuscript. All authors provided final approval before submission of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Data availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.