
Abstract
We sought to describe the clinical, radiological characteristics and determine the outcomes of children with primary headache. A retrospective observational study was conducted. Children with primary headache were recruited. Demographic, clinical and radiological data were compiled. Visual Analog Scale was used to determine pain severity. Seventy-three patients were included in the study. Their median age was 10.0 (IQR: 8.0-12.0) years, and 38 (52.1%) were female. Fiftyfour (74.0%) had migraine headache. Majority, 50 (68.5%) reported severe headaches at presentation. Three (4.1%) patients had abnormal findings on MRI while 5 (6.8%) patients had abnormal findings on EEG. Most participants were pain free at 3 and 6 months follow up. Most used prophylactic agent was sodium valproate (84.0%).
Introduction
Headache is an important cause of morbidity in children and adolescents globally.1,2 The International Headache Society defines primary headache as a disorder not resulting from biological structures of the brain and not caused by or attributed to other disorders. 2 The major groups of primary headache disorders include migraine, tension type headache and trigeminal autonomic cephalalgias. Primary headache disorders represent 54.4% of childhood headache presentations. 3
Migraine is the most common primary headache diagnosis in children.4,5 The prevalence of migraine increases from 3% in children age 3 to 7 years to 4% to 11% in age 7 to 11 years and 8% to 23% in adolescents. 6 In children, migraine and tension type headache often occur together and are mostly episodic. Trigeminal autonomic cephalalgias are very rare in children and adolescents. 6 The Global Burden of Disease study 2010 identified migraine as the seventh disabler among 289 diseases in terms of years of life lost to disability.7,8 In children, migraine and other primary headache disorders cause a substantial negative impact on physical and mental health as well as on school performance and quality of life. 8 An Austrian study on quality of life of children and adolescents with migraine showed reduced quality of life in the areas of physical, socio-economic and school functioning. 8 Children with headaches have lower school functioning and emotional functioning than children with other chronic illnesses. 9 Migraine is also associated with a number of co-morbidities such as atopy, sleep disorders, emotional and behavioral problems, depression and anxiety. 8 There is moderate quality evidence that suggests that the presence of comorbid negative emotional states in children is associated with increased risk of headache persistence. 10 Frequent pain in childhood is a risk factor for chronic pain as an adult. 11 The most common headache triggers include stress, fatigue, sleep disturbances, prolonged exposure to excessive sunlight or heat and hunger. 10
The clinical diagnosis of primary headache is based on the International classification of headache disorders 3rd edition. 2 A study in North Jordan by Al Momani et al 5 found migraine to be the most common primary headache with 40% presenting with severe headache, 34.5% had daily headaches and 78.9% had bilateral headaches. An Italian study also found migraine to be the most common headache type and 46.7% had positive family history. 12
Most primary headache disorders can be diagnosed without diagnostic testing using comprehensive history and a focused physical and neurologic examination. In patients with headache and normal neurological examination, important vascular and neoplastic unexpected findings are rare and are better detected with Magnetic Resonance Imaging. The overall prevalence of unexpected findings and normal variants was found to be low in studies using MRI only.13,14
The management of primary headache constitutes a multimodal program including lifestyle modification, psychotherapeutic interventions, pharmacotherapy and complementary measures. 15 Aerobic exercise can decrease pain intensity, frequency and duration of migraine and can also increase quality of life. 16 Migraine is episodic and requires both acute and preventive treatment for better outcome. Commonly used medications for migraine include non-steroidal anti- inflammatory drugs (NSAIDs), anti-dopaminergics, antihistamines, antidepressants, antihypertensives, antiseizure medications like levetiracetam and sodium valproate, triptans, dihydroergotamines, gepants, nutraceuticals such as vitamin B2, Coezyme Q10, magnesium.17,18 The goal of preventive treatment is to reduce headache frequency and disability associated with recurrent pain. The Childhood and Adolescent Migraine Prevention (CHAMP) trial found a high placebo response rate that was similar to other previous headache trials. 19 The findings suggest that effective treatment models used in adults may not be similarly effective in pediatric population. The treatment of acute migraine remains a therapeutic challenge in many emergency departments.
Headache is underestimated, under recognized and undertreated throughout the world. In low and middle-income countries, outcomes are poorer due to limited access to drugs and appropriate interventions, significantly limiting the quality of life of children with primary headache. The structures for providing quality care for children and adolescents with headache disorders are not adapted to suit their needs.
Our study describes the presentation and outcomes of childhood primary headache in the Kenyan context. This data set contributes to the understanding of management and outcomes of primary headache in this setting.
Methods
We conducted a retrospective observational study to describe the clinical, radiological characteristics and outcomes of primary headache among children aged between 3 and 18 years. The study was conducted at a tertiary hospital between October 2022 and May 2023. All medical records of children seen at the pediatric neurology clinic between January 1, 2015 and December 31, 2020 were reviewed to identify eligible participants for the study. We conducted an electronic search of the hospital patient records database (

Study participants recruitment flow chart.
Statistical Analysis
De-identified data were verified and entered into a secured RedCap. Data were analyzed using Statistical Package for Social Sciences (SPSS) version 23 statistical software. The variables were age, gender, Body Mass Index, pain severity, pain location, pain duration, precipitating factors, MRI and CT scan abnormality, EEG findings, family history, comorbidities and pharmacotherapy use. Quantitative variables were summarized as means and standard deviation and categorical variables were summarized as frequency and percentages. Data were reported in tables and graphs at baseline, 3 and 6 month categories.
Ethical Considerations
This study was approved by the Institutional Ethics and Review Committee (approval number 2022/ISERC-83 v2). The ethics committee waived the need to obtain consent for collection, analysis and publication of the retrospectively obtained and anonymized data for this observational study. Patient medical information was collected, data was de-identified and stored in a secured database.
Results
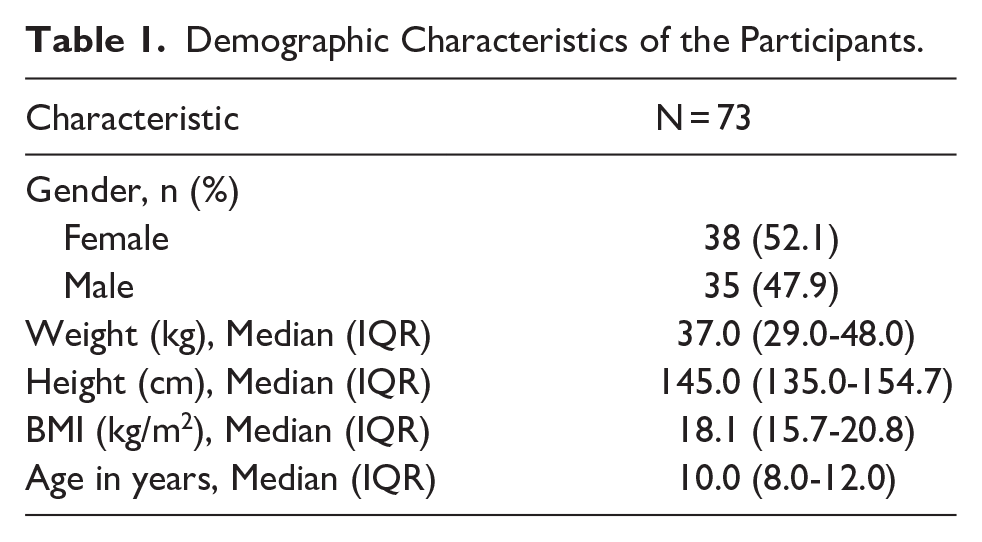
A total of 73 records of children with primary headache were included. They were of median age 10.0 (IQR: 8.0-12.0) years and 38 (52.1%) were female (Table 1).
Demographic Characteristics of the Participants.
Of the participants enrolled in the study, 54 (74.0%; 95% CI: 62.8-83.8) were diagnosed with migraine headache. The pain was most common in bilateral, temporal and frontal location as reported by 35 (47.3%), 32 (43.2%) and 28 (37.8%) respectively.
Majority, 50 (68.5%) reported severe headaches and 45 (61.6%) did not have known precipitating factors. A positive family history of headache disorders was reported by 34 (46.6%) participants.
Most participants 61 (83.6%) had headache episodes of unquantified duration, 2 had headache episodes lasting less than 1 hour, 7 had headaches lasting 1 to 72 hours, 3 had headaches for a duration of more than 72 hours. Of the participants who reported attack frequency, 16 (21.9%) had daily headaches, while 19 (26.0%) reported attack frequency of 2 to 4 days and 7 had headaches once per week. The attack frequency was not reported in about 42.5% (n = 31) of the participants. Sleep disorders were the most common comorbidity as reported by 24 (32.9%) participants. This data is presented in Table 2.
Clinical Characteristics of Participants.

For those who had imaging done, only 3 of 38 (4.1%) participants had abnormal MRI findings (1 with unremarkable-incidental isolated absent septum pellucidum and 2 unremarkable-incidental mega cisterna magna). No abnormalities were noted on CT scan. Five of 61 children had abnormal EEG findings, (generalized spike and wave, generalized spike and wave occurring once, polyspikes and spike and wave discharges, generalized spike and wave with bi-anterior dominance). This data is summarized in Table 3.
Radiological and EEG Characteristics of Participants.

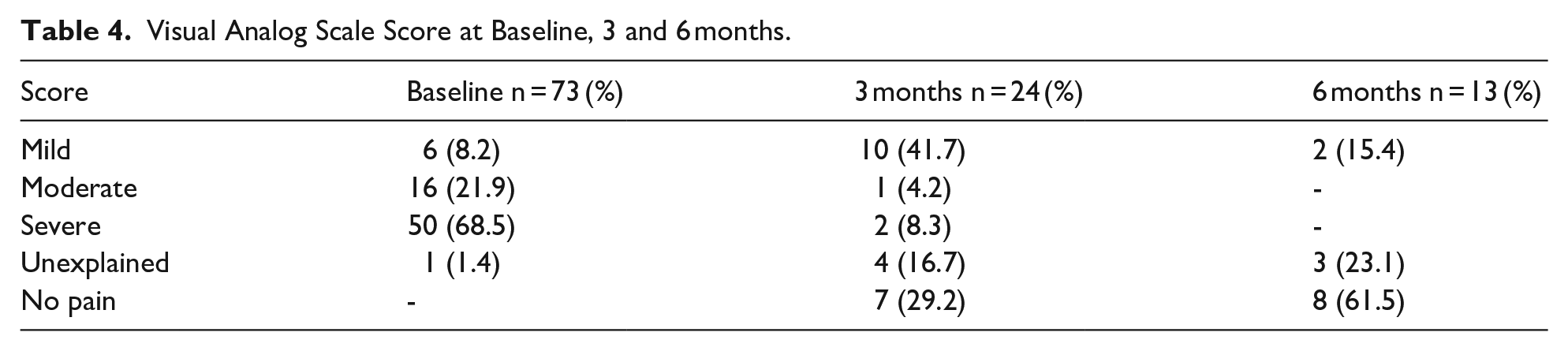
There were 24 (32.8%) participants on follow up at month three after initial review. The majority 16 (64.0%) of the participants were pain free. Records of only 13 (17.8%) children were available at 6 months follow up. About 9 (64.3%) of them were free of pain. VAS score at baseline was mild in 6 (8.1%), moderate in 16 (21.6%) and severe in 51 (68.9%). This data is presented in Table 4.
Visual Analog Scale Score at Baseline, 3 and 6 months.
At baseline the most commonly used abortive pharmacotherapy was paracetamol (57.5%, n = 42). Sodium valproate was the most common drug used for prophylaxis as reported by 21 (87.5%) at 3 months and 11 (84.6%) at 6 months. This data is summarized in Table 5.
Pharmacotherapy Use at Baseline, 3 and 6 months.

Only 2 of the participants followed at 3 months missed school, 12 (50.0%) did not have any comorbidity and 4 (16.6%) had learning difficulties. At 6 months follow up, 10 (76.9%) had no comorbidity while 2 (15.4%) had learning difficulties.
Discussion
In this retrospective observational study, we describe the clinical, radiological characteristics and outcome of primary headache among children aged between 3 and 18 years. The mean age was 10 years and the most common primary headache type was migraine. Most children 50 (68.5%) had severe headache at presentation, and the most common location was bilateral 35 (47.3%) and nausea was the most common symptom accompanying headache. A significant proportion of the children 34 (46.6%) had positive family history of headache disorders.
These study findings are similar to other studies among children that show a higher prevalence of migraine than tension type headache.5,20 Migraine headache has a genetic etiology and most children with migraine have a positive family history. In our study, about half of the participants reported a positive family history for headache (46.6%) which is similar to an Italian study done among adolescents. 12 A study in Romania using polysomnography found a positive correlation between migraine and sleep disorders and in our study, sleep disorders was the most common comorbidity (32.4%) reported at baseline. 21 The diagnosis of primary headache is clinical and detailed evaluation is critical to avoid unnecessary and expensive investigations. In our observation, 4.1% had abnormal incidental findings on MRI brain and no abnormal findings were found on CT scan. These numbers are lower than other studies and supports the current guidelines to avoid imaging in patients with primary headache and when such imaging is required then MRI is preferred. 22 The management of primary headache involves a multimodal approach that includes lifestyle modification, psychotherapeutic interventions, pharmacotherapy and complementary measures.17,23,24 A recent double blinded CHAMP trial showed no significant differences in reduction in headache frequency or headache related disability in children with migraine taking amitriptyline, topiramate or placebo. 19 In our study, most participants used sodium valproate and about two-thirds were pain free at 3 and 6 months, respectively. VAS scores overall showed a significant improvement at 3- and 6-months post treatment. Access to newer and safer prophylactic agents remains limited in our setting due to high costs hindering their utilization as therapeutic options. Psychotherapy and behavioral therapies in chronic migraine are locally available but not readily accessible and many families drop off after 1 or 2 sessions due to high costs. In addition, analyzing the benefits of such therapeutic options in our setting is difficult.
Overall, our study provides significant insights on the clinical presentation and outcome of primary headache among children. Early identification and intervention of primary headache disorders in pediatric population is important to improve quality of life of children with headache. This is the first study in Kenya that investigated the clinical and radiological patterns of children and adolescents with primary headache. There are however some limitations to the study. First, the information obtained was limited to the data found in the patients’ files. Secondly, the study was conducted in a single center which is a tertiary hospital and might not be representative of the general pediatric population. Further studies with larger sample size should be conducted.
Conclusion
In our study, migraine was the most common primary headache. Detailed clinical history and physical examination is necessary for diagnosis and avoids unnecessary and costly investigations. Severe disability can be prevented by use of proper prophylaxis. There are substantial challenges to accessibility of newer and safer therapeutic options in our setting. This requires significant investment to include such medicines in the essential list of drugs. Where resources are limited, sodium valproate and other therapeutic options can be chosen to alleviate pain and reduce disability in children suffering from primary headache.