
Abstract
Dermatofibrosarcoma protuberans (DFSP) is a rare, slow-growing soft tissue sarcoma of the skin, representing less than 1% of all soft tissue sarcomas. Clinically, it is characterized by its indolent nature, localized growth, and low-grade malignant fibrosarcoma features. Here, we present a case of a 40-year-old woman diagnosed with DFSP carrying a deletion in the SMARCA4 gene. Following complete tumour resection, no recurrence or new malignancies were observed during the 1-year follow-up period. To our knowledge, cases of DFSP with SMARCA4 gene deletions have not been previously documented in the literature. This case contributes to our understanding of the molecular mechanisms underlying DFSP in soft tissue sarcomas, potentially enhancing clinicians’ ability to accurately assess patient prognoses.
Introduction
Dermatofibrosarcoma protuberans (DFSP) is a localized, low-grade, malignant fibrosarcoma of unknown etiology. DFSP is most common among dermal sarcomas, with an annual incidence of 0.8% to 4.1% per million population. The histopathological features of DFSP include fibroblasts arranged in a storiform pattern and an often irregular tumour shape. 1 The clinical, histopathological, and immunohistochemical characteristics of DFSP are typical, although molecular features such as the deletion of the SMARCA4 gene in this case are rare and have not been previously reported. The SMARCA4 gene, located on chromosome 19q13, encodes the BRG1 protein, a subunit of the catalytic heterodimer of the SWI/SNF chromatin-remodelling complex. Wang et al. discovered varying degrees of deletion of SWI/SNF complex subunits in different types of tumours, indicating their role as tumour suppressor genes in tumourigenesis and development. 2 Tumours with deletion of SWI/SNF complex subunits show a certain correlation with the site of tumourigenesis. Loss of SMARCA4 expression is common in hypercalcemic small cell carcinoma of the ovaries in young women. 3 Additionally, SMARCA4 loss has been reported in 5% to 10% of patients with non-small cell lung cancer (NSCLC). 4 Furthermore, lung cancer patients with loss of SMARCA4 expression have a shorter survival time compared to those without the loss of this gene, indicating its importance in poor prognosis. 5 In this case, we describe the pathomorphological and immunohistochemical features of a female patient with DFSP who had a deletion in the SMARCA4 gene, an association not previously reported with this tumour, providing new insights into the molecular profile of this rare malignancy.
Case Description
A 40-year-old female patient presented to the outpatient department of the tumour hospital in Hebei Province with a groin mass that had been present for more than 2 months, accompanied by pain for 1 week. Physical examination revealed swelling in the groin area with purplish skin discoloration on the surface, but no ulceration was noted. Ultrasonography revealed a subcutaneous mass with a mixed echo occupying a space of approximately 6 × 6 × 3 cm in size, displaying a regular shape and clear boundaries. The patient did not exhibit any other symptoms or signs, leading to her admission to the hospital for surgical treatment.
After the surgery, a gross pathological examination revealed a nodular mass measuring 6 × 5.5 × 2 cm, characterized by a solid consistency, grey and white coloration, toughness, clear boundaries, and the absence of a distinct capsule. Further microscopic analysis revealed that the tumour consisted of cell bundles with spindle nuclei and intertwined collagen fibers. The tumour cells exhibited uniform staining, abundant cytoplasm, large nucleoli, easily identifiable mitotic figures, and were arranged in vortex- or wheel-like structures. Additionally, the tumour showed infiltration into the surrounding adipose tissue(Figure 1A-C).

Haematoxylin and eosin (H&E) and immunohistochemical staining results. (A-C): H&E staining showed vortex- or wheel-like structures. The tumour nuclei were uniformly stained, with abundant cytoplasm. The surrounding tumour infiltrated the surrounding adipose tissue (5×, 10×, 20×). (D-L): results of Bench Mark automatic immunohistochemistry method (20×); (D): VIM was diffuse strong positive; E: CD34 was diffuse strong positive; (F-G): CD68 and CD163 showed positive staining in the background histiocytes; (H): SMA was focal positive; (I): S100 was negative; (J): STAT6 was negative; (K): pan-TRK was negative; (L): BRG1 were not expressed.
Immunophenotyping demonstrated strong diffuse positivity for VIM and CD34, focal positivity for SMA, negativity for S100 and STAT6. CD68 and CD163 showed positive staining in the background histiocytes. These immunohistochemical profiles helped in excluding a diagnosis of dermatofibrosarcoma protuberans (DFSP). However, immunohistochemical staining for the novel markers pan-TRK and BRG1 revealed negative results. Pan-TRK, which is associated with targeted therapy, showed a negative result, indicating that the corresponding targeted drug cannot be used effectively (Figure 1D-L). Furthermore, a negative result for BRG1 suggests a loss of the SMARCA4 gene, a rare occurrence.
In order to confirm the presence of the SMARCA4 gene deletion, we conducted RT-PCR and Next-generation-sequencing (NGS) analysis of 1021 genes with a sequencing depth of 1000×. The results from these analyses confirmed the presence of the SMARCA4 gene deletion in this case of DFSP, as shown in Figure 2. This finding is unprecedented and has not been previously reported in the literature.
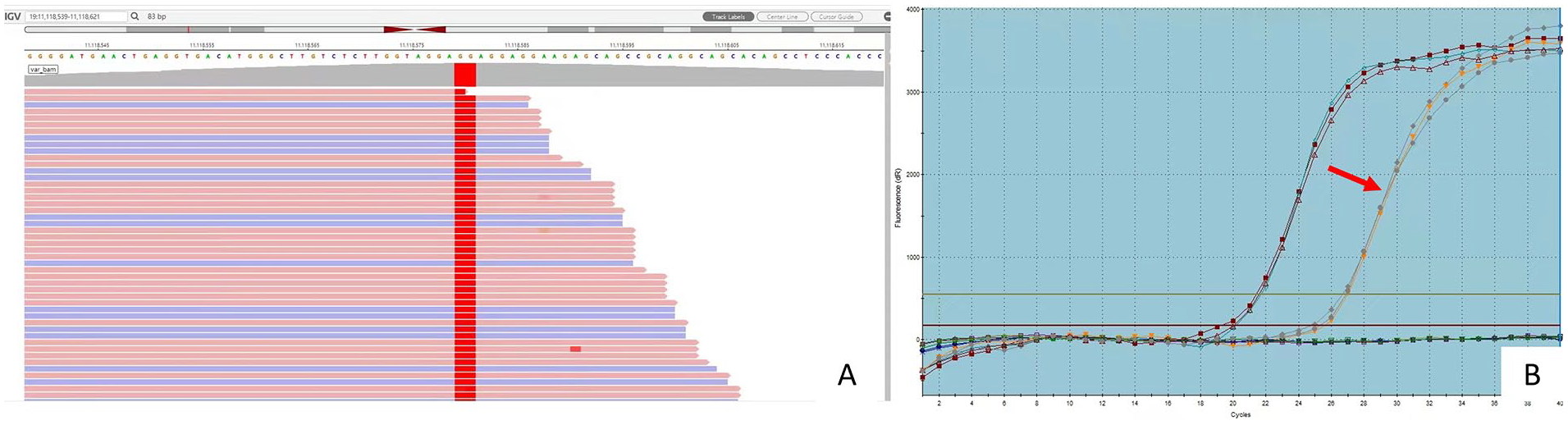
(A) SMARCA4 gene del-mutation (NM_003072.3 c.2004 2005delGGinsTT p.E668 E669delinsD*) was identified in the present case of dermatofibrosarcoma protuberans by 1021 genes NGS test; (B) SMARCA4 gene del-mutation was also validated using PCR.
Proteins interacting with SMARCA4 (BRG1) were identified through the STRING database analysis. The STRING database (https://cn.string-db.org/cgi/network?taskId=bSz4xRaZdvoT&sessionId=buqwGa3X2omw) is a comprehensive resource for known and predicted protein-protein interactions. Utilizing this database, a protein network interacting with SMARCA4 (BRG1) was constructed, as depicted in Figure 3.

STRING database analysis proteins interacting with SMARCA4(BRG1) were identified using the STRING database. 6 (A) a protein network interacting with SMARCA4(BRG1) was built by the database of protein-protein interactions; (B) The relationship between SMARCA4, SMARCA2, TP53, PDGFB and COL1A1 in the network of STRING database; (C) The specific explanations of (A) and (B).
Following the complete resection of the tumour, the tumour stage was determined to be T2N0M0. No additional treatments were deemed necessary. During the 2-year follow-up period, there were no signs of recurrence or metastasis.
Discussion
Dermatofibrosarcoma protuberans (DFSP) is a rare clinical entity that predominantly affects young to middle-aged men. Approximately 50% to 60% of DFSP cases manifest in the trunk, followed by the proximal extremities and the head and neck. 7 Clinically, DFSP is characterized as a slow-growing, localized, low-grade malignant fibrosarcoma that can manifest at any age. There are occasional reports of cases where DFSP transforms into fibrosarcoma (FS), and this transformation often leads to a significant potential for metastasis. 8
Initial clinical symptoms of DFSP are often subtle, and metastasis is uncommon. Metastatic occurrences, when they do arise, typically progress over an extended duration, with rare cases metastasizing to sites such as the lung, breast (pleuropulmonary), brain, or pancreas. 9 Incomplete or inadequate tumour resection can significantly increase the risk of postoperative recurrence. 10 MRI examination can effectively detect tumor recurrence, and after the administration of contrast agents, DFSP typically shows uniform enhancement. 11 Pathologically, DFSP is defined by the presence of fibroblasts arranged in a whorled pattern within an irregular tumour mass. In this specific case, the tumour exhibited typical morphological features, facilitating a clear and definitive diagnosis.
Multiple factors contribute to the development of DFSP, including oncogenes, tumour suppressor genes, and immune deficiency. Simon et al. 12 have demonstrated that chromosomal translocations involving chromosomes 17 and 22 (t 17; 22) (q22; q13) lead to the fusion of the PDGFB and COL1A1 genes. The resulting COL1A1-PDGFB chimeric gene produces mature PDGFB, activating the PDGFB receptor pathway and promoting tumourigenesis. In this case, no fusion of this gene and other genes were detected; however, we identified a mutation in the WRN gene (NM_000553.4, c.3868C>T, mutation frequency 13.8%) in addition to the SMARCA4 gene. However, the histological features and immunohistochemical expression of this case were very typical and consistent with DFSP. Mutations in the TP53 gene and overexpression of its protein have also been linked to DFSP development.13,14 Therefore, more detection methods need to be applied in the molecular testing of DFSP. Additionally, DFSP has been observed in patients with immunodeficiency disorders such as X-linked gammaglobulinemia, 15 adenosine deaminase-deficient severe combined immunodeficiency, 16 ataxia telangiectasia syndrome, 17 and human immunodeficiency virus (HIV) infection. 18
There are no reports on the relationship between DFSP and SMARCA4. Although a new classification of SMARCA4-deficient undifferentiated tumours has been added to the fifth edition of the WHO classification of thoracic tumours, DFSP with a SMARCA4 deletion has not been named a new subtype in the latest version of the soft tissue tumour classification. Previous studies 19 (60 cases) showed that loss of SMARCA4/BRGl and SMARCA2/BRM expression was associated with poor prognosis compared to intact expression. Another study 20 (193 cases) showed that low SMARCA2/BRM expression was associated with poor prognosis in patients with NSCLC (5-yr OS rate: 32.3 % vs 53.5 %). Several studies have revealed that BRM was a synthetic lethal target in SMARCA4/BRGl mutant tumours, and SMARCA4/ BRG1-del lung cancer cells required the complete depletion of BRM to effectively inhibit tumour cell growth in vivo and in vitro.21,22 Therefore, whether DFSP with SMARCA4 deletion predicts a worse prognosis is still unknown. This case is remains under follow-up, and survival also needs to be further studied.
In conclusion, the molecular characteristics of DFSP exhibit a wide range of variations, and a thorough comprehension of its pathogenesis and related factors can enhance the precision of patient prognosis evaluations. It is imperative to emphasize and pursue additional comprehensive investigations concerning DFSP tumours with a SMARCA4 deletion.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Beijing Xisike Clinical Oncology Research Foundation(Y-2022METAZQN-0045); Hebei Provincial Department of Finance/Hebei Provincial Health Commission 2023 Government funded Clinical Medicine Excellent Talent Training Project(ZF2024103).
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
LYP: Conceptualization, Methodology, Formal analysis, Writing – review & editing. DHY and LMY: Conceptualization, Methodology, Investigation, Formal analysis, Writing – review & editing. JY, JKQ and JHX: Conceptualization, Methodology. FXJ: Surgical excision.
Ethics approval and consent to participate
This study was approved by The Medical Ethics Committee of the Fourth Hospital of Hebei Medical University (code number 2021KY426). The participant was informed about the study goals. A consent form was completed by the participant before enrolment in the study. To make the participant feel more comfortable, an administrator interviewed her, and the collected information was kept confidential.