
Abstract
Background:
Current guidelines recommend discontinuing isotretinoin 6 months before rhinoplasty, due to concerns regarding impaired wound healing and adverse cosmetic outcomes.
Objectives:
The objective of the study is to systematically review primary literature involving patients taking isotretinoin within 6 months of rhinoplasty.
Methods:
A comprehensive literature search of PubMed, Embase, and Cochrane databases, from 1982 to August 2024, was conducted to identify articles for systematic review. Studies involving isotretinoin use within 6 months of rhinoplasty were included. Data were extracted by two independent reviewers and analysed qualitatively.
Results:
Two randomised controlled trials, four observational studies, and one case study were included. No significant adverse effects on wound healing or cosmetic outcomes were reported in 253 patients using isotretinoin. Four studies reported improved early cosmetic results, and patient satisfaction was consistently higher among isotretinoin users.
Conclusion:
The findings challenge current guidelines and suggest that isotretinoin can be safely used within 6 months of rhinoplasty, potentially improving early aesthetic outcomes and patient satisfaction.
Introduction
Isotretinoin (13-cis-retinoic acid), commonly known as Accutane→ (Hoffmann-La Roche, Nutley, NJ), was approved for severe treatment-resistant cystic acne by the FDA in 1982 1 and is an increasingly common treatment for moderate to severe acne today. 2 Isotretinoin is derived from vitamin A, and its mechanism of action involves the promotion of apoptosis, leading to involution of the sebaceous glands,3–6 inhibition of collagenase, 7 and activation of anti-inflammatory pathways. 1 This involution also thins and increases the elasticity of the skin. 8
Isotretinoin decreases the size of the pilosebaceous duct and alters its microbiome, reducing levels of acne-causing bacteria (such as Propionibacterium ).9,10 The effect of isotretinoin on wound healing is not completely understood, however it has been proposed that isotretinoin decreases fibroblast growth and metabolism, monocyte chemotaxis, and extracellular matrix modulation.9–11 Based on these mechanisms and the overall reduction of inflammation, it is possible that isotretinoin can influence or reduce internal scar formation.11,12 This is especially relevant in patients undergoing cosmetic facial surgery, including rhinoplasty. 10
Rhinoplasty is one of the most commonly performed cosmetic surgical procedures.13,14 Rhinoplasty patients tend to be younger with greater isotretinoin use for treatment-resistant acne.2,13 The surgery can be challenging in patients with particularly thick or sebaceous nasal skin.1,14–16 Thicker nasal skin with poor osseocartilaginous support makes it more difficult to achieve nasal definition through rhinoplasty, especially at the nasal tip.1,15,16 Postoperatively, patients with thick nasal skin often experience prolonged oedema and seek revision surgeries or additional treatments.1,14
Complications include infection, scarring, numbness, and postoperative deformities, which can lead to patient dissatisfaction.17,18 Intraoperative soft-tissue oedema can make it difficult to observe subtle contour changes and asymmetry.17,18 Additionally, post-rhinoplasty nasal tip asymmetry and other cosmetic deformities can result from contracture and fibrosis. 18 These complications can occur even years after rhinoplasty, in addition to postoperative acne.18,19 Case-control studies by Koc et al. and Sadeghi et al. showed increased incidence of acne in open rhinoplasty patients up to 3 months and 3 weeks postoperatively.20,21
Historically, there has been concern that use of isotretinoin during the pre- and postoperative periods might predispose rhinoplasty patients to impaired wound healing and postoperative cosmetic deformities. During the 1980s and 1990s, several case reports detailed complications following facial procedures in patients taking isotretinoin.22–24 These included impaired or delayed wound healing, keloid formation, and atypical scarring.22–24 In the case of rhinoplasty specifically, postoperative soft tissue deformities have also been reported. In a 2005 case series by Allen et al., three patients began isotretinoin post-rhinoplasty. 13 Subsequently, all three patients developed complications such as nasal tip asymmetry and skin atrophy. 13 Though these complications occurred 7 months to 2 years after surgery, 13 it was recommended that rhinoplasty be delayed until isotretinoin has been stopped for at least 6 months, and cutaneous procedures such as dermabrasion or laser treatment be delayed at least 1 year. 16
This is still the recommendation of the American Academy of Dermatology today and is also stated in the drug information given to all patients taking isotretinoin.25–28 Due to isotretinoin’s involvement in wound healing physiology and prior case reports, patients are typically counselled to avoid isotretinoin use for at least 6 months postoperatively.13,22 As such, the notion that isotretinoin use within 6–12 months of cutaneous surgery increases the likelihood of abnormal scarring, delayed wound healing, or cosmetic deformities is a commonly held belief among plastic surgeons.29,30
Despite these concerns, there has been interest in studying isotretinoin during the postoperative period to improve outcomes and patient satisfaction in rhinoplasty patients.1,30–32 The anti-inflammatory effect may reduce postoperative oedema and internal scarring to improve nasal tip definition after rhinoplasty.1,10 Similarly, others have begun evaluating the use of isotretinoin pre and perioperatively in order to decrease thickness and improve elasticity of the skin.14–16
The prior recommendations for isotretinoin use in rhinoplasty were established based on limited case series. With growing interest in isotretinoin use, it is important to review the available evidence. The objective of this systematic review is to examine the existing literature to determine if the use of isotretinoin is safe and effective in rhinoplasty patients within 6 months of surgery, including pre-, peri-, and postoperative exposure. Our hypothesis is that there will be no difference in safety outcomes with the use of isotretinoin within 6 months of surgery.
Methods
A systematic review was conducted following PRISMA guidelines with a pre-specified supplemental protocol to evaluate the effects of isotretinoin use in rhinoplasty patients. We conducted a comprehensive literature search from 1982, when isotretinoin received FDA approval, up to 22 August 2024, using Medline (PubMed), Embase, Google Scholar, Cochrane databases, and ClinicalTrials.gov. The review protocol, full list of search terminology, and an example search strategy for PubMed are available in supplemental files.
Studies were included if they were primary literature involving rhinoplasty patients receiving isotretinoin within a 6-month window of surgery. Review articles and studies administering isotretinoin outside this time window were excluded. A 6-month window was chosen based on current guidelines recommending a delay in surgery for patients taking isotretinoin.
Data were extracted using standardised, pilot-tested forms by two independent reviewers. Extracted data included study characteristics (title, year, country, design), population details (sample size, gender/age), intervention details (preoperative, perioperative, and postoperative isotretinoin use), outcome measures, adverse effects, and conclusions. Discrepancies in extracted data were resolved through discussion until consensus was reached.
Study quality was assessed using the Newcastle-Ottawa Scale (NOS) for observational studies and the Cochrane Risk of Bias Tool 2.0 for randomised controlled trials (RCTs).33,34 The level of evidence was rated using the Oxford Centre for Evidence-Based Medicine guidelines, ranging from Level I (adequately powered and conducted randomised clinical trials) to Level V (case reports). Given the variability in outcome measures and time points across studies, quantitative data analysis and formal assessment of bias across studies were not feasible. Therefore, a qualitative analysis was employed to synthesise the findings.
Results
A total of 43 studies were screened, and 14 were assessed. After applying inclusion and exclusion criteria, 7 were excluded for intervention (2), indication (1), study setting (1), and lack of reported outcomes (3). Ultimately, we included two RCTs, four observational studies, and one case study (PRISMA flow diagram available in supplement).
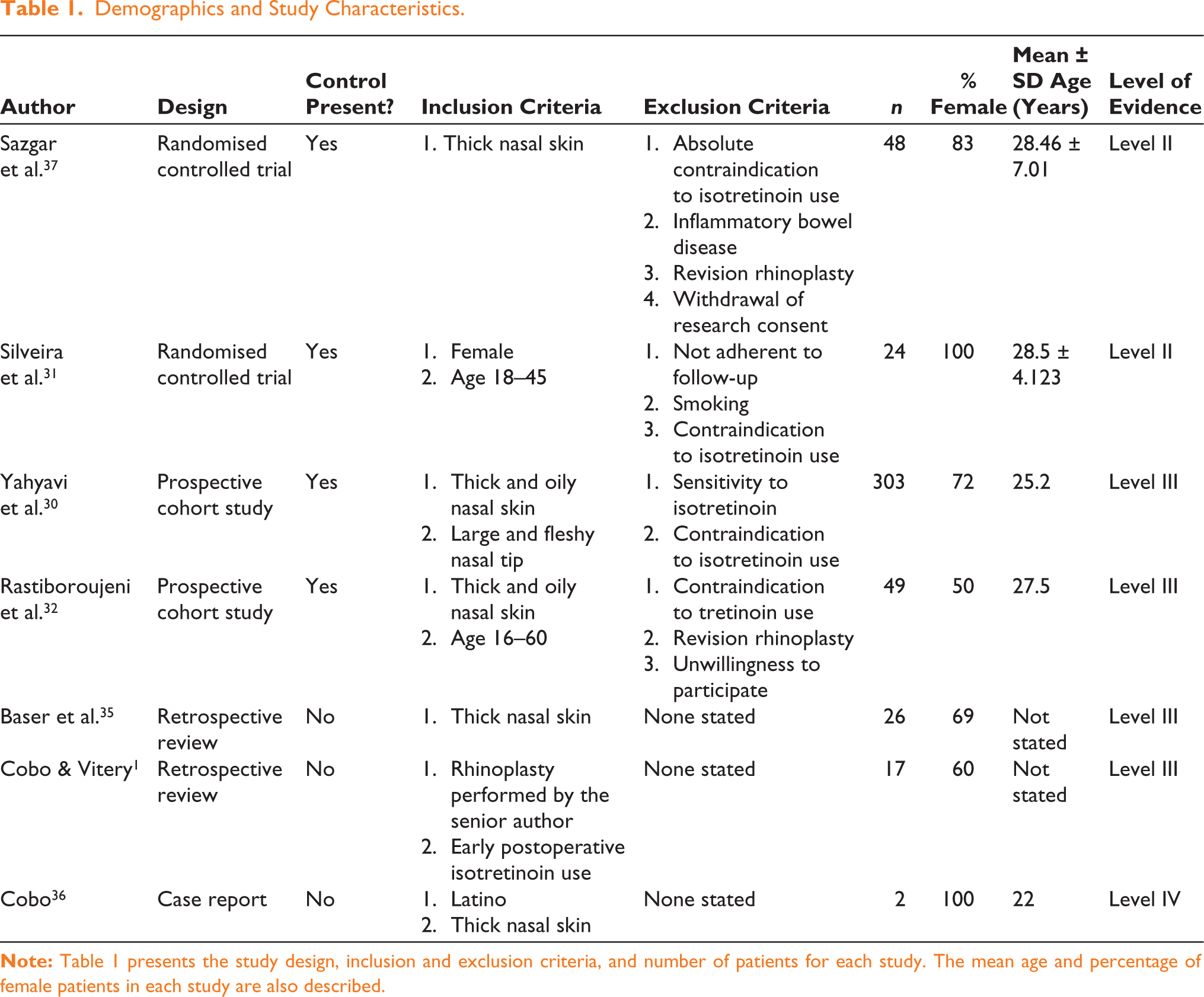
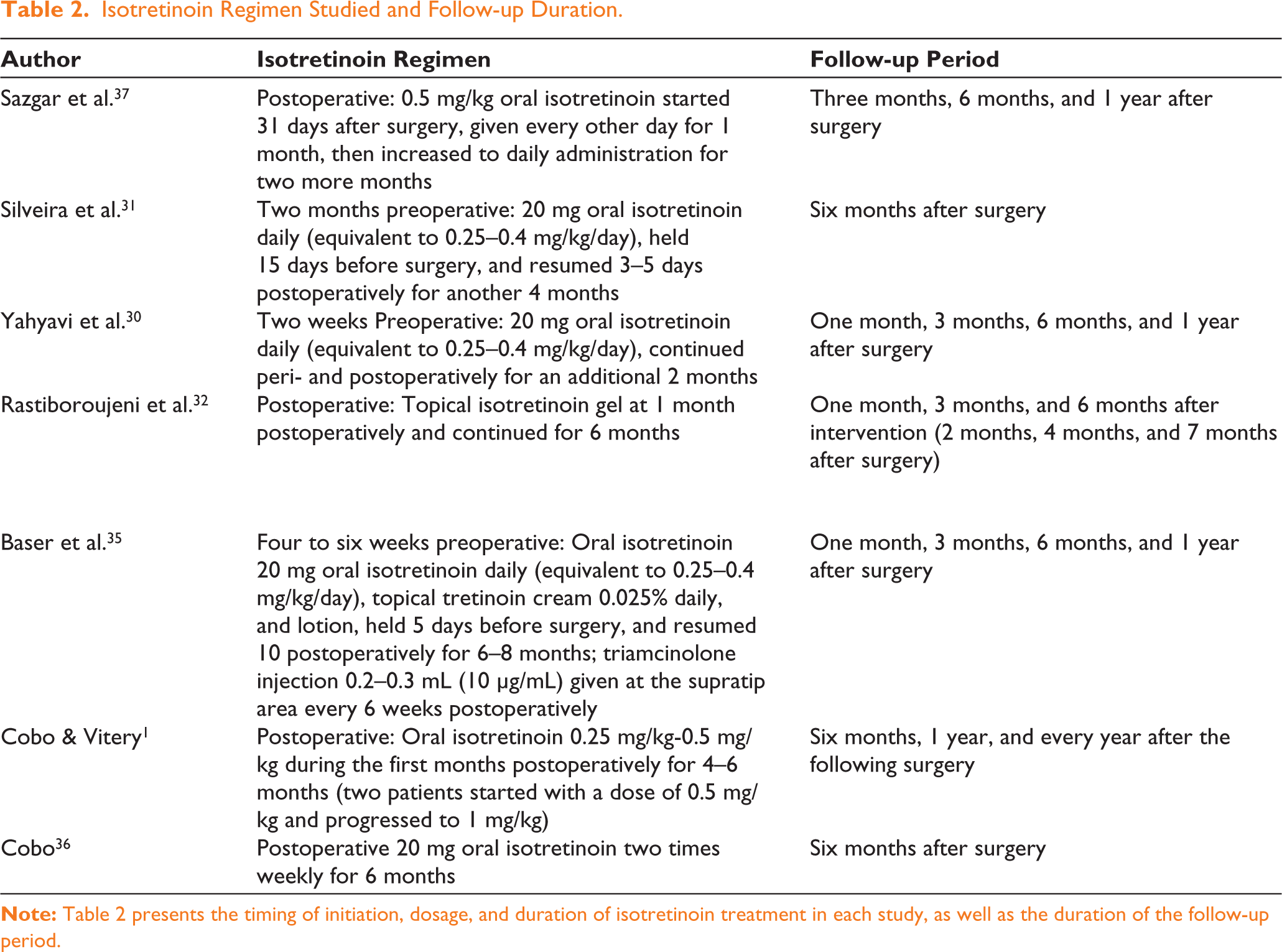
The included studies varied in sample size, study design, follow-up duration, and timing of isotretinoin administration (preoperative, perioperative, and postoperative use). Table 1 provides study design, sample size, inclusion/exclusion criteria, and demographics. Table 2 outlines the regimen of isotretinoin and follow-up periods. Table 3 describes the metrics, outcomes, and conclusions. While a formal meta-analysis was not performed due to heterogeneity in study design and outcomes, across the seven studies, 253 patients received isotretinoin with zero reported complications. Cheilitis, xerosis, headache, nasal and labial dryness, and elevated triglycerides were reported as known adverse effects which did not impede patient tolerance. All seven studies used postoperative isotretinoin. Two studies (Silveira and Baser) also included preoperative doses, and one study administered isotretinoin pre-, peri-, and postoperatively (Yahyavi).30,32,35
Demographics and Study Characteristics.
Isotretinoin Regimen Studied and Follow-up Duration.
Baser and Cobo retrospective studies and the Cobo case report each showed isotretinoin was associated with improved cosmetic outcomes without comparison to a control. These outcomes compared pre- and postoperative photographs by the operating surgeon, assessing nasal tip definition, texture, acne, and scarring.1,35,36 Sazgar et al. found isotretinoin was associated with improved cosmetic results in the short term, at 3 and 6 months by blinded surgeon evaluation of pre- and postoperative photographs on a scale of 1 to 5, but no change in cosmetic results at 1 year compared to control. 37 Silveira et al. demonstrated significant thinning of the nasal skin on ultrasound compared to control. 31 Yahyavi et al. and Rastiboroujeni et al. both concluded that there was no difference in rhinoplasty cosmetic outcomes when isotretinoin use was compared to control by surgeon or dermatologist evaluation (Table 3).30,32,36
Outcomes of Perioperative Isotretinoin Use in Rhinoplasty Patients.
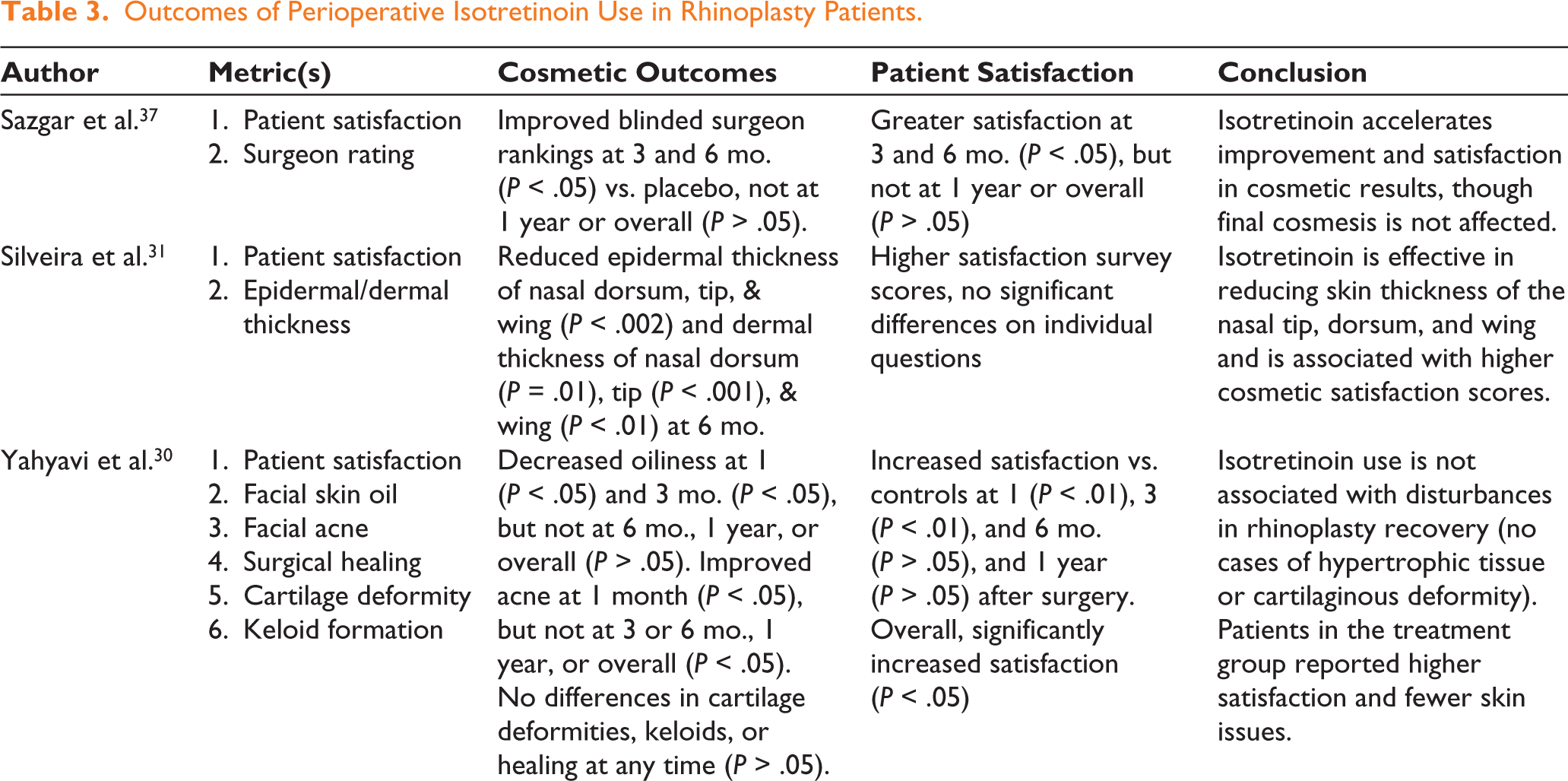
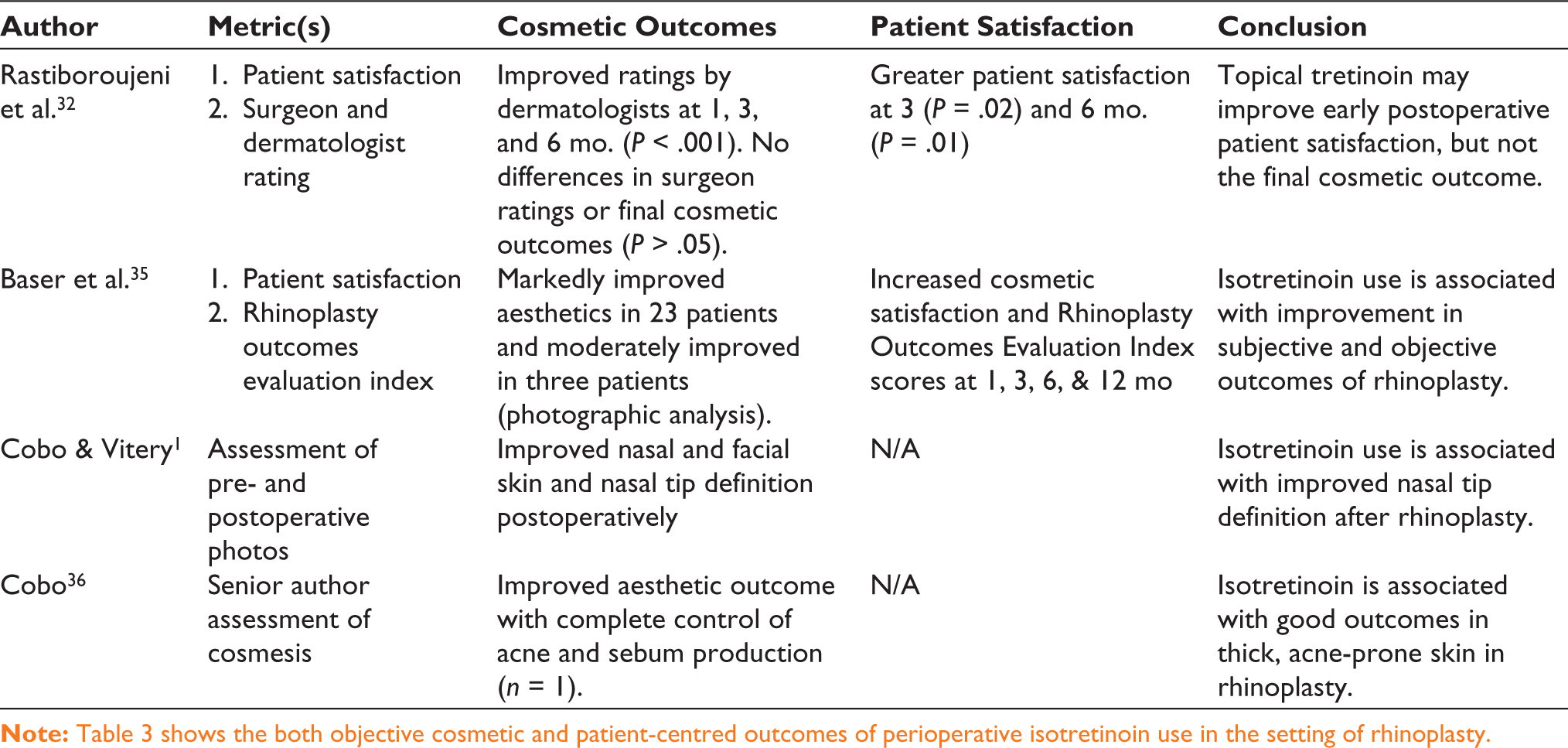
Regarding patient satisfaction, Sazgar et al. showed short-term improvement at 3 and 6 months compared to placebo, with no significant improvement at 1 year with postoperative isotretinoin use. 37 Silveira et al. demonstrated significantly improved patient satisfaction in both groups at 6 months, with higher scores for the treatment group using a Likert scale. 31 Rastiboroujeni et al. and Yahyavi et al. reported improved patient satisfaction compared to control at 6 months and 1 year, respectively.30,32 Baser et al. used subjective assessment to show marked satisfaction at 1 year, with 96.15% scoring above threshold at 1 year using the Rhinoplasty Outcomes Evaluation Index. 35
When evaluating the risk of bias, we used the Cochrane Risk of Bias 2.0 tool, the NOS for the observational studies, and assessed the case study cautiously, noting the inherent limitations and potential biases of case reports (Table 4).
Risk of Bias Analysis, All Studies.
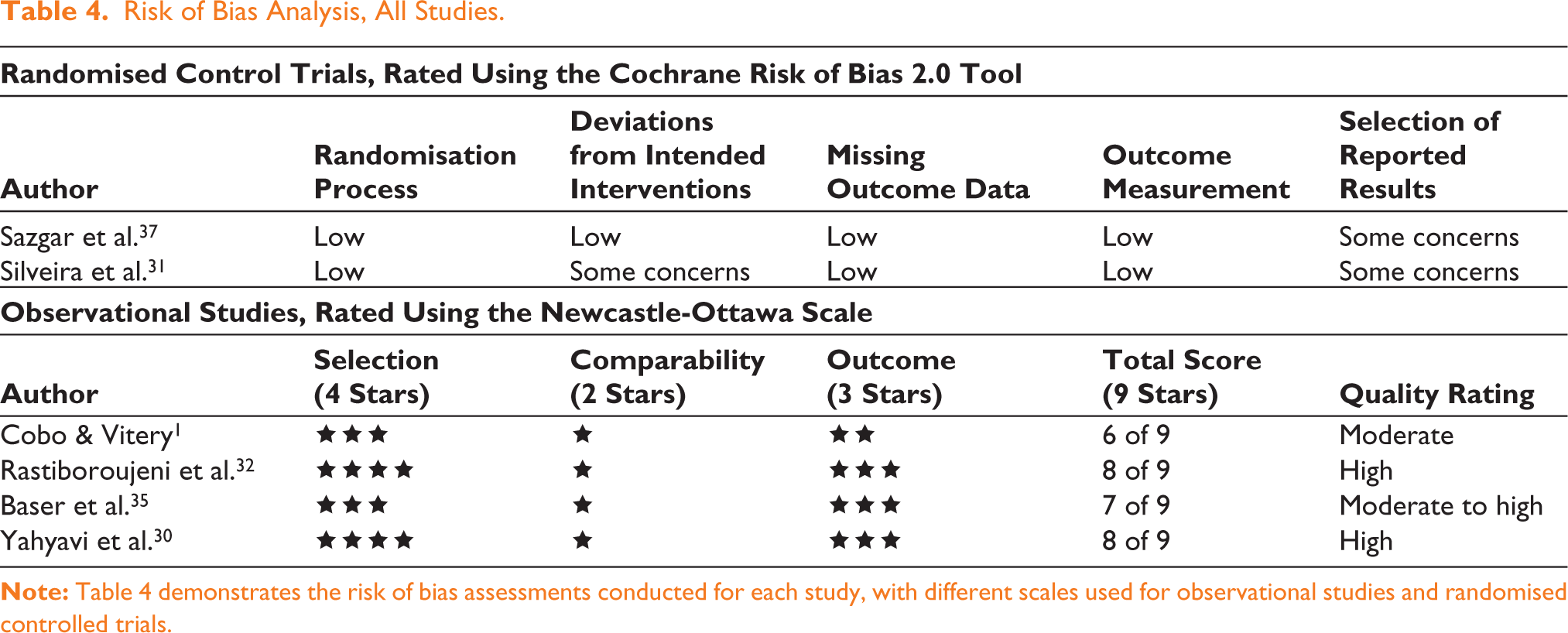
The Cochrane Risk of Bias 2.0 tool was used to assess the methodological quality of the included RCTs. Sazgar et al. demonstrated an overall low risk of bias with clear randomisation and appropriate blinding procedures. 37 However, some concerns arose regarding the selection of reported results due to the absence of a pre-specified analysis plan.
Silveira et al. also demonstrated clear randomisation; however, there were concerns about deviations from intended interventions, as providers were not blinded. 31 Additionally, the result reporting was unclear due to a lack of information on a pre-specified analysis plan, leading to a rating of ‘some concerns’ overall.
The retrospective cohort studies were assessed using the NOS. 33 Cobo and Vitery received 6 of 9 stars, indicating moderate quality. 1 Limitations included no non-exposed cohort and self-reported outcomes. 1 Rastiboroujeni et al. received 8 stars, indicating high quality. 32 Comparability was limited, with only one confounding factor (skin type) controlled. 30 Baser et al. received seven stars, indicating moderate to high quality. 35 Limitations included no non-exposed control and minimal confounder control. Yahyavi et al. received 8 stars, indicating high quality. 30 The study controlled for key confounders and had robust follow-up, but did not control beyond skin type.
Discussion
This systematic review evaluated isotretinoin use within 6 months of rhinoplasty, focusing on patient satisfaction, aesthetic outcomes, complications, and safety across two RCTs, four observational studies, and one case study. All studies administered isotretinoin postoperatively, with three incorporating preoperative doses. Only one study by Yahyavi et al. continued isotretinoin perioperatively. 30
No adverse events or surgical complications related to isotretinoin use were reported in over 253 patients receiving the medication within 6 months of surgery. Mild side effects such as cheilitis and xerosis were reported by Cobo et al., Yahyavi et al., and Silveira et al.; Yahyavi et al. reported headaches in two participants, and Silveira reported elevated triglycerides in one case.1,31,30 However, none led to discontinuation of treatment. It is also worth noting that pregnancy is a well-studied absolute contraindication to isotretinoin; all studies included this, and several counselled female patients to avoid pregnancy or required pregnancy testing.
Patient satisfaction, measured through Likert scales and other validated tools postoperatively, was consistently higher in patients receiving isotretinoin pre-, peri- and postoperatively up to 6 months.1,30–32,37 The patient population in the included studies shares similar characteristics to those undergoing rhinoplasty at baseline, predominantly female and aged in their mid-twenties; however, they had thick nasal skin. 38 This is a key consideration when evaluating generalizability. For patients with thick nasal skin, the strength of evidence for patient satisfaction is strong, with consistent findings across RCTs and observational studies. Reported patient satisfaction showed high levels at 6 months post-surgery, regardless of whether isotretinoin was administered orally, topically or with additional preoperative doses. While there is variation in study design and modes of delivery, isotretinoin had a consistently positive impact on patient satisfaction without adverse effects.
Cosmetic outcomes were measured by surgeon and dermatologist evaluation or by standardised scales and generally showed no long-term effect.1,32,35,37 Sazgar and Rastiboroujeni et al. both suggested a short-term aesthetic benefit for 6 months. Sazgar and Rastiboroujieni et al. demonstrated associated improvements in skin texture and nasal contour at early stages that equalised at 6 months to 1 year.32,37 Similarly, Baser (2024) and Cobo (2017) showed comparable early results; however, the absence of a control group raises concerns about potential bias and generalizability.1,35 Final aesthetic outcomes do not appear significantly influenced by isotretinoin, though there may be a short-term benefit within 6 months of surgery.
Several study-level limitations impact the strength and reliability of these findings. The included RCTs exhibited risk of bias due to a lack of blinding and selective reporting. Observational studies were generally of moderate quality, with limitations related to selection bias, confounder control, and reliance on self-reported outcomes. The small sample sizes in some studies and the paucity of primary literature also limit generalizability. Conclusions are limited by variability in study design, with variable dosages, timing of doses, and method of administration across studies.
While the included studies employed different dosages and variable timelines of isotretinoin administration, most commented on the utility of using lower-dose regimens to avoid deleterious side effects while achieving the desired outcomes. The standard oral dose to address acne is 0.5–1 mg/kg per day39–41 to reach a cumulative dosage of 120–150 mg/kg over 3–6 months; most studies stayed below this range.41,42 Variability of dosing regimens seen in Table 2 limited our ability to formally make recommendations; however, there was no obvious correlation between higher doses and the incidence of negative side effects. Prior studies have shown that many side effects of isotretinoin are highly dose-dependent and, as such, can be reduced with lower daily doses.39,40,43 Given that each study found that isotretinoin provided either benefit or an equivalent postoperative outcome for rhinoplasty patients with thick nasal skin, it is reasonable to infer that lower-dose regimens and use in preoperative, perioperative, and postoperative time frames are potential options in this population.
Current evidence suggests that isotretinoin may be safely incorporated into surgical planning for rhinoplasty patients with thick nasal skin without significantly increasing the risk of adverse outcomes. Clinicians can consider isotretinoin part of a comprehensive management strategy for patients with thick or oily skin, potentially improving both aesthetic outcomes and patient satisfaction. Current literature is insufficient to support a specific methodology at this time. However, the medication may be used safely with proper patient selection.
For patients considering rhinoplasty while on isotretinoin or with a history of its use, the findings of this study are reassuring. Current literature indicates that isotretinoin does not significantly interfere with wound healing or aesthetic results when dosed intentionally for patients with thick nasal skin. Patients should be aware of the common side effects, such as dry skin and cheilitis, but these are unlikely to affect surgical outcomes.
Current guidelines often recommend discontinuing isotretinoin well before elective surgery due to concerns about impaired wound healing. This caution stems from earlier case reports of nasal tip deformity following rhinoplasty in patients who had started isotretinoin postoperatively. 13 The study suggested that isotretinoin might interfere with collagen production, fibroblast activity, and other critical components of the wound healing process, leading to poor surgical outcomes. 13 As a result, it has become common practice for surgeons to advise patients to discontinue isotretinoin use for up to 6 months before cosmetic procedures like rhinoplasty to minimise the risk of complications.
However, the findings from this systematic review challenge the necessity of these stringent guidelines, particularly for procedures where skin thickness and oiliness are critical factors in recovery. The studies reviewed did not provide strong evidence that isotretinoin is detrimental to postsurgical wound repair or contributes to poor outcomes. On the contrary, isotretinoin, whether preoperatively, perioperatively, or postoperatively, was associated with positive outcomes and few side effects. Therefore, the recommendation to delay facial surgery until isotretinoin has been discontinued for 6 months should be reconsidered. Updated guidelines that allow for more flexible isotretinoin use, especially in the perioperative setting, may be warranted.
In addition to heterogeneity, this review was limited by the inability to retrieve some potentially relevant studies, including those published in languages other than English. While efforts were made to include all eligible studies, the possibility remains that some data were not captured, potentially impacting comprehensiveness. There is also potential for publication bias, as studies showing positive results (improved cosmetic outcomes with isotretinoin) are more likely to be published. Additionally, selective outcome reporting within studies could have led to an overemphasis on favourable findings while downplaying or omitting adverse results. Given the limited number of studies on this topic, the overall conclusions should be interpreted with caution until more high-quality research is conducted. These limitations highlight the need for large, well-designed studies to provide more definitive guidance on timing and dosage regimens for use in rhinoplasty.
In conclusion, this systematic review suggests that isotretinoin can be safely incorporated into the surgical planning of rhinoplasty patients with thick nasal skin. The consistent findings across multiple studies underscore positive effects on improving patient satisfaction and early aesthetic outcomes. These results support the need for updated clinical guidelines that reflect current evidence, ensuring that patients receive the most effective care possible. Future larger studies are still needed to better define dosing and timing. At this time, clinicians should consider a patient’s individual risk factors when deciding on use until more definitive protocols are established.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.