
Abstract
Introduction:
Dorsal hump reduction is one of the most common reasons that rhinoplasty is pursued by patients. While there are multiple treatment modalities, dorsal preservation rhinoplasty (DPR) technique has enjoyed a renaissance in the last decade. This is a retrospective review of DPR’s subjective effect on nasal function and objective effect on the internal nasal valve (INV).
Material and Methods:
Eight septorhinoplasty patients presenting with functional and aesthetic nasal concerns underwent DPR. Preoperative and postoperative facial computed tomography scans of each patient were evaluated by both authors. A NOSE questionnaire was also administered to each patient preoperatively as well as postoperatively.
Results:
A statistically significant improvement in nasal function was noted, with NOSE scores going from 93.8 (standard deviation 4.2) preoperatively to 23.1 (standard deviation 12.4) postoperatively. Mean INV measurements went from 11.3° (standard deviation 1.2°) preoperatively to 11.5° (standard deviation 1.9°) postoperatively.
Discussion:
This is the first report evaluating changes in both INV angle and patient-reported outcomes with the DPR technique.
Conclusion:
Based on the observations of this limited case series, DPR offers improvement in both objective and subjective metrics of nasal function.
Introduction
Cosmetic rhinoplasty is a challenging procedure with one of the highest rates of revision amongst cosmetic surgery procedures. While patients most frequently pursue primary rhinoplasty to address dorsal hump reduction, revision rhinoplasty patients most often cite concerns with postoperative mid-vault irregularity and nasal obstructive symptoms.1,2 Dorsal preservation rhinoplasty (DPR) is a decades old technique, enjoying a recent resurgence, that aims to improve outcomes and decrease revision rates by maintaining mid-vault anatomy. 3 The goal of this manuscript was to assess whether or not DPR not only improved aesthetic outcomes, but also concurrently addressed nasal function.
Materials and methods
This is a retrospective chart review of patients treated from January 2024 to December 2024, and no experimental procedures were performed on human subjects. Therefore, this report was not subject to institutional board review. All procedures were conducted in accordance with the Declaration of Helsinki. Preoperative and postoperative CT imaging and NOSE questionnaires were performed for patients who underwent DPR at the authors’ clinic. Patients were excluded if they did not return for postoperative imaging, they failed to complete their postoperative NOSE questionnaire, or if they had concurrent tip plasty with their DPR.
The internal nasal valve is a cross-sectional area bound by the nasal septum medially, caudal edge of the upper lateral cartilage superolaterally, and the head of the inferior turbinate inferiorly. This area represents the narrowest portion of the nasal passage for airflow. In order to assess it radiographically, high resolution computed tomography images were oriented on a tilted axis with the coronal plane perpendicular to the estimated acoustic axis. 4 Using this modified nasal base view to account for the functional anatomy of the nose has been previously determined to give a more accurate assessment of the nasal valve and associated physiologic nasal airflow. 5 The internal nasal valve was then measured one slice anterior to the inferior turbinate, with each author independently verifying markings and measurements.
Eight patients were given preoperative and postoperative Nasal Obstruction Symptom Evaluation (NOSE) scale questionnaires to assess subjective nasal function. The NOSE scale is a validated patient-reported outcome measurement instrument that helps quantify the functional benefit of septorhinoplasty on nasal breathing. Scores can range from 0 to 100, with 100 being the worst, and 0 being asymptomatic. Descriptive statistics were used to measure differences in preoperative and postoperative measured values.
All surgeries were performed under general anesthesia using a low strip septoplasty, lateral and transverse osteotomies and a pushdown technique. No tip plasty was performed in any of the included patients. The septum was accessed utilizing a left hemi-transfixion incision followed by sub-mucoperichondrial and sub-periosteal septal flaps on either side of the septum. The cartilaginous septum was released from the vomer, maxillary crest and anterior nasal spine to complete a swinging door septoplasty (Figure 1) followed by low strip septal excision and subdorsal resection of the bony-cartilaginous septum cephalic to the dorsal hump (Figure 2). The swinging door septoplasty allowed access to the bony septum, where 6 of the 8 patients had unilateral septovomerine spurs removed. Radix, transverse, and lateral osteotomies were percutaneously completed with a 2-mm osteotome. Once the mid-vault was completely mobilized, it was pushed down into the piriform aperture until the dorsum was at the desired height (Figure 3). Any excess basal septum was sequentially trimmed in 1-mm segments until the dorsal profile was deemed aesthetically acceptable. While flaring of the caudal upper lateral cartilages was noted in each of the cases, the cartilages were not dissected off the lateral bony pyramid in order to maintain mid-vault width, as this was an intended effect of the procedure.
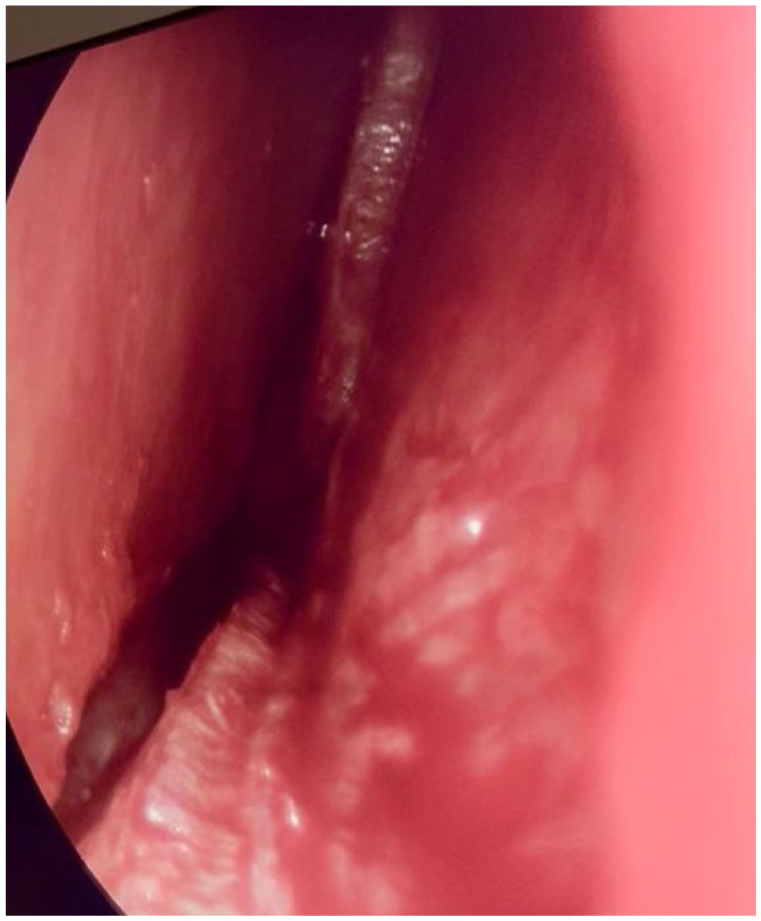
Endoscopic view of swinging door septoplasty.
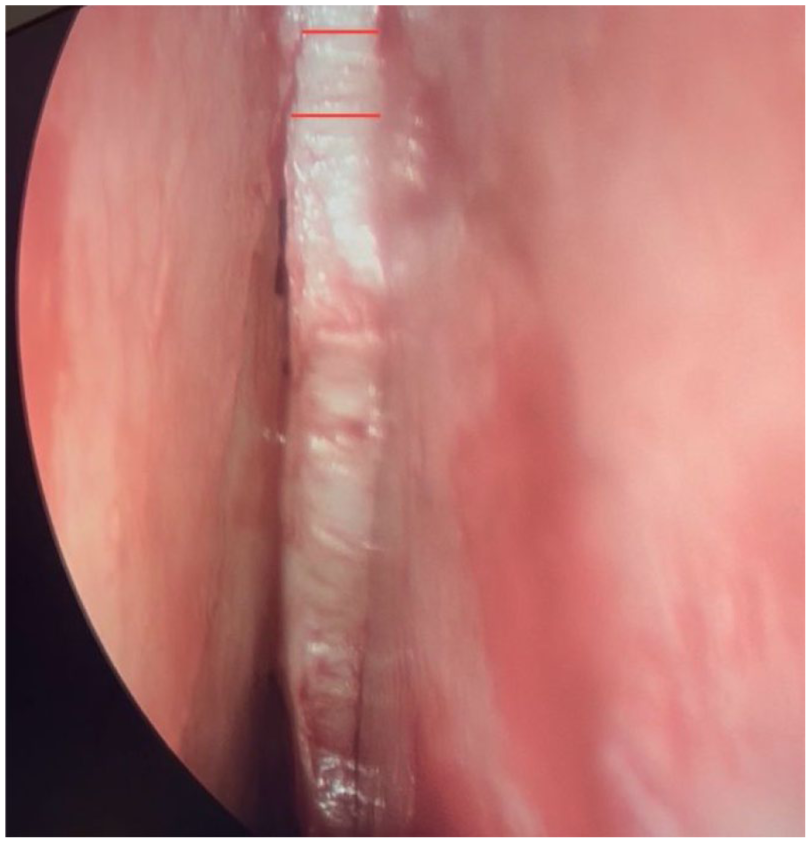
Endoscopic view of access to the septum beneath the dorsal hump. The red lines represent an example of the area of bony-cartilaginous resection to prevent the mid-vault from being “blocked out” when being pushed down into the piriform. The authors are conservative with this step to avoid infantilizing the dorsum.
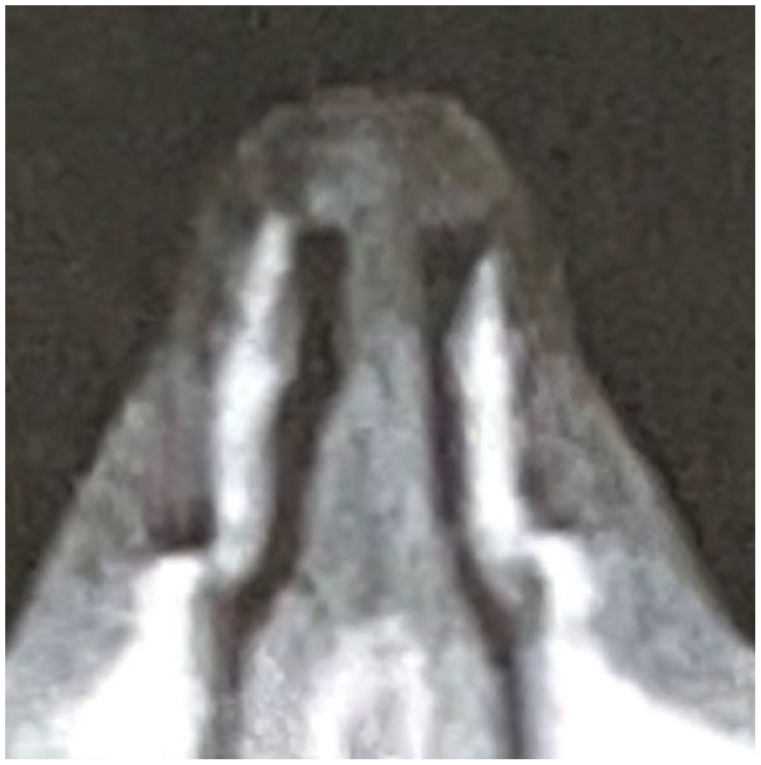
Reference to show displacement of mid-vault into piriform after push down maneuver.
Results
Eight patients (mean age 31) with both functional and aesthetic nasal complaints underwent DPR. There were 7 female patients and 1 male patient. Recorded data points were age, sex, preoperative and postoperative NOSE score, radiographic preoperative and postoperative INV angle measurement, and subjective aesthetic assessment at two months (Figure 4). There was no significant difference in INV measurements (.807, P > .05). The mean preoperative internal nasal valve angle was 11.3° (standard deviation 1.2°), while the average postoperative angle was 11.5° (standard deviation 1.9°). The mean preoperative NOSE score was 93.8 (standard deviation 4.2), and the mean postoperative NOSE score was 23.1 (standard deviation 12.4), indicating a statistically significant improvement in nasal obstruction symptoms (9.42 × -10 P < .05). In all cases, patient’s endorsed satisfaction with their dorsal hump reduction at their 2-month follow-up visit (Figure 5). An example of preoperative and postoperative INV measurements is demonstrated in Figure 6.
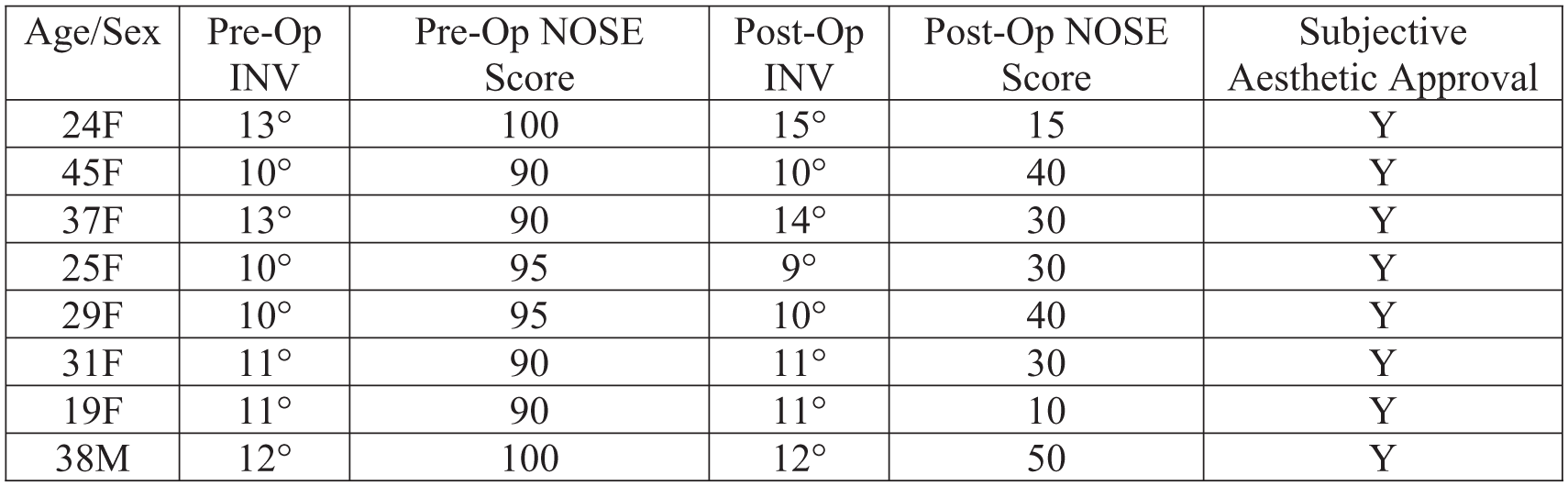
Objective radiographic and patient-reported subjective preoperative and postoperative measurements for 8 DPR patients.

Preoperative and 2-month postoperative clinical progress pictures of a 37-year-old female treated with isolated DPR.
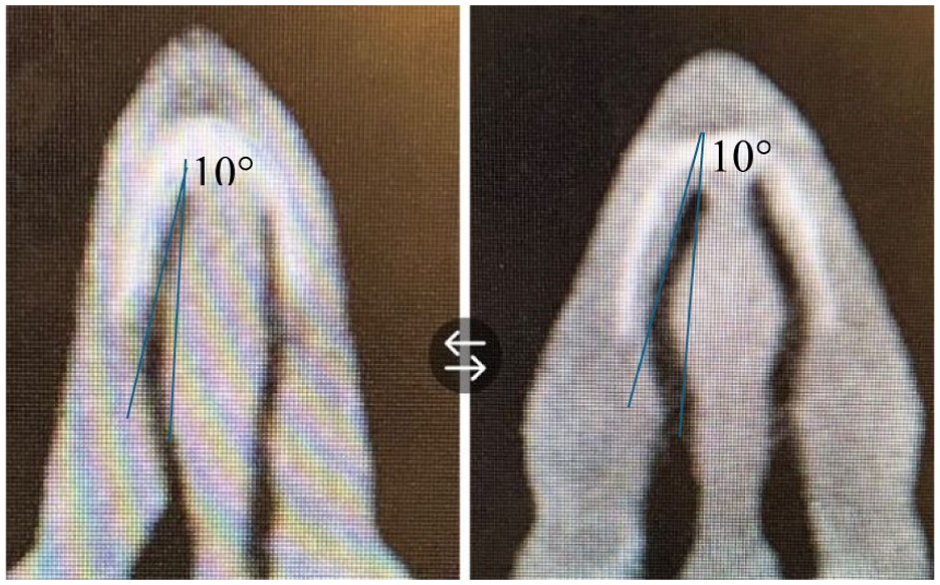
Before and after pictures of radiographs showing measurement of INV.
Discussion
There have been 3 other reports in the literature on the effect of DPR on the internal nasal valve.6-8 Notably lacking from these reports was the clinical significance of changes in the internal nasal valve with DPR. Previous studies have shown that while symptomatic rhinoplasty patients had a composite average internal nasal valve angle of 10° while asymptomatic rhinoplasty patients had an average INV angle of 11.4°.8,9 Previous reports have used this as conjecture to speculate about the impact of changes in INV angle, but none have used a patient-reported outcome measure to correlate changes with DPR. This is the first such report that integrates the subjective and objective outcomes on patients and also the first to look exclusively at the pushdown technique.
Colloquially referred to as a dorsal hump, a convex dorsum or “tension nose” has been shown to be due to excessive anterior septal growth. 10 Traditionally, this has been treated with en bloc dorsal resection and subsequent spreader graft reconstruction to widen the internal nasal valve. This does not treat the underlying cause of the dorsal hump, however. Recently, the re-discovery of the DPR technique has allowed rhinoplasty surgeons to reduce the dorsal hump by addressing the anteriorly overgrown septum directly, obviating the need to reconstruct native mid-vault anatomy as was needed with direct hump resection.
A majority of patients in the authors’ clinic have concurrent tip plasty with DPR, which limited the amount of patients who could be included in this series. Additionally, asymptomatic patients often did not comply with postoperative imaging and questionnaires, eliminating them from being observed as well. With only 8 patients observed, there is a possibility that this report suffers from sample bias. Another potential confounder of these reported results are the concurrent functional procedures performed with DPR. Notably, 6 of the 8 patients in this report had septovomerine spurs excised that likely provided additional improvement in nasal obstructive symptoms. The two patients who did not have bony spurs removed were the 29-year-old and 31-year-old females included in this case series, and each reported similar improvement in their NOSE score with isolated DPR. Nonetheless, formal investigations should aim to incorporate larger sample sizes and isolate DPR as a variable to evaluate its effect on the nasal valve function more thoroughly. Additionally, the type of DPR technique employed must be taken into account. While the authors used a low strip with pushdown osteotomies and the closest correlate study used a low strip with let-down ostectomies, 8 it would be beneficial to evaluate the commonly used DPR combination of high strip septoplasty with pushdown osteotomies.
Preservation rhinoplasty represents a paradigm shift in rhinoplasty surgery with natural results that maintain the native mid-vault anatomy and provide long-lasting outcomes. Based on the observations of this limited case series, DPR additionally offers improvement in both objective and subjective metrics of nasal function.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.