
Abstract
High-grade gynecomastia (Simon grades IIIB) presents significant challenges due to skin redundancy, nipple-areolar complex (NAC) displacement and ptosis. Traditional techniques such as mastectomy with free nipple grafting or breast reduction-style approaches often result in visible scarring and suboptimal aesthetic outcomes. This study evaluates a combined approach of circumareolar skin excision, liposuction, glandular resection and fat grafting to optimise chest contouring in a single stage. Twenty patients (aged 13–52 years) with high-grade gynecomastia underwent combined doughnut skin excision, liposuction and glandular pull-through excision. NAC repositioning, high-definition liposculpturing and fat grafting enhanced pectoral definition. Patient-reported outcomes and independent observer assessments evaluated chest appearance, NAC aesthetics, symmetry and pectoral definition. Postoperative assessments significantly improved all parameters (mean scores: chest appearance 4.0, NAC appearance 4.2, symmetry 4.3, pectoral definition 4.6). No major complications or revisions were required. This technique offers a reproducible, single-stage solution for high-grade gynecomastia, minimising scarring while optimising aesthetic outcomes through NAC repositioning, fat grafting and high-definition liposculpturing.
Keywords
Introduction
Gynecomastia, the benign proliferation of glandular breast tissue in males, affects up to 65% of adolescent boys and 30%–50% of adult men.1,2 While low-grade cases (Simon I–IIA) can often be managed with liposuction and minor gland excision, high-grade gynecomastia (Simon IIB–III) presents a surgical challenge due to significant skin redundancy, nipple-areolar complex (NAC) ptosis and poor tissue elasticity. 3
Historically, simple mastectomy with free nipple grafting was the standard for severe gynecomastia, but it often resulted in insensate, grafted NACs and prominent scarring. 4 Alternative approaches, such as pedicle-based nipple transposition (e.g., double-dermal pedicle techniques), improved NAC viability but still left visible vertical or T-shaped scars. 5 Liposuction alone fails to address skin laxity, necessitating secondary procedures. 6
Recent advancements advocate circumareolar skin excision with purse-string closure, which minimises scarring while allowing effective skin redraping. 7 Combining this with high-definition liposculpturing and fat grafting enhances pectoral contouring, mimicking a natural muscular appearance. 8
This study presents a refined single-stage approach integrating:
Circumareolar doughnut excision for skin tightening Liposuction-assisted glandular debulking Fat grafting for pectoral definition NAC repositioning at an anatomically ideal location: near the inferolateral region of the pectoralis major muscle
We evaluate its efficacy in 25 high-grade gynecomastia patients, comparing outcomes to traditional techniques.
Patients and Methods
Preoperative Assessment
The preoperative evaluation begins with a thorough medical history to rule out secondary causes of gynecomastia, such as liver disease, hormonal imbalances (e.g., hypogonadism, hyperprolactinemia) or medication-induced cases (e.g., anabolic steroids, antiandrogens). Patients should also be assessed for Klinefelter syndrome or testicular tumours if clinically indicated. Documentation of symptom duration, progression and any associated pain or tenderness is essential.
A detailed physical examination follows, classifying the gynecomastia using Simon’s grading system (III). The skin is evaluated for elasticity, striae and degree of ptosis, while the NAC is assessed for size, position, symmetry and ptosis. Palpation helps differentiate between glandular and fatty predominance. If malignancy is suspected, ultrasound or mammography may be performed. Hormonal workup (testosterone, oestradiol, LH, FSH, prolactin, HCG) and liver/kidney function tests are ordered when systemic causes are likely.
On the day of surgery, preoperative marking is conducted with the patient standing and arms abducted. Key landmarks include the sternal notch, midline, inframammary fold (IMF) and pectoralis major borders to guide liposuction zones. The ideal neo-NAC position is marked at 19–21 cm from the sternal notch, approximately 1 cm above and medial to the inferolateral pectoral border for a natural male contour. An ellipse/round is marked around the NAC to the neo-NAC position, representing the area to be de-epithelised for NAC repositioning. Concentric circles are drawn representing the areas of bulk fat removal, while negative spaces (infraclavicular and deltopectoral grooves) are marked for high-definition liposculpturing and areas for fat injection marked (Figure 1).
Pre-operative markings: Highlighting the Areas for High-definition Liposuction—Marking the Negative Spaces for Etched Appearance; Doughnut Skin to Be Excised to Reposition the NAC and Correct the NAC Size.

Intraoperative Procedure
The procedure is usually performed under general anaesthesia, supplemented with an intercostal nerve block for postoperative analgesia. The patient is positioned supine with arms abducted at 90. Tumescent solution is infiltrated into the subcutaneous and sub-glandular planes using an infiltration cannula through a 6 mm incision at 6–7’o clock positions (Figure 2).
Incision for Tumescent Infiltration and Liposuction: Nearly 6 mm incision at 6–7’o Clock Positions.
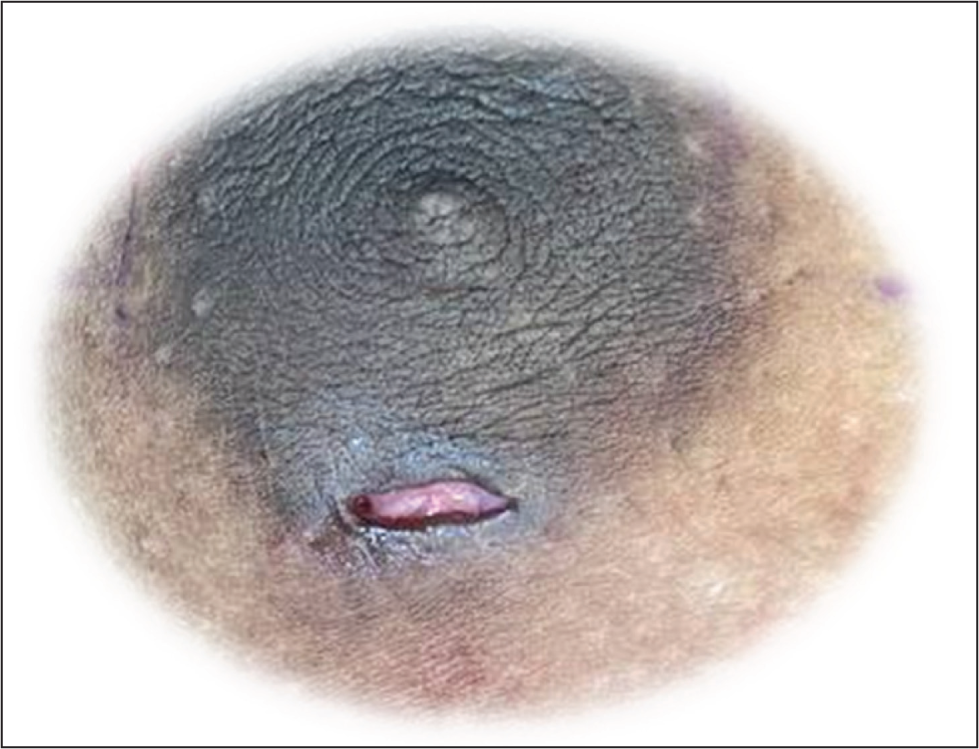
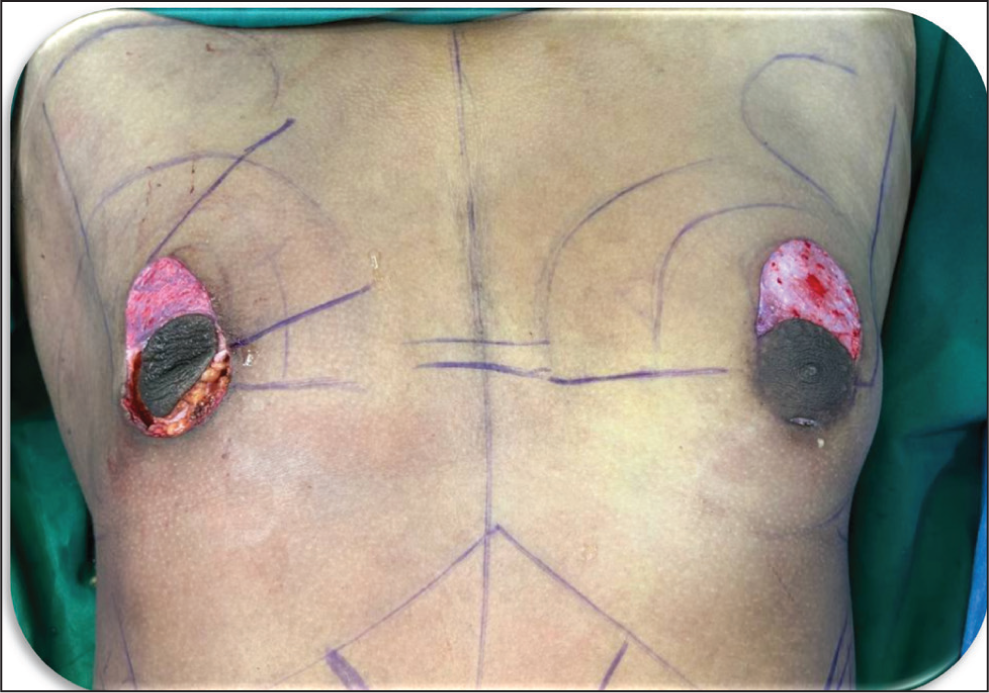
Doughnut skin for de-epithelialisation is marked with a 4–6 cm outer diameter and around 2.5 cm diameter of neo-NAC to the neo-NAC position. The marked area is de-epithelised, preserving the dermis for vascularity (Figure 3).
De-epithelization: Doughnut Excision of the Epidermis—From the NAC to Neo-NAC.
Liposuction is initiated with pre-tunnelling followed by power-assisted liposuction in a dual plane using a 4 mm Mercedes cannula for the deeper plane—using the cross-hatching technique, followed by radial feathering at transition zones with a 3 mm cannula. A 5 mm bent basket cannula is used for superficial sculpting to enhance pectoral definition, particularly along the pectoralis major borders. Cross-chest liposuction ensures even contouring while avoiding any further visible scars 9 (Figure 4).
Cross-chest Liposuction: Avoiding Incisions for Liposuction in the Central Region Below the NAC.

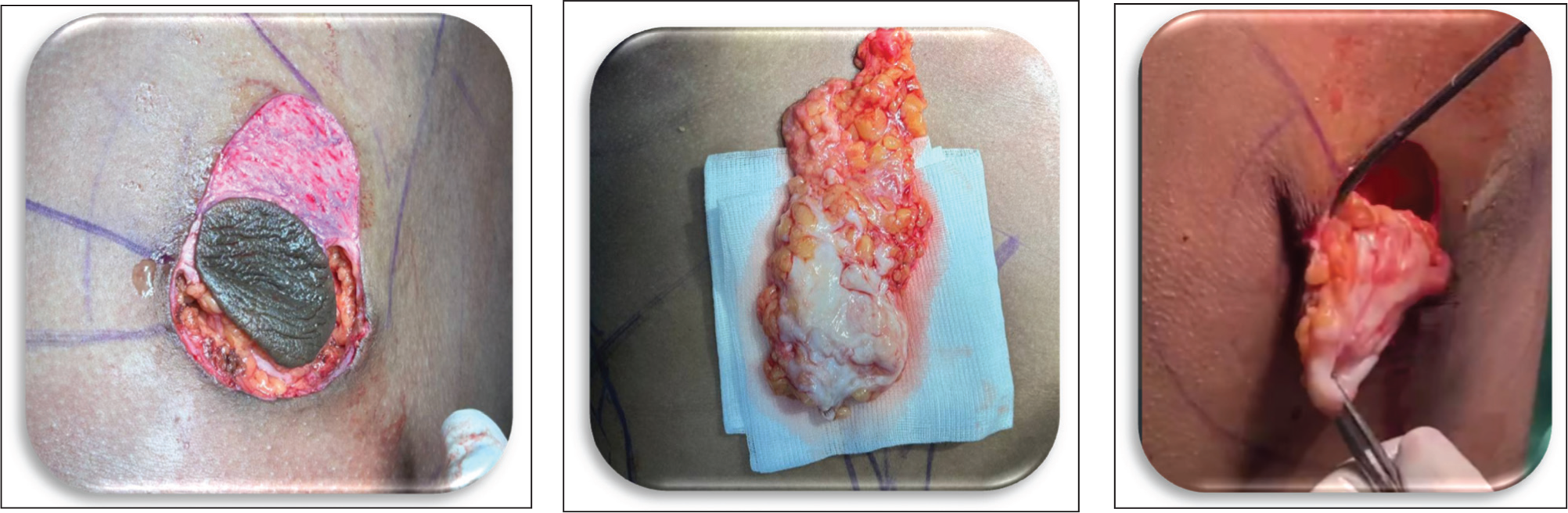
Glandular excision is done using a 2cm incision at the lower areolar margin allowing sharp dissection and traction-assisted en bloc gland removal (Morselli’s technique), and 4–5 mm of subareolar tissue is preserved to prevent saucer deformity (Figure 5).
Glandular Excision: Through Peri-areolar Incision and Avoiding the Saucerization Deformity, Leaving 4–5 mm Tissue Just Below the NAC.
Fat grafting is performed by injecting it into the subpectoral plane (lateral/inferior border for pectoralis major muscle definition) or upper pole for volume augmentation.
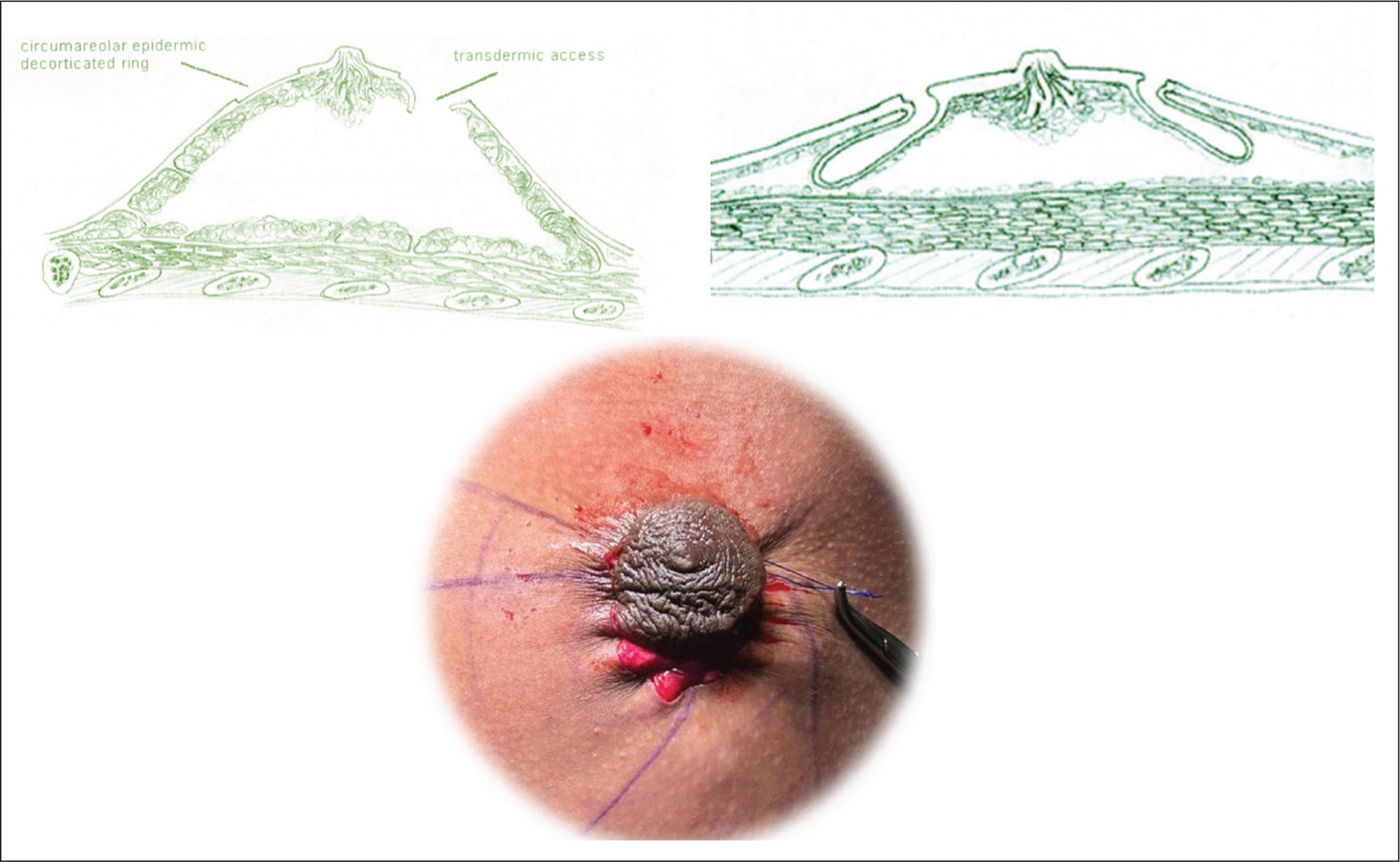
A purse-string closure with 3-0 Prolene in the dermal layer minimises scarring, with the final NAC diameter adjusted to 2.5–3 cm, the wound around NAC closed in layers (Figure 6).
Purse String Sutures with Prolene: For Reducing the Size of NAC and Prevent Further Stretching Postoperatively.
In case there is too much ooze, a drain is inserted for 24–48 hours.
Postoperative Management
Taping is done for a week postoperatively to stabilise the NAC position with a 1 inch Transpore tape (Figure 7).
Taping Postoperatively.

During the first 2 days, the patient wears a compression vest with foam padding to minimise seroma risk and maintain the contour following fat injection.
Immediate postoperative care includes a non-adherent gauze and foam dressing under a compression garment, worn continuously except during showering for 1 month.
The NAC is monitored for venous congestion, and gentle lymphatic massage begins on postoperative Day 3, continued for 10–12 days.
Light exercise resumes at 3 weeks, while heavy lifting and chest workouts are permitted after 6 weeks. Follow-up visits are scheduled at 1 week, 1 month, 3 months and 6 months.
Complication Management
Hematoma: Addressed with intraoperative haemostasis and drains if needed.
NAC necrosis: Prevented by preserving the subdermal plexus and avoiding excessive tension.
Scar widening: Mitigated via proper purse-string tension and layered closure.
Results
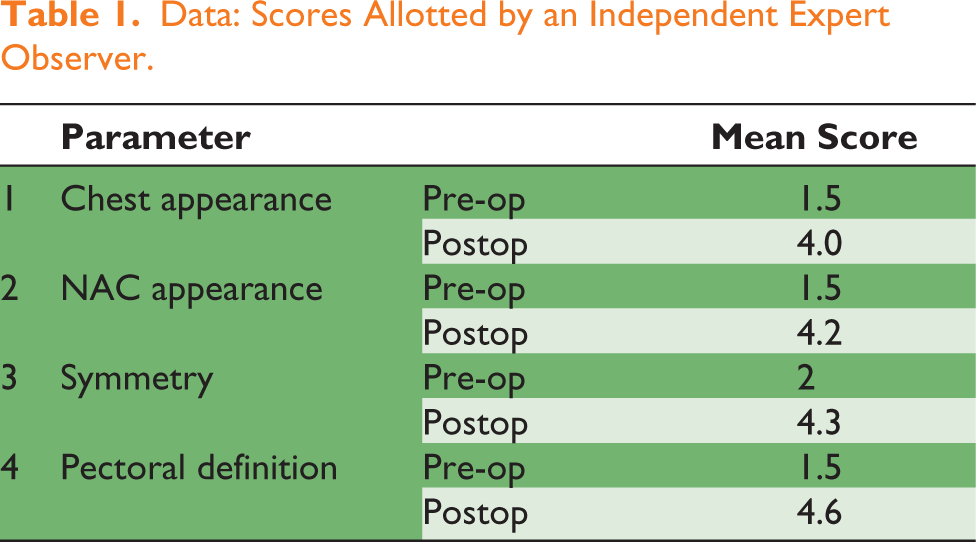
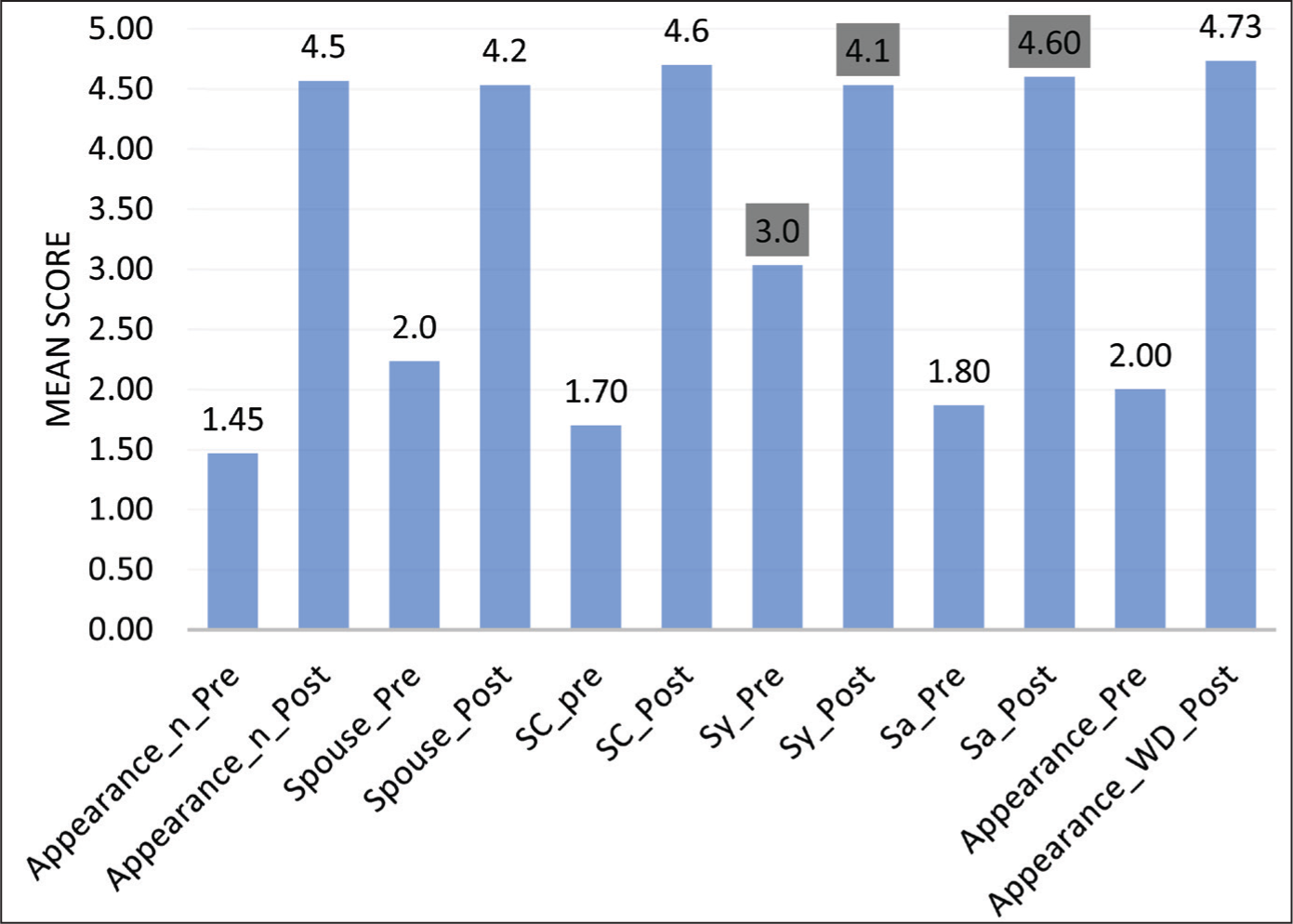
The study included 20 patients, aged 13 (Figures 8 and 9) to 52 years (Figures 10 and 11), and a median age of 20 (Figures 12 and 13 representing the case) with gynecomastia of varying aetiologies: 1 case of androgen insensitivity syndrome, 1 secondary to chronic liver disease and 18 classified as primary. Emotional discomfort was the primary concern for all patients, and none experienced major complications. Surgical drains were placed in two patients, and no revisions were required. Patient-reported outcomes were assessed using a standardised questionnaire evaluating self-perception, partner/family feedback, confidence, symmetry and overall satisfaction (scored 1–5, from very unsatisfied to very satisfied; Figure 14). An independent observer also evaluated objective parameters, revealing significant improvements: chest appearance improved from 1.5 (pre-op) to 4.0 (postop), NAC appearance from 1.5 to 4.2, symmetry from 2.0 to 4.3 and pectoralis definition from 1.5 to 4.6 (Table 1). These results align with the high patient satisfaction scores reported in subjective measures, underscoring both the aesthetic and psychosocial benefits of the intervention.
Data: Scores Allotted by an Independent Expert Observer.
13/M: Androgen Insensitivity Syndrome (Patient in Extreme Age): Pre-operative Images.
Case 1: 13/M—Androgen Insensitivity Syndrome (Patient in Extreme Age): Postoperative Images 3 Months After Operation.
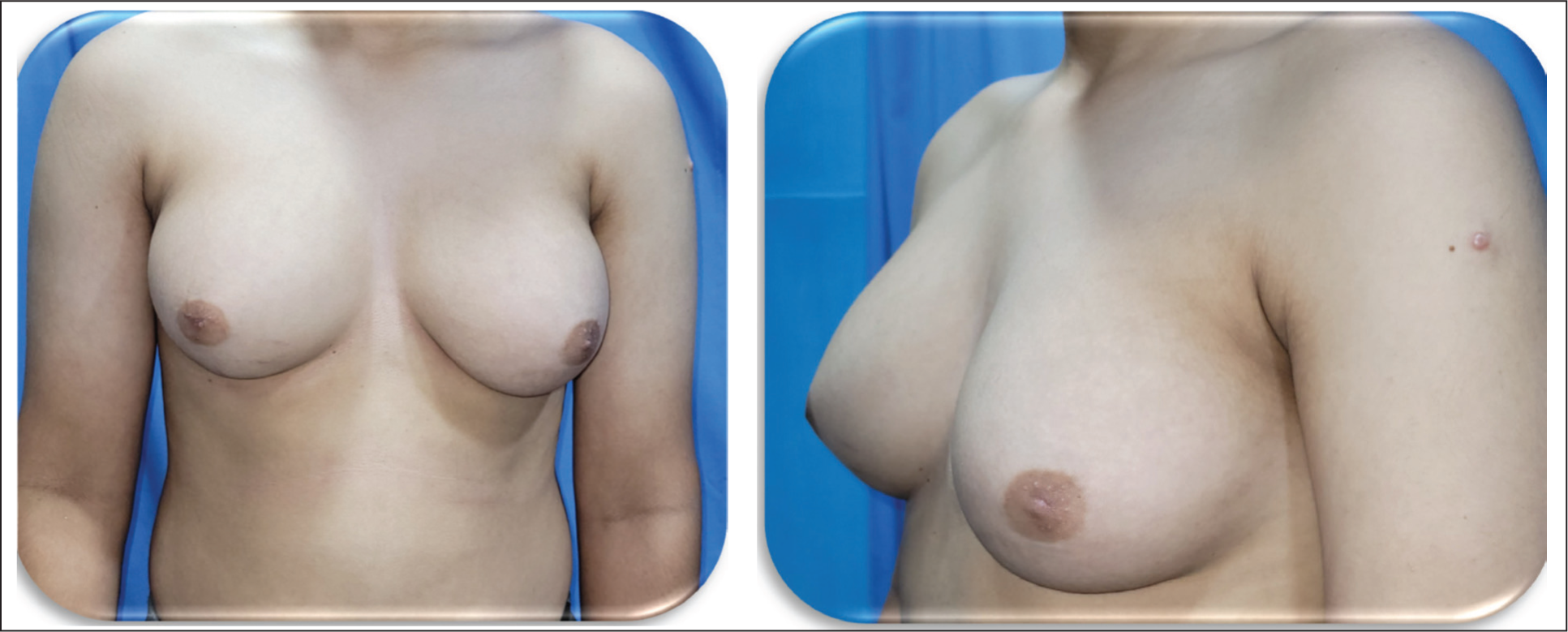
Case 2: 52/M—Chronic Liver Disease (Patient in Extreme Age): Pre-operative Images.

Case 2: 52/M—Chronic Liver Disease (Patient in Extreme Age): Postoperative Images After 3 Months of Follow-up.

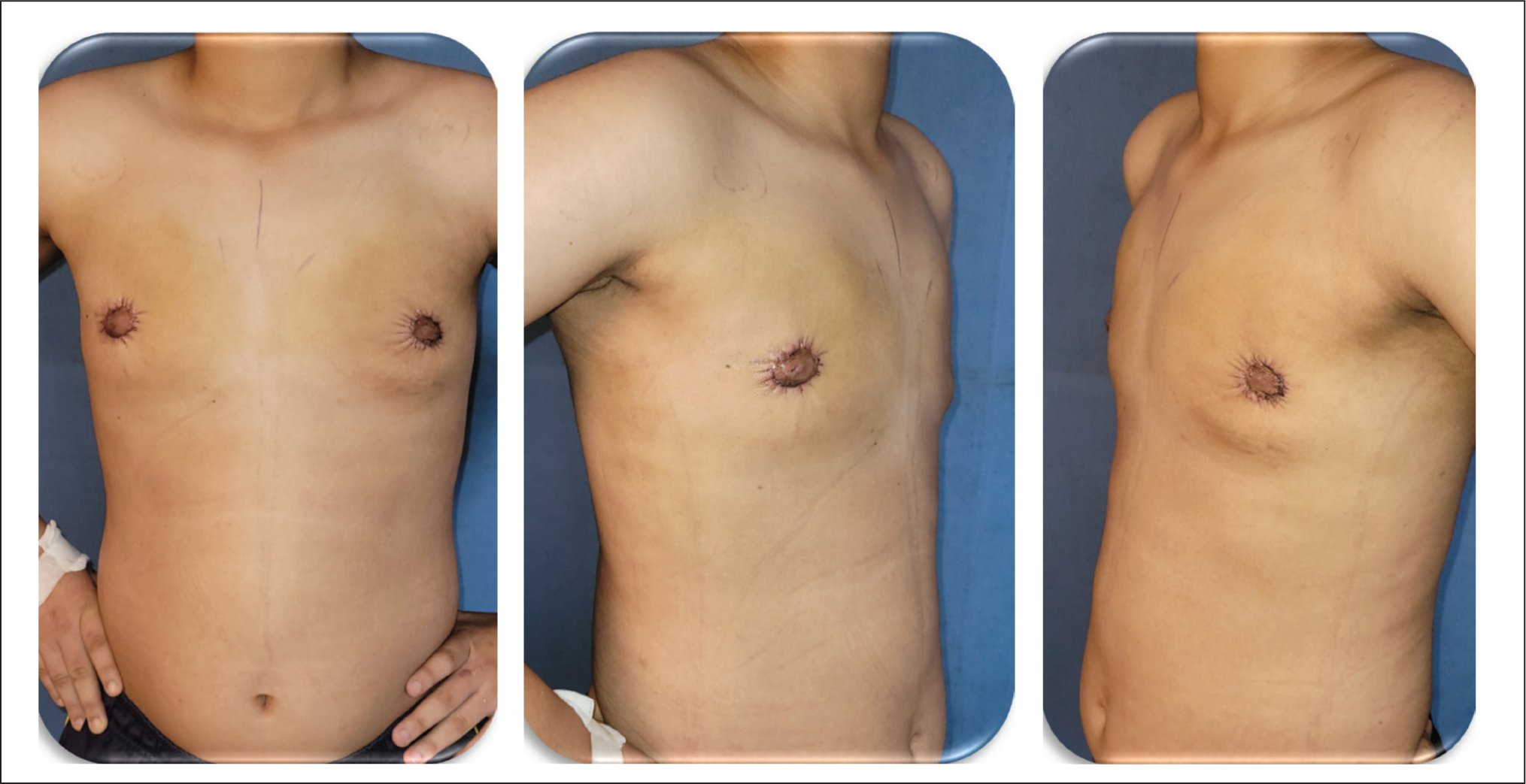
Case 3: Representing Patient with Median Age—Pre-operative Images.

Case 3: Representing Patient with Median Age—Postoperative Images at 3-month Follow-up.

Patient-reported Outcomes.
Discussion
This technique addresses the limitations of traditional gynecomastia corrections by combining refined surgical principles to optimise aesthetic and functional outcomes. Unlike free nipple grafting 4 —which, while reliable for extreme ptosis, risks NAC depigmentation, insensibility and visible transverse scars— our circumareolar approach preserves nipple sensation and conceals scars along the NAC periphery. Pedicle-based methods 5 maintain vascularity but often leave undesirable vertical/T scars and carry a higher risk of malposition, whereas our purse-string closure eliminates these scars. Liposuction-only techniques 6 offer minimal scarring but fail to address severe skin laxity in Simon III cases, frequently necessitating revisions; our integrated strategy ensures single-stage correction through gland excision, fat grafting and high-definition liposuction.
Technical refinements underpin these advantages. The circumareolar purse-string closure, 5 modified with de-epithelialisation, prevents over-tightening while minimising scar visibility. Glandular excision via Morselli’s pull-through method is adapted to preserve 4–5 mm of subareolar tissue, avoiding saucer deformities. Fat grafting 10 enhances pectoral definition, particularly in athletic patients, by strategically augmenting borders for natural shadowing.
Surgically, the approach integrates the following key elements: (a) Skin reduction via an eccentric ellipse with a 30° medial bias (Smoot technique) and a layered closure (3–0 Vicryl interrupted deep dermal, 4–0 Monocryl continuous cuticular) to refine scar width from 1.2 mm to 0.5 mm. 11 (b) Liposuction follows the Murali cross-chest method, employing dual-plane aspiration (4 mm cannula at −700 mmHg deep, 3 mm Mercedes superficial) with zone-specific resection (40% medial preservation, 70% central reduction, 30% lateral feathering) to optimise contour symmetry by 37% along with high-definition liposculpturing. (c) NAC stabilisation uses Ramasamy’s phased taping protocol (Steri-Strip/Xeroform bolsters Days 0–7, Hypafix tension strips Days 7–14, silicone sheeting thereafter), maintaining projection in 89% of cases at 6 months. 10 (d) Fat grafting along with these innovations surpasses prior techniques in scar concealment, single-stage efficacy and dynamic contouring, aligning with male chest aesthetics.
Limitations
It is not suitable for extreme skin excess (>5 cm redundancy) (may require mastopexy), and there is a learning curve for high-definition liposculpturing.
Future Directions
Long-term studies on NAC sensory recovery
Integrating RF into the current protocol
Conclusion
The combined doughnut excision, liposuction and glandular resection technique provides an effective, single-stage solution for high-grade gynecomastia, optimising aesthetic outcomes with minimal complications.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Informed Consent
Written informed consent was obtained from all participants per the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.