
Abstract
Background:
Gynecomastia is a benign, excessive development of the male breast that occurs at an overall incidence of 32% to 36%. The goals of surgical treatment are to restore the breast contour with minimal scarring and protect the areolar anatomy and sensation. Here, a new single stage technique is described where peripheral fat tissue is effectively removed using ultrasound-assisted liposuction (UAL) followed by a Dome breast lifting from the superior parabolic periareolar incision without touching the complex inferior pedicle.
Methods:
A retrospective review of outcomes for 29 patients aged between 18 and 49 years with grade IIB or grade III gynecomastia who were treated with UAL and the Dome technique. Health-related quality-of-life and aesthetic outcomes were evaluated using a modified version of the Breast Evaluation Questionnaire (BEQ).
Results:
The mean Likert-type score (LS) increased from 1.82 (18%) preoperatively to 4.10 (81%) months postoperatively (p < 0.05). No infection, nipple–areola complex necrosis, nipple retraction, or saucer deformity was encountered.
Conclusion:
The use of UAL and Dome technique for the treatment of severe gynecomastia allows for the effective removal of both the fat and glandular tissue of the breast through a minimal periareolar parabolic incision. This technique can achieve excellent aesthetic results with inconspicuous scarring in a single session.
Introduction
Gynecomastia is defined as persistent benign enlargement of the male breast. It results from proliferation of breast ducts and ductal epithelial hyperplasia, rather than excessive breast adipose tissue, the latter being a condition named pseudo-gynecomastia. Gynecomastia is a relatively common condition, with an incidence rate of approximately eight cases per 100,000 men, and it can present throughout all stages of life. 1 Gynecomastia moreover affects approximately 30% to 65% of adult men over 50 years of age. The cause is not fully understood, but it may be associated with testicular dysfunction in aging. Surgical resection of the periareolar glandular tissue is essential in the treatment of gynecomastia.2–4
Gynecomastia is usually bilateral, although 25% to 30% of patients have unilateral gynecomastia, or having one larger breast. 3 This condition can greatly impact a patient’s quality of life. During treatment, it is important to not only restore the breast contour but also leave minimal scars. 5
Simon et al. 6 developed a classification system for gynecomastia that was solely based on the amount of excess skin; grade I small enlargement with no excess skin; grade IIa moderate enlargement without skin excess; grade IIb moderate enlargement with minor skin excess; and grade III marked enlargement with extra skin. In 2003, Rohrich et al. 7 proposed a classification system for gynecomastia based on the amount of excess skin, fat, and glandular tissue.
Techniques used to treat gynecomastia include subcutaneous mastectomy, breast reduction, liposuction or a combination of these.8–10 The aim of this study is to describe a novel technique combining both open surgery and liposuction for treating grades IIB and III gynecomastia using only a periareolar approach that ends with a well-camouflaged scar within the nipple areolar complex. In addition, to evaluate the aesthetic results of this surgery, and assess the incidence of early and late postoperative complications.
Methods
Patients
The Dome technique was applied to 29 patients diagnosed with Simon stage IIB and III gynecomastia, who were admitted to the authors clinic between February 2019 and December 2023. Patients underwent a triple diagnostics preoperatively. No hormonal imbalances or abnormalities were shown in the preoperative examinations.
BMI was calculated for each patient, and gynecomastia was graded according to the Simon system. Patients were asked to not to use acetylsalicylic acid, ibuprofen, vitamin E, and tobacco for at least 10 days before surgery. Patients with pseudo-gynecomastia were excluded. Demographic characteristics, general medical history, family and medication history, motivations for surgery, complications, and other surgical details of all patients were recorded. Informed consent was signed by all the patients.
Comprehensive medical records for each patient were procured, encompassing preoperative laboratory data that included complete blood counts and coagulation profiles. The preoperative hormonal status, including the levels of luteinizing hormone (LH), follicle stimulating hormone (FSH), testosterone, estradiol, and human chorionic gonadotropin (hCG) were assayed in every patient. Endocrinology consultations were undertaken to eliminate potential hormonal issues, resulting in three patients being excluded from the study cohort.
Ultrasonography was performed in all patients to confirm the diagnosis of gynecomastia. Patients’ breasts were examined carefully to help determine the size and thickness of fibrous gynecomastia and the degree of sagging and elasticity of the skin was noted. The author (U.Z.) checked every patient for chest wall deformities during preoperative physical examinations.
Outcome measures were measured during outpatient visits through examinations and comparisons of preoperative and postoperative photographs.
Flap planning
An illustration of the Dome technique is shown in Fig. 1. Patient markings are performed with the patient in a standing upright position, with the hands freely on the sides. All anatomical landmarks were identified and marked (sternal notch, breast meridian, and inframammary fold). The anterior-axillary line laterally, the superior border of the breast footprint, the midsternal area neighborhood medially, and the area containing the inframammary fold inferiorly were marked as liposuction borders.
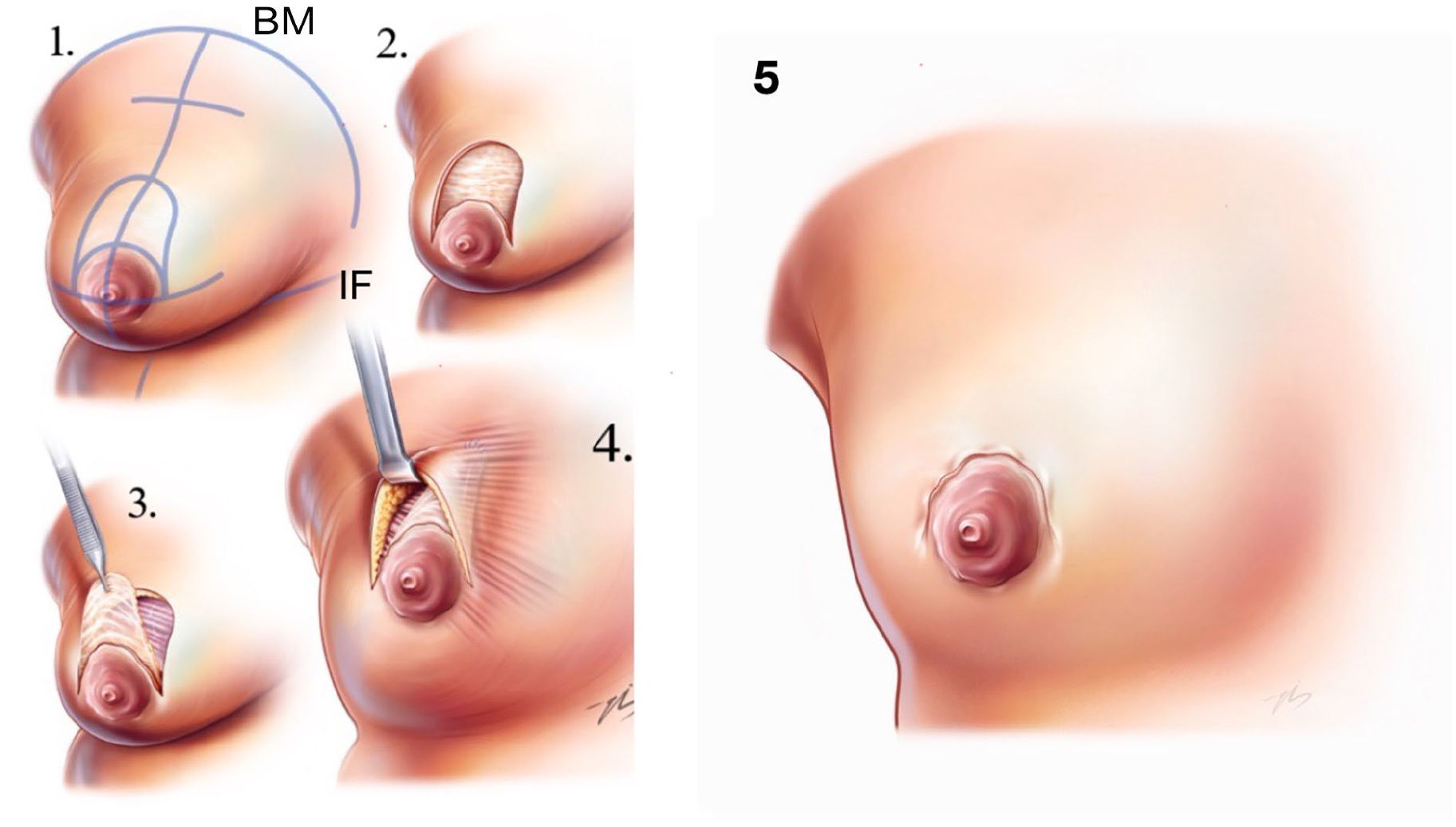
Illustration of the Dome technique; Anterior sectional view proliferated male breast showing combined use of suction-assisted liposuction and Dome technique. IF: Inframammary Fold, BM: Breast Meridian.
An oblique line was drawn from the midclavicular point to the inframammary fold, passing through the nipple. The location of the new nipple alignment was determined on the oblique midclavicular line as the midpoint between the apex of the deltoid muscle and the elbow when the arm is flexed. A line was drawn from the midpoint of the nipple areolar complex (NAC) dividing it into two equal parts (3 o’clock and 9 o’clock) on the horizontal plane. A parabolic dome was drawn starting from both sides of the intersection of the oblique line and the areola and extending to the new NAC position. This parabolic area (Dome area) was determined as the area to be de-epithelialized. Another point was drawn on an oblique line equal to the height of the parabola. This point was marked as the projection of the pectoral muscle fascia to which the complex inferior pedicled upper dermal flap containing the NAC would be fixed (Fig. 2).
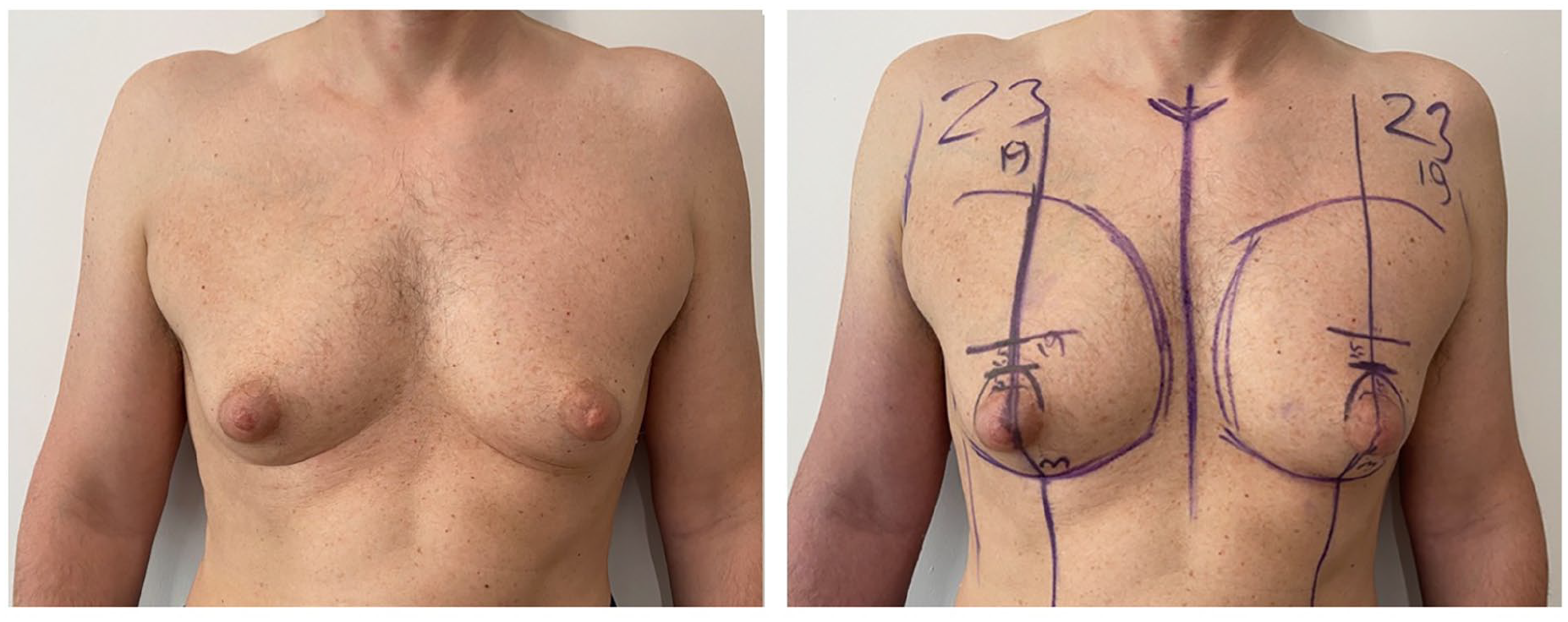
Dome technique markings on a patient in standing position; marked upper and lower border, nipple-midclavicular oblique line, parabolic dome, NAC horizontal line and markings of the new location of the flap.
Surgical Procedure
Surgery was performed under general anesthesia with a folded flat sheet placed under the shoulders to maintain the forward breast position. After the patient was administered an intravenous dose of antibiotics and antisepsis of the surgical field was performed (Fig. 3A). Ultrasound-assisted liposuction (UAL) of the breast was the first step in the technique. Infiltration with a tumescent solution comprising of 1000 mL normal saline or Ringer lactate solution with 1 mL of 1:1000 adrenaline. Generally, 400 to 500 mL of fluid was infiltrated subcutaneously into each breast for super wet tumescent liposuction (Fig 3B). Ultrasound-assisted liposuction (VASER) of the breast using a 3-mm Mercedes cannula was used. Initially liposuction of adipose tissue on the marked area of the mammary region was performed to smoothen the contour and liposuction ended after blood was observed in the aspirate or pinch test was adequate (Fig. 3C). Subsequently, an incision was made on the previously drawn periareolar parabolic marks, and the excess skin was de-epithelialized, while avoiding any damage to the vascular flow of the NAC (Fig. 3D). The previously drawn parabolic tissues were completely separated from the surrounding tissues. The muscle fascia was reached following a full-thickness incision on the upper part of the tissue to be de-epithelialized (
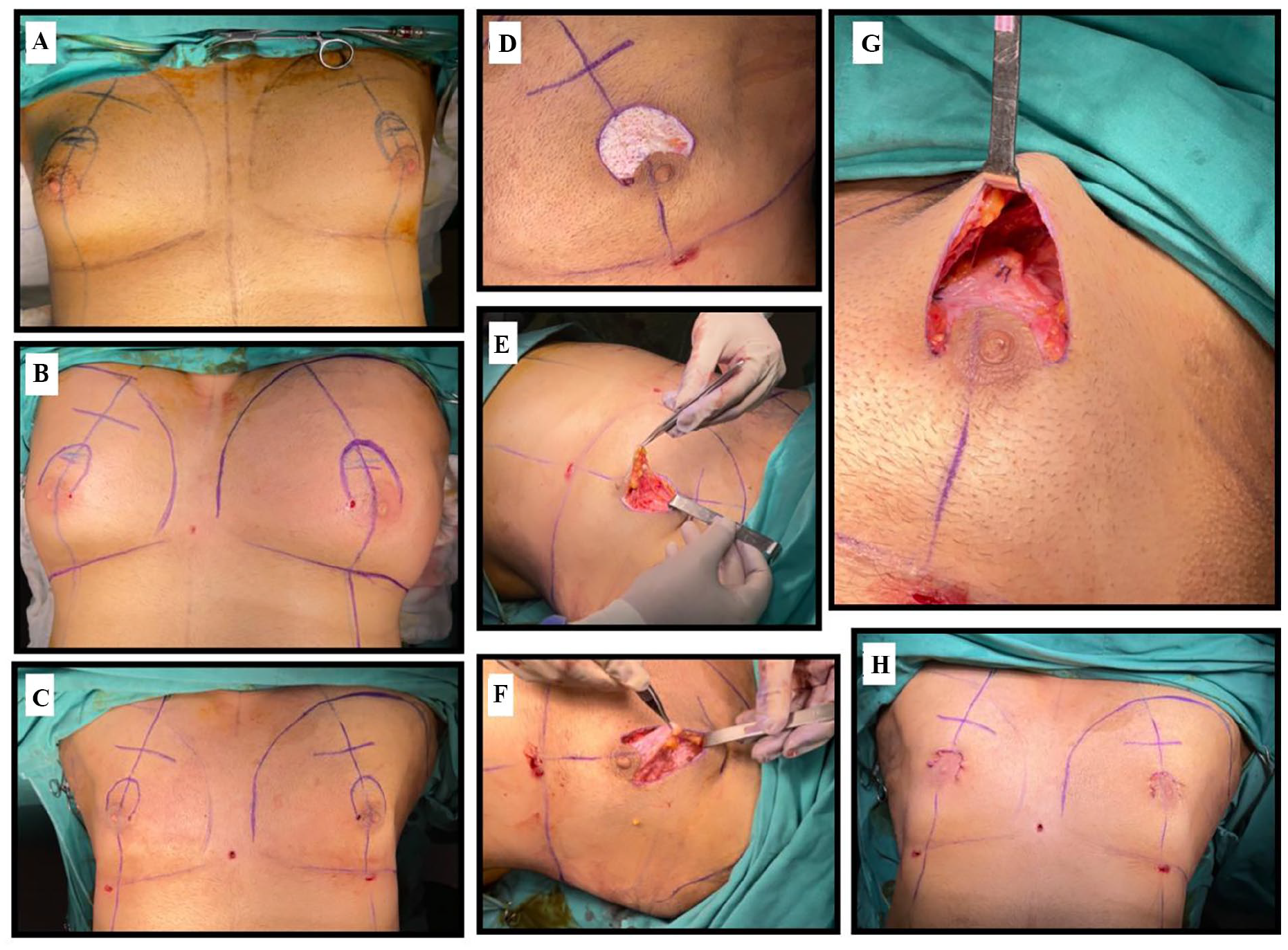
Steps of the operation; (
A complex inferiorly based NAC flap is created by incising the upper half of the circumareolar region from the 3 o’clock to the 9 o’clock position. It’s formed into a NAC flap with an inferior complex (skin-subcutaneous) pedicle and superior free dermal flap (Fig. 3G). Special attention was paid when freeing the inframammary fold from its attachment to the pectoralis fascia, which was performed by blunt dissection using a liposuction cannula. Remnant glandular tissue was resected. The thickness of this flap was 0.5 to 1 cm when proceeding upward to downward. The dissection continuing in a plane just beneath the NAC flap and above the rest of the breast tissue. After hemostasis was achieved with cautery and the pocket was irrigated with saline, an examination was performed to detect any remaining lumps in the tissue requiring resection. The inferior NAC pedicle was moved to its new location with the aid of a superior dermal flap, which was sutured to the muscle fascia using 2.0 vicryl sutures at 12, 3, and 9 o’clock positions in the same plane (
Elastic bandages were wrapped around the chest. The patient remained in the hospital for one night and was discharged the day after drain removals. Elastic bandages subjected to compression were applied for 3–4 days.
Follow-up
Patients were followed up at 4 weeks, 3 months, 1 year, and 2 years after surgery. Measurements of brassiere size and the distance from the sternal notch to the nipple were performed 4 months after surgery. Preoperative, early, and late postoperative pictures were taken.
Evaluation of quality of life and outcomes
There is no validated outcome assessment questionnaire specific to gynecomastia correction and male breast surgery in general. 8 In a recent study, Ridha et al. 11 assessed the HRQoL and surgical outcomes of patients who underwent surgery for gynecomastia and developed a modified version of the Breast Evaluation Questionnaire (BEQ). The BEQ is a validated 55-item questionnaire used to assess patient satisfaction with HRQoL outcomes following various breast surgery procedures. 12 The authors changed the gender approach of the questions to make them more appropriate for patients with gynecomastia. The questionnaire evaluated comfort with breast/chest size, in dressed and un-dressed conditions in different settings. Furthermore, patients were asked to score their satisfaction level with themselves and their partners on a 5-point Likert-type scale (1—very dissatisfied; 2—dissatisfied; 3—neither; 4 —satisfied; 5—very satisfied). Following the study by Ridha et al., 11 HRQoL in the present cohort was evaluated using the modified BEQ. Surveys were administered directly to the patients at the 1-year follow-up clinic visit.
Ethical considerations
This study adhered to ethical principles outlined in the Declaration of Helsinki and received approval from the relevant institutional ethics committee. As a retrospective analysis, all patients included in this study provided informed consent for both their participation and the use of their medical data, including preoperative and postoperative photographs, for academic and scientific publication purposes. Confidentiality and anonymity were strictly maintained throughout the study. The surgical procedures described were performed in compliance with established clinical guidelines, and no experimental or unapproved methods were utilized. All patients were fully informed about the scope and nature of the study and voluntarily agreed to the use of their data for research purposes.
Statistical analysis
Data was analyzed using SPSS 22.0 for Windows (IBM Corp., Armonk, NY, USA). Initially, all patient charts were reviewed to ensure informed consent for the study. The Student’s t-test was applied for parametric data analysis, whereas the Mann–Whitney U test was used for non-parametric data. Statistical significance was determined using a 95% confidence interval, and any group differences with a p-value < 0.05 were considered significant.
Results
Twenty-nine patients underwent surgery between February 2019 and December 2023 by a single surgeon (U.Z.) using the Dome method. Among the 29 patients operated, 22 patients were classified as having grade IIB, and seven patients were classified as having grade III gynecomastia (Table 1). A total of 24 modified BEQ questionnaires were returned giving an 82.7% overall response rate. Out of these 21 of 24 questionnaires were correctly completed. The three patients with incompletely filled questionnaires were excluded. Therefore, the final study cohort consisted 21 patients. Patients ages ranged from 18 to 49 years, with a median age of 30.25 years. Out of the 21 included patients, 17 were classified as grade IIB, and four patients were classified as grade III (Table 1).
Patient Characteristics.
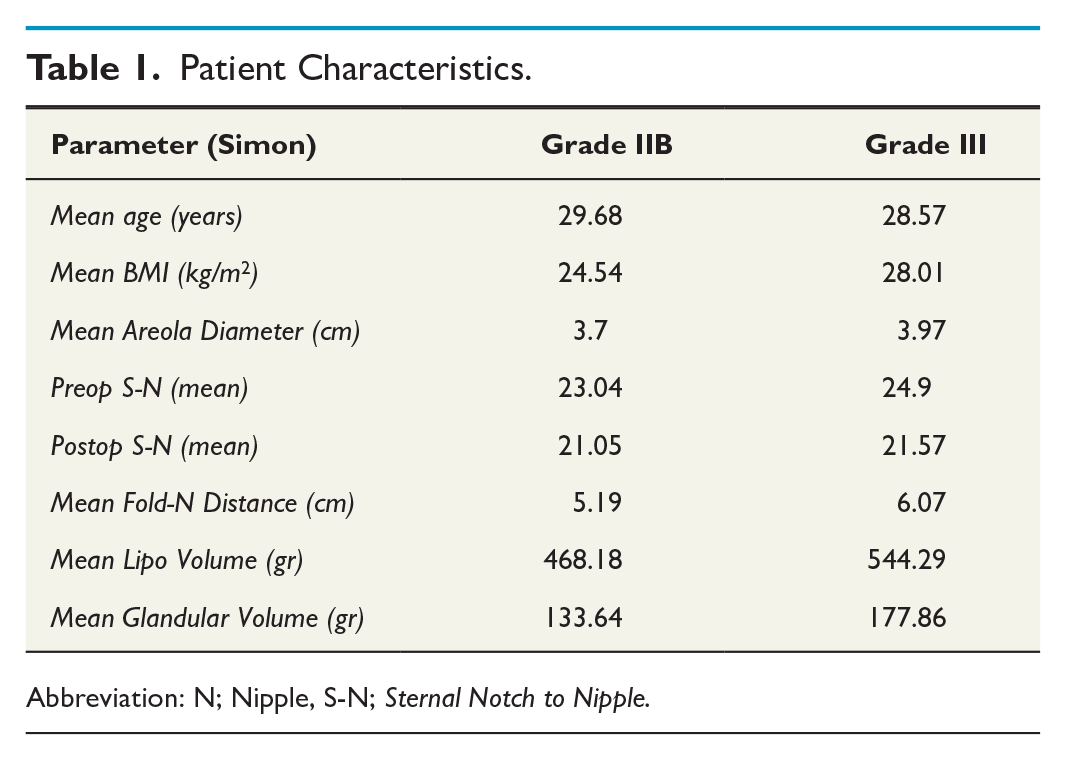
Abbreviation: N; Nipple, S-N; Sternal Notch to Nipple.
UAL was applied to all the 29 patients. The mean aspiration volume per breast was 460 mL and the mean weight of the resected glandular tissue was 140.3 g. Histologic examination of resection specimen revealed no malignancy. During follow-ups that ranged from 4 weeks to 2 years, three complications were noted: one hematoma, one asymmetry, and one numbness.
Overall, 61% of patients had more than one reason for undergoing surgery. Most patients (80%) underwent surgery for self-confidence and emotional distress caused by gynecomastia (Fig. 4). Only a minority of patient underwent surgery for pain or discomfort. Two patients felt that their gynecomastia affected their ability to gain employment and two found that it affected their ability to play sports. The mean Likert-type scores (LS) for each question in the modified BEQ questionnaire, both preoperatively and postoperatively, are shown in Fig. 4. The graphs show that surgery led to an increase in the mean LS in all surgical patients. The mean LS increased from 1.82 (18%) preoperatively to 4.10 (81%) postoperatively (p < 0.05).
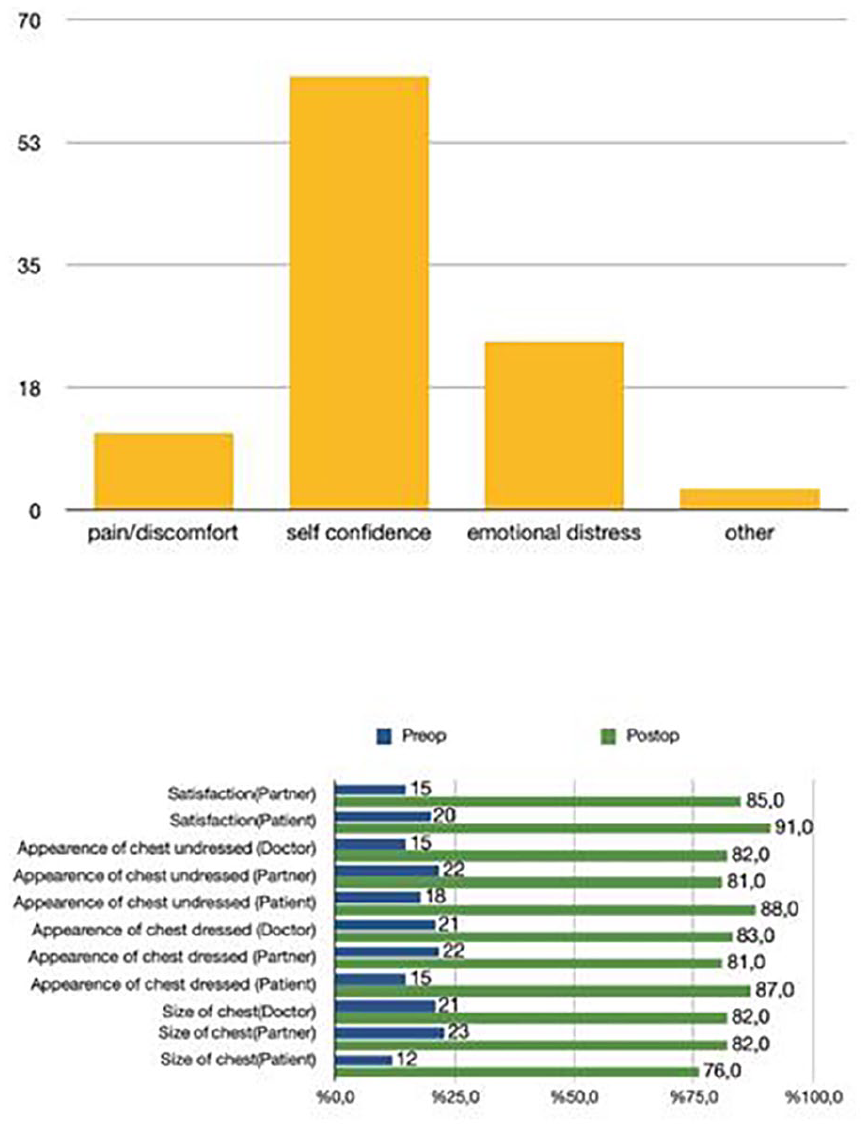
Patient reasons for undergoing gynecomastia surgery (Upper part). Preoperative and postoperative satisfaction of all patients are shown (Lower part) displayed with a mean Likert-type score (%) of the modified BEQ questionnaire.
Scar appearance was scored as excellent in 20 patients. The scars on the superior areolar margin were barely recognizable (Supplemental Figure 1). No hypertrophic scarring or NAC necrosis were observed. In two cases, minor contour problems near the areola were recorded. No other complications were noted. Figure 5

A 49-year-old patient treated with liposuction and Dome technique. (Upper panels) Preoperative views; (Lower panels) Postoperative views after 1 year.
Discussion
Several surgical trials have been performed to correct gynecomastia. Various incisions and surgical techniques have been described, 13 including Webster’s intra-areolar incision placed inside the inferior border of the NAC and a peri areolar incision along the inferior margin of the skin and areola. 14 In grade I gynecomastia, minimal incision techniques such as liposuction and/or the pull-through technique for glandular tissue excision are sufficient, whereas in grade III gynecomastia skin excision is required. Over the years, numerous approaches to resecting excess skin have been described. The skin can be removed as an ellipse, with the nipple transposed on a pedicle or repositioned as a full-thickness graft.15,16 Redundant skin has also been excised concentrically around the nipple to avoid extra-areolar scarring, keeping it on a superior or central pedicle.17–19 All these reduction-mastopexy techniques are still used in patients with grade III or postbariatric gynecomastia.
Here, a minimally invasive method combined with limited skin excision, that can be well concealed, is described. This method can be an option for patients with grade IIb and III gynecomastia. To avoid possible complications many previous methods have initially used liposuction/surgery and fat/glandular tissue excision initially and removed excess skin in a second session. Multiple procedures are however disadvantageous in terms of increased hospitalizations, costs, and labor.20,21
Some authors have used free nipple grafts in Simon grade III patients to prevent NAC necrosis. 8 In all previously described surgical models, the skin flap and the NAC-glandular flap were dissected separately, which cause prolonged surgical times and varying NAC necrosis rates depending on the surgeon experience. 22 In the present technique, the skin and glandular tissue were not dissected separately, and no ischemia was observed in NAC circulation. The authors believe that the inferior dermo-glandular complex pedicle (Dome technique) using vessels 6 o’clock is enough to supply the NAC even in patients with Simon grade III gynecomastia. In addition, meticulous liposuction may prevent damage to the inferior pedicle. After UAL, the inferior pedicle skin had a more reliable blood supply as it was moved upward by preparing the dermo-glandular complex flap without dissection. Another important feature that distinguishes the present technique from others is that it provides closure without skin tension, despite being a peri areolar technique. No necrosis, including partial necrosis, was observed.
Even in patients with mild gynecomastia, there remains fatty or glandular tissue after liposuction or gland excision. Techniques, such as female reduction mammoplasty, often have disadvantages, including long and unacceptable scarring of the male thorax and coning of the breast in wise pattern reductions.23-25 In the present series using the parabolic-dome excision, no coning or female pattern bulk areolas were observed.
Excessive skin undermining or large incision techniques lead to delayed healing. 26 Delayed wound healing did not occur in the present series because skin undermining was avoided. When the excision was deep into the skin, minimal dissection of breast tissue was carried out laterally and superiorly and the upper skin flaps were maintained at least 0.5 cm thick throughout their length and the inferior pedicle did not have too much lateral traction.
The upper skin flap is elevated between the subcutaneous tissue and scarpa fascia. 27 The subdermal plexus can be preserved which minimizes sensory loss. While venous congestion can be seen in the central, superior pedicle or purse string technique, it was not encountered in the present technique. 28 There is moreover an excellent field of view and thus bleeding can be easily controlled with a lower risk of hematoma compared to pull-through and other uncontrolled techniques. The surgical time was short, and the learning curve is easy.
Originally, small periareolar incisions were published by Morselli 29 and some authors described small incisions in the inferior breast fold, some in the axillary region. 26 The most important advantage of the pull-through technique is to remove glandular tissue from a simple incision with minimal scarring. The most important disadvantage over the Dome technique is that it cannot move the position of the NAC upward and cannot repair asymmetric NACs. The superior aesthetic results of the present method can be attributed to the conservative approach of removing the tissues just above the nipple. This approach is primarily applicable to patients with excessive ptosis and excess skin. The technique is versatile, effective and can achieve male chest contouring with minimal inconspicuous scarring. Despite this obvious advantage, the most important disadvantage of this technique is upper pole step-off deformity.
Conclusion
With the use of UAL and the Dome technique in the treatment of gynecomastia, both fat and glandular tissue of the breast can be effectively removed through an acceptable scar using a periareolar incision. Excellent aesthetic results can be achieved in term of thoracic contour and scar quality.
Supplemental Material
sj-jpg-1-sjs-10.1177_14574969251363334 – Supplemental material for The Dome technique: A single-stage liposuction and dermopexy treatment for high-grade gynecomastia
Supplemental material, sj-jpg-1-sjs-10.1177_14574969251363334 for The Dome technique: A single-stage liposuction and dermopexy treatment for high-grade gynecomastia by Umut Zereyak and Onur Aksoy in Scandinavian Journal of Surgery
Supplemental Material
sj-jpg-2-sjs-10.1177_14574969251363334 – Supplemental material for The Dome technique: A single-stage liposuction and dermopexy treatment for high-grade gynecomastia
Supplemental material, sj-jpg-2-sjs-10.1177_14574969251363334 for The Dome technique: A single-stage liposuction and dermopexy treatment for high-grade gynecomastia by Umut Zereyak and Onur Aksoy in Scandinavian Journal of Surgery
Supplemental Material
sj-jpg-3-sjs-10.1177_14574969251363334 – Supplemental material for The Dome technique: A single-stage liposuction and dermopexy treatment for high-grade gynecomastia
Supplemental material, sj-jpg-3-sjs-10.1177_14574969251363334 for The Dome technique: A single-stage liposuction and dermopexy treatment for high-grade gynecomastia by Umut Zereyak and Onur Aksoy in Scandinavian Journal of Surgery
Supplemental Material
sj-jpg-4-sjs-10.1177_14574969251363334 – Supplemental material for The Dome technique: A single-stage liposuction and dermopexy treatment for high-grade gynecomastia
Supplemental material, sj-jpg-4-sjs-10.1177_14574969251363334 for The Dome technique: A single-stage liposuction and dermopexy treatment for high-grade gynecomastia by Umut Zereyak and Onur Aksoy in Scandinavian Journal of Surgery
Footnotes
Authors’ Note
The author declared no use of AI or AI-assisted technologies in the writing process.
Author contributions
Study design, manuscript writing, and critical revision were performed by U.Z. and O.A. Acquisition of data analysis was contributed by U.Z. and O.A.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Compliance with ethical standards
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
Informed consent was obtained from all patients.
Statement of human and animal rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.