
Abstract
Introduction:
Rhinoplasty is an aesthetic procedure which requires precise surgical techniques for preservation of delicate bone and soft tissues. Prolonged edema, ecchymosis and pain in postoperative period caused by soft tissue damage is very unpleasant for the patient. Over the time, advancement of using piezoelectric instrumentation in rhinoplasty has been found to be safe, delicate and accurate in comparison to manual instrumentation.
Objectives:
To observe the postoperative outcomes in patient undergoing piezoelectric rhinoplasty.
Methodology:
All patients were assessed during post-operative period (Day 1, 7, 30 and 90), for the level of edema, ecchymosis and pain as per Kara et al., Caglar et al. and Numerical Rating Scale (score 1 to 10) respectively.
Results:
Our observation in 13 patients revealed mean scores as Kara score (1.80 0.82), Caglar score (3.73 2.73) and NRS score (3.07 0.76) on post-operative day 1. The mean scores decreased on further follow up at post-operative day 7 and completely resolved on subsequent follow ups at one month and three months.
Introduction
Rhinoplasty is one of the most common plastic surgery procedures around the world. Most rhinoplasties demand bony correction for adequate results, which requires the use of mechanical instruments like saws, osteotomes, chisels and rasps. Precise surgical techniques are required to preserve the delicate bony and soft tissues.1–4 Over the past decades, continuous refinement in instrumentation and technology has been done in an attempt to achieve better post-operative outcomes. The role of power instruments in rhinoplasty is still debatable.
As we all know, osteotomy is considered to be the most vulnerable process in rhinoplasty as it demands great precision. Indications of osteotomy include open roof deformities, post-hump removal correction, thinning of the nasal pyramid, removal of asymmetry and straightening of the nasal bones. Osteotomy of the nasal bone can result in soft tissue damage, causing oedema and ecchymosis after surgery. The use of piezosurgery in rhinoplasty is one of the recent advances in mechanical instrumentation used for bony correction.4–7 In patients operated on with a piezoelectric device, the vibrations are generated by an electrically applied piezoceramic transducer, which is utilised in cutting bones through various tips. 8
Piezoelectric surgery was originally used for the first time in 1975 by Horton for alveolar bone surgery. However, its use in rhinoplasty was first introduced by Robiony in 2007 for lateral osteotomy or dorsum hump reduction. 9 They described the piezo instrument as a precise and easily manageable device with increased visibility intraoperatively and less post-operative complications like oedema and ecchymosis. Since the introduction of piezosurgery in rhinoplasty by Robiony, 9 it has been used in various clinics. Tirelli et al. have compared external perforating osteotomy with piezosurgery, 10 and their results revealed less post-operative oedema and ecchymosis in piezo patients. Even after these reports, there is still no agreement regarding the superiority of either method. Although in some systematic reviews it was concluded that post-operative oedema, ecchymosis and pain were less in piezosurgery without increasing the duration of surgery. Despite the potential advantages of less post-operative oedema, ecchymosis and pain, the use of the piezosurgery device is not widespread. This could, however, be secondary to its higher cost and longer learning curve.11–15 The present study was designed to describe the use of piezoelectric surgery for bony correction in rhinoplasty. It also describes the intraoperative feasibility of using the piezosurgery device as well as post-operative outcomes in an elaborate manner.
Patients and Methods
This prospective observational study was conducted in the Department of Plastic Surgery in a tertiary-level hospital in northern India. The study duration was 18 months, and it was conducted after taking approval from the institutional ethical committee. Patients presenting with nasal deformity requiring bony correction as part of rhinoplasty were enrolled. Demographic and clinical details, including mode and circumstances of injury and examination findings, were noted for all patients in a predesigned proforma. All patients were photographed in standard views using the same camera (f/1.7, 0.8 µm/48 M) at a uniform distance and constant background (Figures 1 and 2). The study was conducted as per STROBE guidelines.
Patient (Case 1) Photographs from Front Angle, from Left to Right: Pre-operative, Post-operative Days 1, 7 and 30, Respectively.

Patient (Case 2) Photographs from Front Angle, from Left to right: Pre-operative, Post-operative Days 1, 7 and 30, Respectively.

Surgical Procedure
The nasal cartilaginous framework was exposed using an open approach and supra-perichondrial dissection. Once the keystone region was visualised, dissection proceeded in the subperiosteal plane up to the radix. Transverse dissection was done from one frontal process of the maxilla to the other side. Such an approach provided a wider view for bony correction. Bony correction was done with the piezosurgical bone scalpel (Misonix™; Misonix Inc., New Highway, Farmingdale, NY). The device has an ultrasonic console with a nominal frequency of 22.5 kHz. A blunt 10 mm right-angled blade (Figure 3) was used with a short extension and silicone sleeve. Dorsal bony reduction was carried out using the piezosurgery device. Precise control could be achieved without causing visible damage to the underlying cartilage and mucosa. As bony hump reduction was incremental, there was less incidence of open roof deformity. Whenever indicated, osteotomy was done using the piezosurgical device. In most cases, we performed osteotomy in a sequential manner—starting with low to low lateral osteotomy, followed by transverse and medial oblique osteotomy. Once osteotomies were done, bony flaps were medialised. Reconstruction of the middle third involved exposure of the septum by separating mucoperichondrial flaps on either side. Septal reduction was done, leaving an L-shaped strut dorsally and caudally. Once the upper lateral cartilage (ULC) was separated from the septum, repositioning was done using either a spreader flap or a spreader graft to avoid internal nasal valve collapse. After ensuring adequate haemostasis, closure was done followed by nasal packing and splintage.
Right-angled Piezotome.

Post-operative Care
In the post-operative period, patients were given non-anti-inflammatory analgesics on an SOS basis. The nasal splint was kept in place till post-operative day 7. Patients were nursed in a recumbent position with the head end up. Assessment was done on day 1 for pain, periorbital oedema and ecchymosis by a single observer using Kara et al score 16 and numerical rating scale (NRS) score, 17 respectively. All patients were discharged on post-operative day 2 and re-assessed on day 7 for suture and nasal splint removal. Further follow-ups were done at 1 month and 3 months. The data were analysed using SPSS version 22. Descriptive statistics in the form of mean scores were depicted.
Results
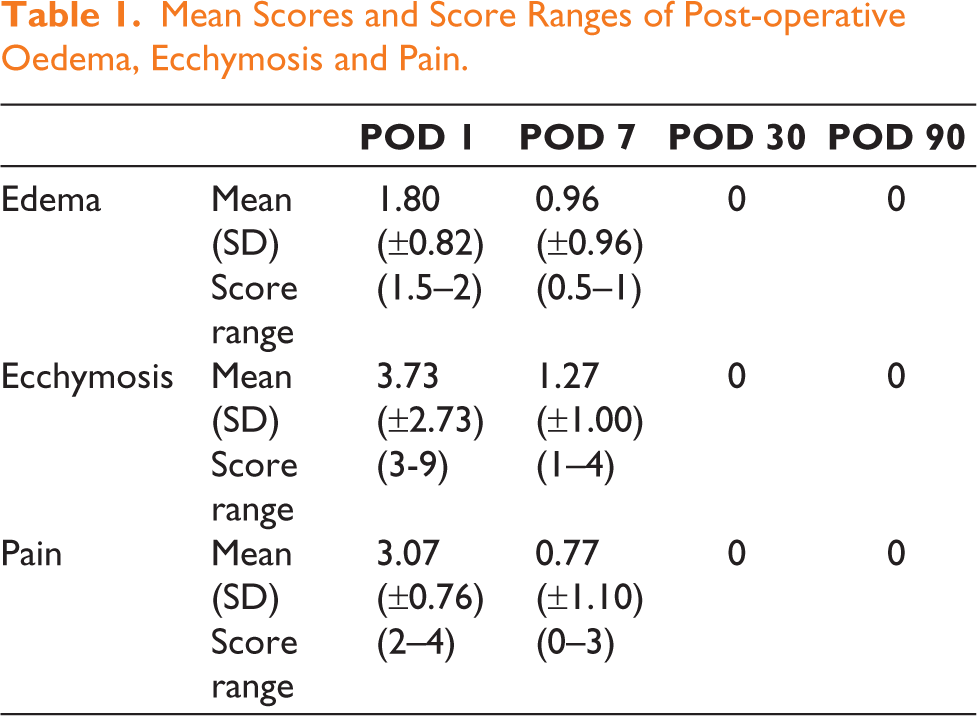
A total of 13 patients were enrolled in the study after taking consent, with an age range of 17–35 years (mean age 24.76 years), 9 male and 4 female patients. All patients underwent the surgical procedure as mentioned in materials and methods. During their post-operative follow-up assessments, mean scores for periorbital oedema, ecchymosis and pain were noted as 1.80 (± 0.82), 3.73 (± 2.73) and 3.07 (± 0.76) on post-operative day 1, which declined to mean scores 0.96 (± 0.96), 1.27 (± 1.00) and 0.77 (± 1.10) on post-operative day 7, respectively, as shown in Table 1. No appreciable periorbital oedema, ecchymosis and pain was noted on post-operative days 30 and 90.
Mean Scores and Score Ranges of Post-operative Oedema, Ecchymosis and Pain.
Intraoperative Observations
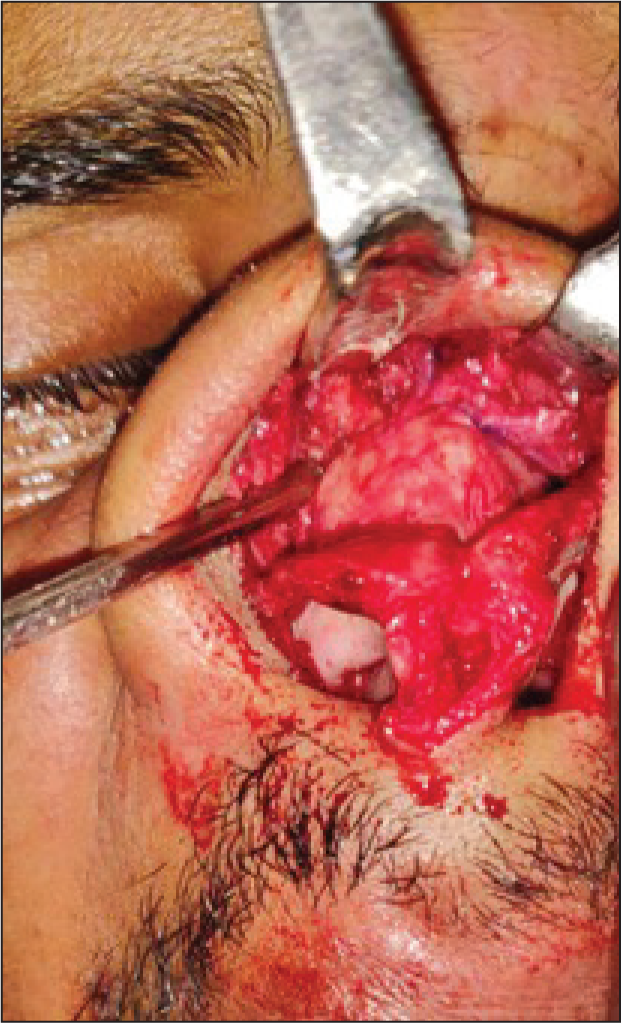
Misonix™ ultrasonic bone scalpel was used as the piezosurgical device. During the operative procedure, we noticed the following benefits of the equipment (Figure 4): (a) It was easy to follow pre-marked osteotomy lines precisely without causing negligible radiating fracture lines; (b) there was controlled cutting of bone with efficient cooling at the surgical site with minimal bleeding; (c) there was no visible damage to the underlying nasal mucosa; (d) right-angled osteotome allowed precise sculpting of the nasal dorsum; (e) it allowed direct visualisation of the operative area and hand fatigue was minimal.
Intraoperative Field Showing Selective Act on Bones, Preserved Skin, Mucosa, Cartilages and Accurate Fracture Lines.
Discussion
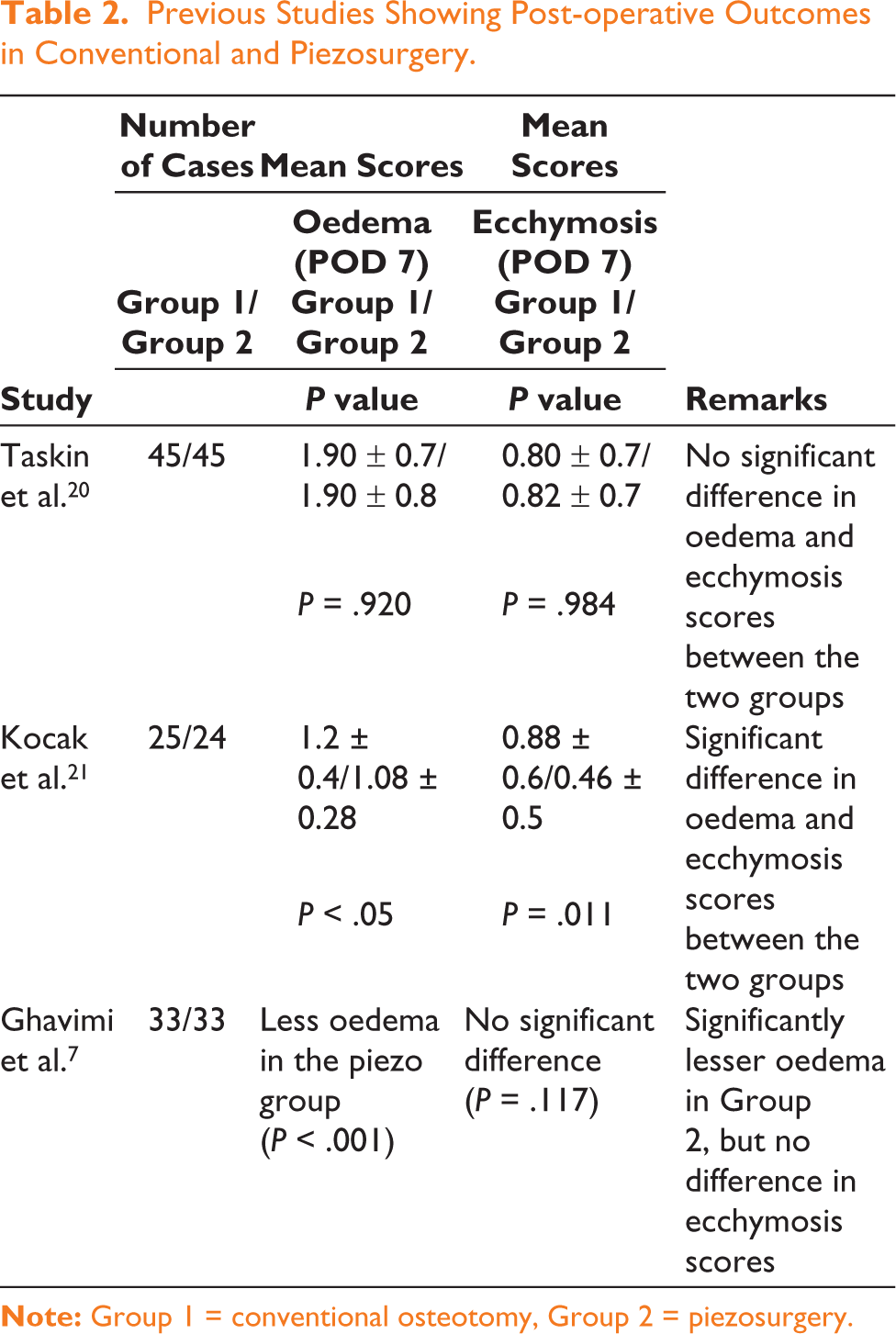
Rhinoplasty is one of the most challenging aesthetic procedures, which require precise surgical techniques for the preservation of delicate bone and soft tissues. Bony vault remodelling during rhinoplasty involves incremental dorsum reduction, spur excision, nasal spine and maxillary crest reduction, and finally osteotomies. The indications of osteotomy are correction of open roof deformity and a wide upper third base. Piezosurgery or ultrasonic instrumentation is an important advancement in performing osteotomy during rhinoplasty. Owing to incremental bony reduction, there is relative protection of the underlying cartilage. This causes less disruption of the ULC at the keystone area and allows bony reduction without producing open roof deformity. A common complication of ‘step off’ at the keystone area following the conventional bony reduction technique was also found to be lower with piezosurgery. Piezosurgical instrumentation is easier to use for lateral osteotomies. Robiany et al. reported that peri-operative haemorrhage and post-operative oedema and ecchymosis were less with the use of the piezo instrument. 9 Also, in our patients, we noticed less requirement of medial osteotomy as piezosurgery allowed precise reduction of the bony dorsum. Ozucer et al. reviewed current concepts of osteotomy in rhinoplasty and concluded that conventional osteotomy techniques using saws and rasps are non-selective and non-precise. The conventional approach leads to partially mobilised osteotomy segments, because of which manual pressure is applied to medialise the segments, causing more post-operative ecchymosis and oedema. 18 Koc et al. performed a prospective comparative study to compare piezosurgery versus conventional lateral osteotomy. Their results showed significantly lower scores of post-operative oedema, ecchymosis, pain and haemorrhage on post-operative days 1 and 7 in the piezosurgery group. No subperiosteal tunnels were made, and the underlying nasal mucosa was spared in all piezosurgery cases. 19 Similarly, a few more studies have been done to compare the post-operative outcomes in two groups (conventional vs. piezosurgery).7,20,21 Some studies showed significantly lower scores of pain, oedema and ecchymosis post-operatively in piezo patients, while other studies reported no significant difference between the two groups (Table 2). However, bleeding, symmetry of the pyramid and presence of external scars were similar in both groups.10,19,21
Previous Studies Showing Post-operative Outcomes in Conventional and Piezosurgery.
In our study, we performed rhinoplasty using the piezosurgical device in 13 patients. Intraoperatively, the piezosurgical device was more feasible than conventional instruments. There was better visualisation due to continuous irrigation and less blood loss. Precise bone cutting was possible without causing visible soft tissue damage. It was observed that post-operative oedema, ecchymosis and pain scores were highest during post-operative day 1, which decreased on day 7 and completely resolved on further follow-up till 3 months. The mean scores for oedema, pain and ecchymosis on days 1 and 7 were lower compared to other studies in which conventional methods were used. The present study had two major limitations: the sample size was small, and it was not a comparative study between the piezosurgery and conventional surgery groups. We hope that the results of this study will encourage surgeons to use piezosurgery in rhinoplasty.
Conclusion
Ever since the advent of modern rhinoplasty, many conventional and motorised techniques have been devised. Conventional techniques using osteotomes/saws/rasps cause more soft tissue injury, leading to increased periorbital oedema, ecchymosis and pain in the early post-operative period. It showed that piezosurgery allows for a bloodless field and better visualisation throughout the bony sculpting process without causing radiating fracture lines and reduced antecedent soft tissue injury intraoperatively. Also, immediate cooling of tissues with continuous saline irrigation ensures reduced collateral damage to soft tissues, and the underlying mucosa is protected. Future studies with larger sample sizes and comparative groups (piezosurgery vs. conventional surgery) are required to evaluate the role of piezosurgery in rhinoplasty.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical approval was obtained, for the research from institutional ethical committee prior to starting the research. Approval no- INT/IEC/2019/1500550 dated 16th march 2019.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Patient consent was taken for use of photos for the purpose of follow up and publication (given that the identity is not revealed).