
Abstract
Introduction:
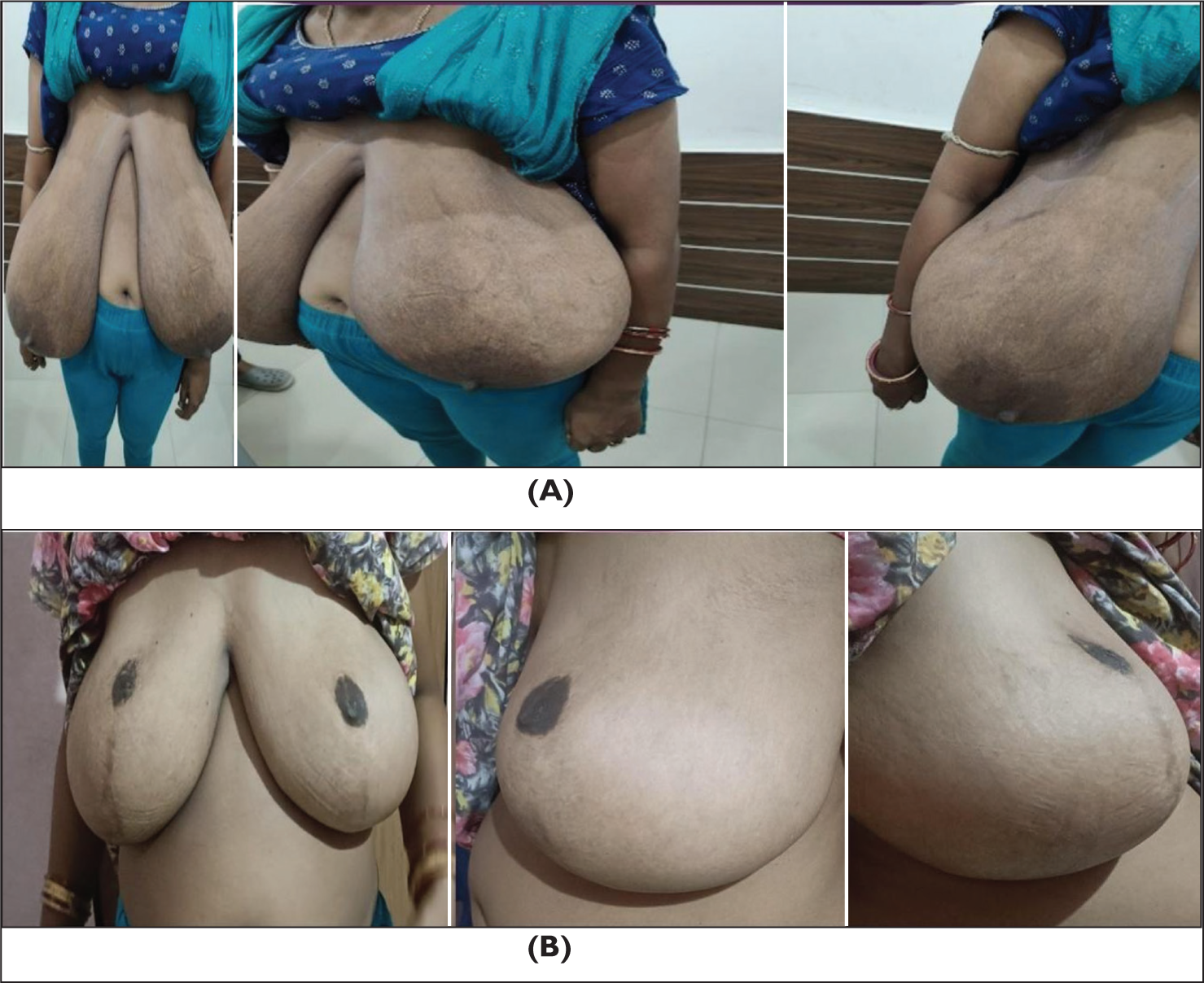
Gigantomastia, or breast hypertrophy, is a rare condition characterised by excessive breast tissue growth, leading to significant physical and psychological distress. Inferior pedicle reduction mammoplasty (Goldwyn & Courtiss, 1990, Plast Reconstr Surg, 255–266) is a well-established technique for addressing this condition, ensuring adequate blood supply to the nipple–areolar complex (NAC) while achieving substantial volume reduction and aesthetic improvement.
Patients and Methods:
This retrospective study included 35 women who underwent inferior pedicle breast reduction between 2007 and 2024. The procedure was performed using a Wise-pattern skin incision. Standard preoperative markings guided tissue resection while maintaining a well-vascularised inferior pedicle to sustain NAC viability.
Results:
All patients experienced a reduction in breast volume with sustained NAC sensation (Baslaim et al., 2018, Plast Reconstr Surg Glob Open, 6, e1798), breast projection and shape. The mean tissue resection ranged from 600 g to 1.2 kg per breast. Complications included bottoming-out in three patients, high positioning of the NAC in one patient and partial NAC necrosis in one patient. The average follow-up period was 12 months, with high patient satisfaction scores regarding appearance, reduction in symptoms and quality of life.
Conclusion:
Inferior pedicle reduction mammoplasty is a reliable and versatile technique that balances volume reduction, aesthetic outcomes and preservation of NAC vascularity. The technique provides long-term symptomatic relief and functional benefits while ensuring aesthetic harmony.
Introduction
Gigantomastia is a rare disorder characterised by rapid and excessive growth of breast tissue, leading to significant discomfort, including neck and back pain, postural issues and social embarrassment. 1 Several surgical techniques have been employed for reduction mammoplasty, with the inferior pedicle method 2 emerging as one of the most effective approaches due to its ability to preserve nipple–areolar complex (NAC) viability and ensure aesthetic symmetry.
This study evaluates the clinical outcomes of patients who underwent inferior pedicle reduction mammoplasty using an inverted-T skin closure technique. The objective was to assess the safety, effectiveness and long-term viability of the procedure in achieving symptom relief and aesthetic enhancement. 3
Patients and Methods
This retrospective study included 35 female patients diagnosed with gigantomastia who underwent inferior pedicle breast reduction between 2007 and 2024. Indications for surgery included symptoms related to macromastia, such as chronic pain, difficulty with physical activities and psychological distress.
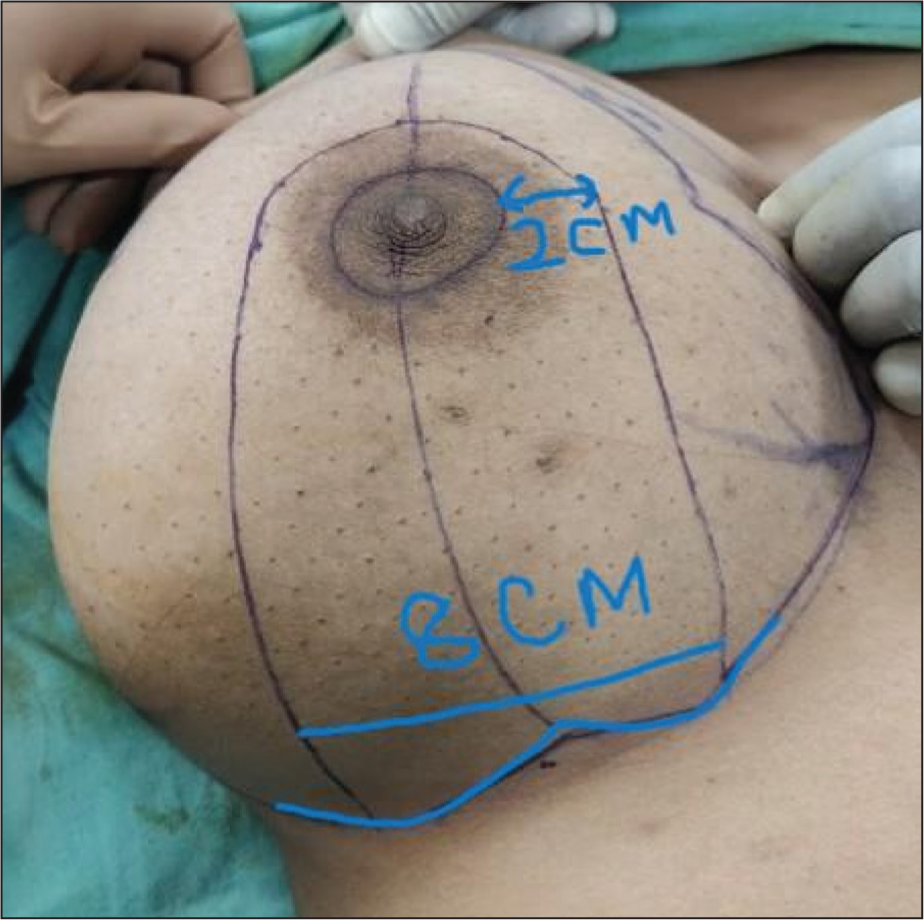
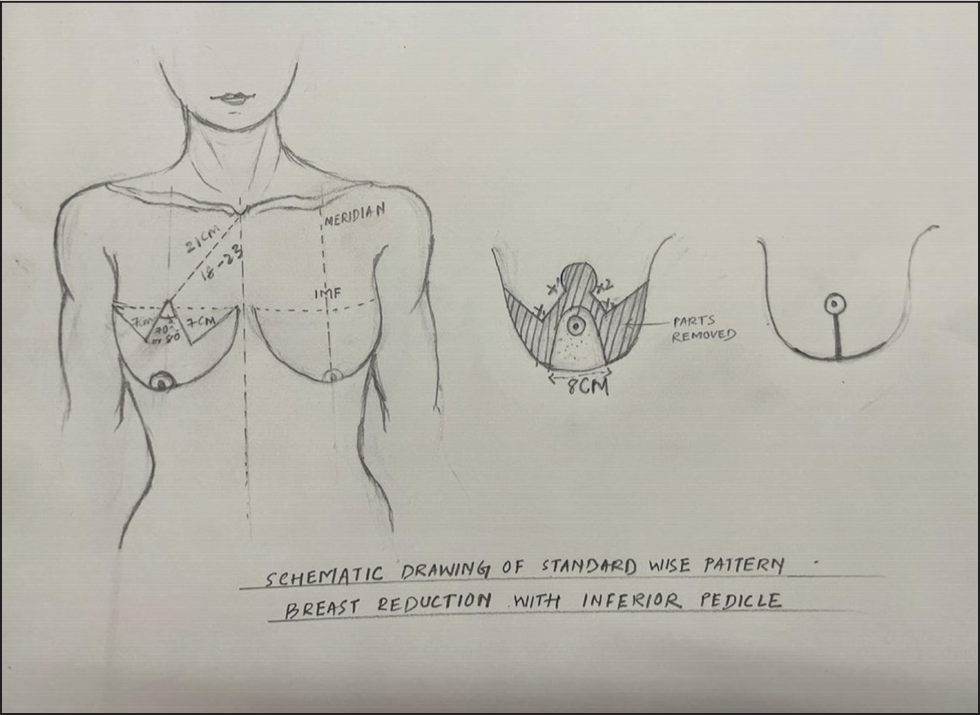
The surgical procedure was performed under general anaesthesia. Preoperative planning involved 4 as shown in (Figure 2) Wise-pattern markings to guide skin excision and ensure symmetrical reduction. The inferior pedicle was designed with an 8–10 cm base to maintain blood supply to the NAC as described in (Figure 1).
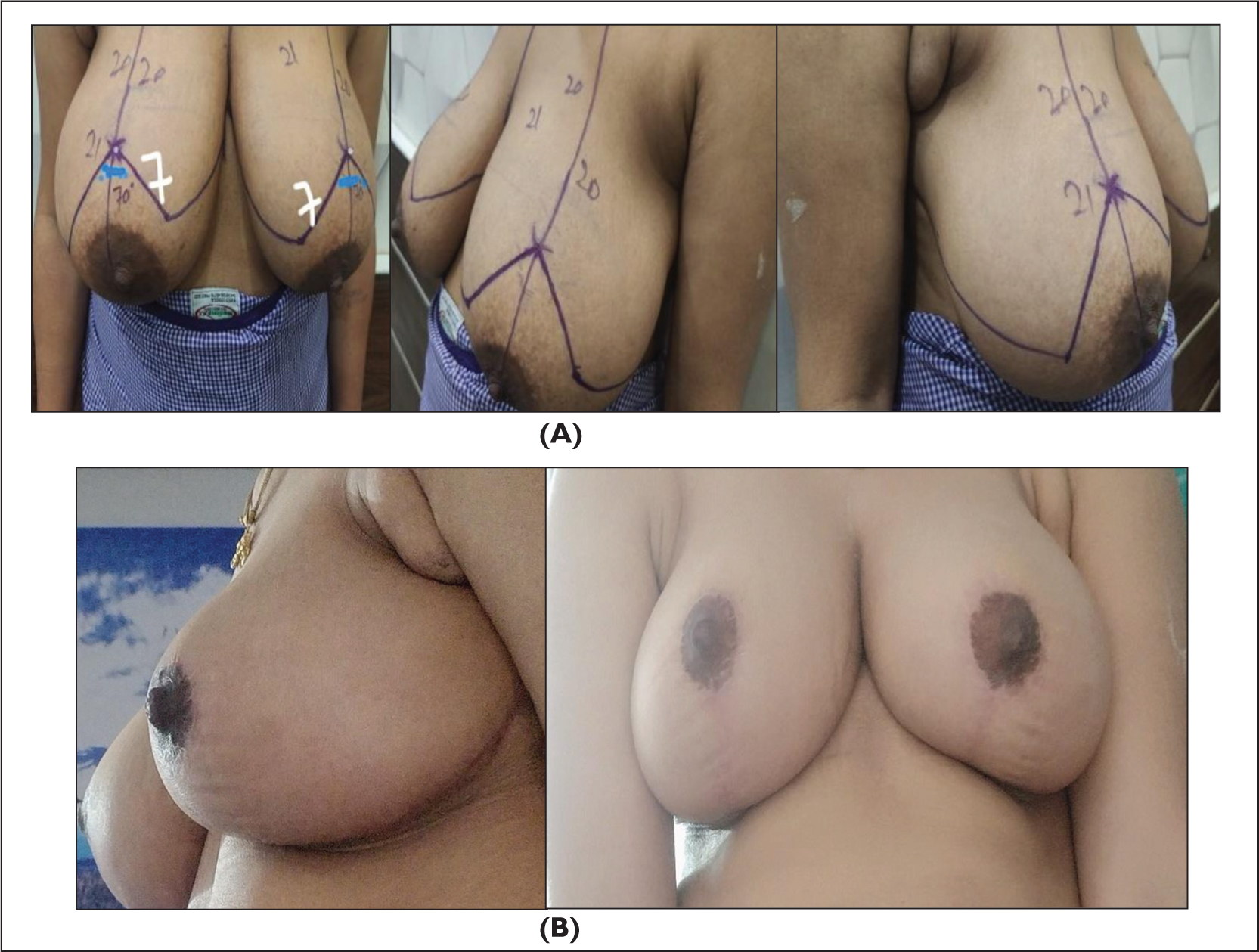
Planning and Preoperative Markings
As shown in (Figure 2), in a Wise-pattern inferior pedicle reduction mammoplasty, 5 preoperative markings are a crucial step to ensure optimal results and symmetry. These markings are typically helpful and guide in creating the desired shape while minimising complications. 6 The following outlines the typical preoperative markings for this type of procedure as summerised in (Figures 1 and 2):
Midline marking:
Draw a vertical line down the centre of the chest, aligning it with the sternum.
NAC location:
Mark the desired position of the NAC, generally positioned about 4–5 cm below the inframammary fold (IMF) or higher, depending on the patient’s anatomy. Mark the NAC’s location, which is usually the central point for the reduction.
IMF:
Mark the IMF (this is the fold beneath the breast). This marking is crucial, as it helps determine the lower boundary of the breast and guides the incision pattern.
Horizontal/transverse marking:
A horizontal line is marked along the IMF to outline the extent of the reduction and the positioning of the breast mound.
Verticalline from NAC:
Draw a vertical line from the NAC down to the IMF to guide the vertical portion of the Wise pattern.
Circle or keyhole shape:
Outline the Wise pattern around the breast using an inverted-‘T’ or anchor shape. The outline includes a horizontal line along the IMF and a vertical line extending from the NAC towards the fold. The skin above the horizontal line is the area to be removed, while the remaining skin forms the new breast shape.
Marking of the pedicle:
The ‘inferior pedicle’ refers to the remaining tissue that will sustain the NAC. Mark the tissue to be retained as the pedicle to maintain blood supply to the NAC. Ensure adequate tissue is left to avoid necrosis of the NAC. The pedicle should be wide enough to preserve blood flow, but narrow enough to allow for proper shaping.
Excess tissue:
Mark the areas where excess tissue will be removed. This is determined by visualising how much volume needs to be reduced, based on the patient’s goals.
Symmetry and aesthetic considerations:
Double-check the markings for symmetry, ensuring both breasts are even in shape and size. Consider the patient’s preferences in terms of breast size and shape when placing the markings.
These markings are intended to guide the incisions and tissue removal, while maintaining aesthetic results and nipple viability. 6
Key steps include as shown in (Figure 3):
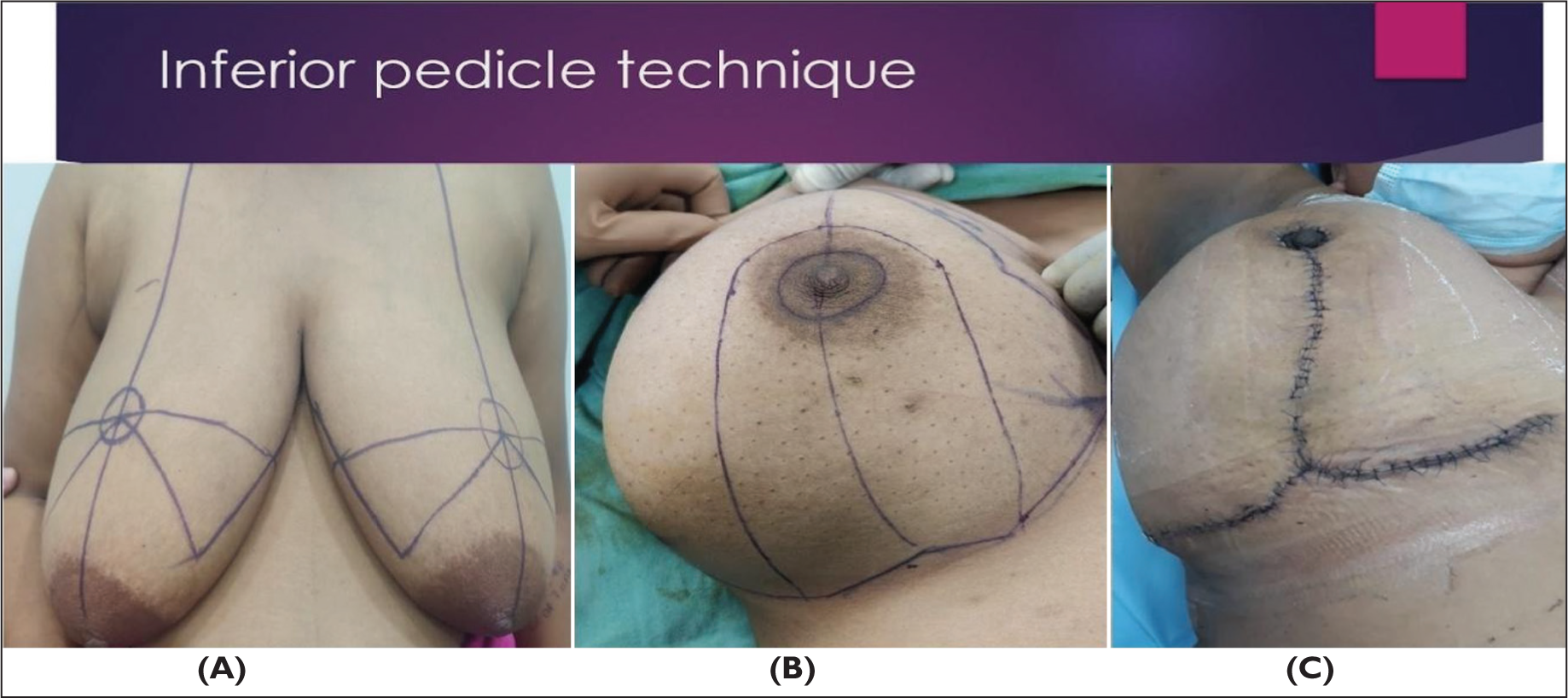

Skin incision following the Wise pattern
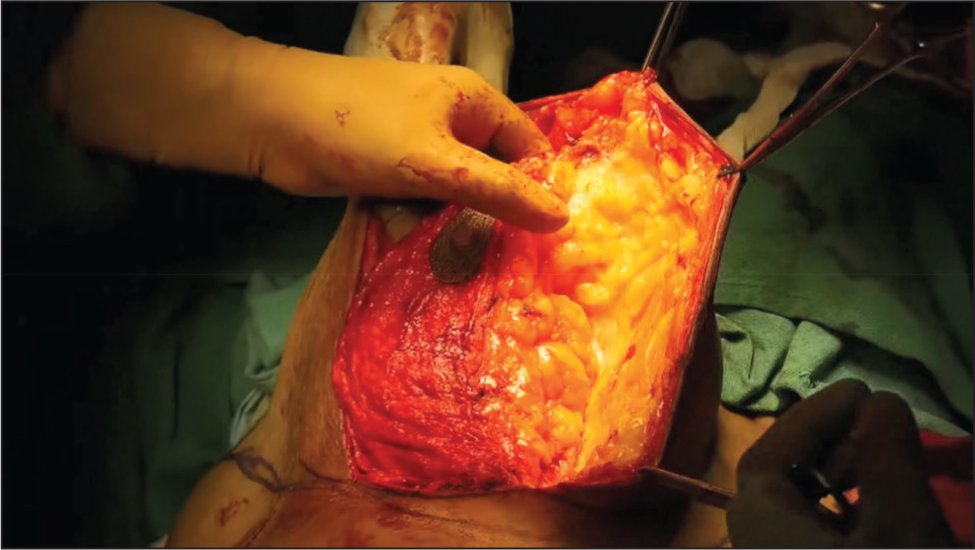
Creation of an inferiorly based pedicle to preserve NAC vascularity
Resection of excess glandular tissue while maintaining structural integrity
Repositioning of the NAC to an anatomically appropriate location
Inverted-T closure for optimal contouring as mentioned in (Figure 4)
Postoperatively, patients were monitored for wound healing, NAC viability and overall breast aesthetics. Compression garments were prescribed to support healing, and follow-up assessments were conducted at 1, 3, 6 and 12 months.
Results
Postoperative outcomes demonstrated significant symptomatic relief and high patient satisfaction. Notable findings included:
Sustained NAC sensation, breast projection and aesthetic shape Average reduction per breast: 600 g to 1.2 kg Complication rates: Bottoming-out (three patients), high NAC positioning (one patient) and partial NAC necrosis (one patient) No instances of total NAC loss or severe asymmetry Patient satisfaction scores reflected improvements in nipple sensation, reduced shoulder/neck pain, ease in clothing selection and reduced social embarrassment. Reduction Mammoplasty in Gigantomastia Using the Inferior Pedicle and Inverted-T Skin Closure as summerised in (Figures 5 and 6).

Discussion
Historically, breast reduction involved simple excision methods with high risks of NAC necrosis. Over time, techniques evolved to include superior, medial and lateral pedicle methods, each with distinct advantages and limitations. The inferior pedicle approach emerged as a preferred technique due to its robust vascular supply and its ability to maintain NAC sensation and function.
The principles guiding successful breast reduction include:
Maintaining appropriate NAC position Achieving a hemispherical, symmetrical breast shape Minimising scarring while preserving skin elasticity
One of the key advantages 7 of the inferior pedicle approach is that it maintains the blood flow to the NAC. This reduces the risk of complications such nipple necrosis, which can sometimes occur when other techniques are used, particularly those that involve detaching the nipple completely. The inferior pedicle technique provides excellent aesthetic outcomes by maintaining the natural shape of the breast. 8 The breast tissue is reshaped in a way that creates a youthful and natural appearance as shown in (Figure 7), with the nipple being placed in a higher, more youthful position. This technique can be used for a wide range of breast sizes and shapes, making it suitable for many different patients. It works well for women with significantly oversized breasts and those looking for both volume reduction and lift. Since the technique involves moving the NAC as a unit, the risk of asymmetry between the breasts is minimised, leading to a more balanced outcome. Because the nipple is preserved with its pedicle, there is a lower risk of permanent changes in nipple sensation, a common concern in breast reduction surgery. Glandular tissue is also preserved to maintain the potential for future lactation. There are some considerations and potential risks. For example, while the inferior pedicle technique offers great aesthetic benefits, 9 the procedure typically leaves visible scarring. The incision is often placed around the areola and extends down ••to the IMF (beneath the breast). The scars usually fade over time, but they may not disappear entirely. Another risk 10 is that the recovery process for this type of breast reduction may take longer compared to other techniques. Patients may experience swelling, bruising and discomfort in the first few weeks. Wearing a supportive bra and following postoperative instructions can help minimise these effects. As with any surgical procedure, there are inherent risks, including infection, poor wound healing, haematoma or changes in nipple sensation. However, when performed by an experienced and skilled surgeon, these risks can be minimised. While the inferior pedicle technique preserves the NAC, it can sometimes affect the ability to breastfeed in the future. Patients should discuss this concern with their surgeon before undergoing surgery, particularly if they plan to breastfeed after the procedure. While the results of breast reduction surgery can be long-lasting, factors like ageing, weight changes and pregnancy may alter the shape and size of the breasts over time. It is important for patients to maintain a stable weight and consider the long-term implications of these factors.
Although the inferior pedicle technique is associated with fewer complications, some issues still can arise, including:
Bottoming-out as shown in (Figure 8): Observed in three patients, managed with secondary corrections. High NAC positioning: Reported in one patient, improved with minor revisions. Partial NAC necrosis: Occurred in one patient, requiring conservative wound care.
Late complications, 10 such as scarring, nipple malposition and asymmetry, were found to be more dependent on surgical technique than on vascularity.
Conclusion
Inferior pedicle reduction mammoplasty remains the gold standard for treating gigantomastia, providing a balance between functional relief and aesthetic outcomes. The technique ensures robust NAC viability, preserves sensation and achieves long-term patient satisfaction. 9 Proper surgical planning, meticulous execution and careful postoperative monitoring are crucial for minimising complications and optimising results.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.