
Abstract
Aim and Objectives:
The primary aim of this article is to evaluate the feasibility and safety of performing gynaecomastia surgery in a stand-alone day-case clinic. We examined existing gynaecomastia classification systems, comparing them with a novel component-based approach, and assessing outcomes in patients, including those presenting with anabolic androgenic steroid (AAS)-induced gynaecomastia.
Introduction:
The coronavirus disease 2019 (COVID-19) pandemic significantly reduced elective procedures in corporate hospitals, prompting many patients to seek treatment in alternative settings. As interests in aesthetic surgery procedures increased during this time, stand-alone clinics emerged as having the potential for day-case gynaecomastia correction.
Methods:
A retrospective review was conducted in a single stand-alone aesthetic clinic, focusing on 74 patients who underwent gynaecomastia surgery between March 2014 and January 2025. Patients were treated based on an adapted component-based classification system that addresses skin redundancy, fat volume, gland prominence and nipple projection. Surgical techniques comprised tailored combinations of gland excision, nipple reduction, skin reduction and where necessary, liposuction. Data was collected on complication rates, patient satisfaction and cost comparisons.
Results:
Among patients treated, findings demonstrated low complication rates and high satisfaction scores. Individuals with AAS-induced gynaecomastia require more meticulous operative planning and follow-up. Costs were generally lower compared to corporate hospitals.
Conclusion:
Day-case gynaecomastia surgery in a stand-alone clinic is both feasible and safe when underpinned by rigorous preoperative protocols, precise patient selection and refined surgical techniques. The use of a tailored classification system enhances surgical planning and outcomes, especially in challenging presentations such as AAS-induced gynaecomastia. This approach highlights the potential for ‘stand-alone’ aesthetic centres to deliver high quality, patient-centred care without compromising safety or efficacy.
Keywords
Introduction
Gynaecomastia is the enlargement of male breast tissue and encompasses a spectrum of presentations. Physiological gynaecomastia is common in newborns and adolescents due to an imbalance between oestrogen and testosterone.1,2 In men above the age of 50, decreasing testosterone levels can result in growth of breast tissue. Nonphysiological gynaecomastia can be caused by medical conditions, medications and use of substances such as anabolic androgenic steroid (AAS). This can cause a great deal of anxiety, pain and discomfort for individuals. Although adolescent gynaecomastia may resolve spontaneously, it can persist in a small number of cases. The term pseudogynaecomastia is used when only fat is the cause of an enlarged male breast.1,2 Treating the underlying cause or stopping the causative medications may lead to improvement. Medical treatment options include tamoxifen, but this may only cause a partial reduction in breast tissue.3,4 Many patients choose to undergo surgical intervention, especially when there is persistent and painful glandular tissue, significant aesthetic deformity or psychosocial distress. 5 Minimally invasive techniques are favoured due to less risk of complications, faster recovery times and reduced scarring.
The coronavirus disease 2019 (COVID-19) pandemic disrupted elective surgical services globally, with many private hospitals prioritising urgent cases and cancelling elective aesthetic procedures such as gynaecomastia correction. Studies have shown that interest in plastic surgery procedures increased during this time. 6 Travel restrictions and cost considerations may have deterred patients from seeking procedures abroad. In the United Kingdom, the furlough scheme also provided some individuals with the financial means and ability to save money. Whilst under lockdown measures they had the time to explore elective surgeries locally. As a result of this, the pandemic gave stand-alone aesthetic day-case centres a unique opportunity to address the gap by offering day-case gynaecomastia procedures. The implementation of rigorous safety measures and comprehensive perioperative protocols has allowed such surgeries to be undertaken in these settings.
Methods
The authors collected the data at the stand-alone day-case aesthetic surgery centre in the United Kingdom. Since the COVID-19 pandemic, between July 2020 and January 2025 a total of 56 patients underwent gynaecomastia surgery at the clinic. Pre-pandemic, a total of 18 patients were also treated. The age of the patients ranged from 21 to 47 and the mean age was 33.
Component-based Classification of Gynaecomastia
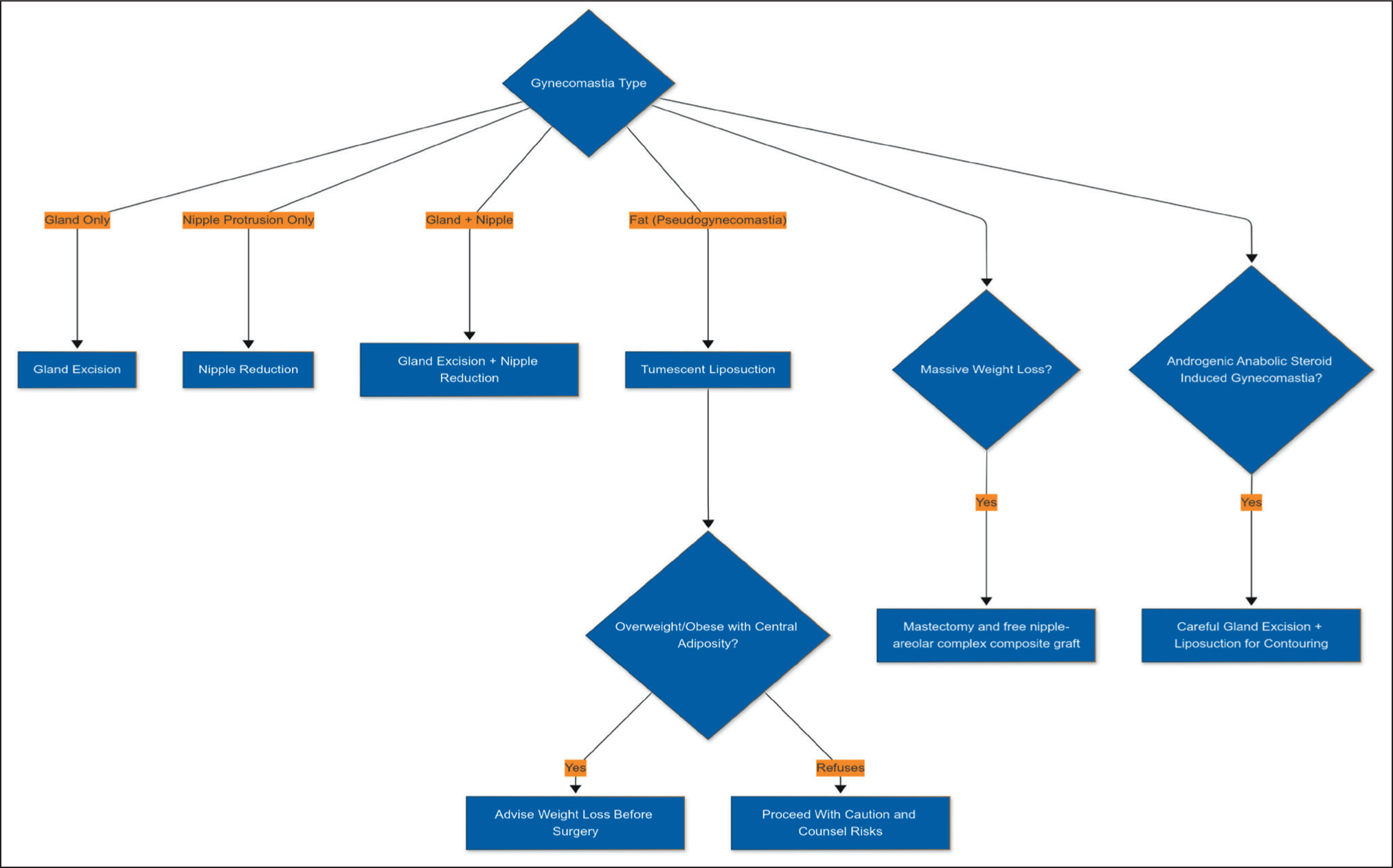
We propose a component-based classification strategy that evaluates the key anatomical elements: skin, fat, gland, nipple, generalised obesity and the position of nipple areolar complex (NAC) (Figure 1). This approach considers the extent of skin laxity (including patients presenting post massive weight loss), any associated fat, the volume and prominence of glandular tissue (including those who have used AAS) and nipple projection. By categorising patients according to the specific components requiring correction, this algorithm (shown in Figure 1) enables precise surgical planning. For example, patients with predominantly glandular tissue and minimal excess fat undergo excisional surgery, with or without minor liposuction for contouring. Conversely, those with significant adiposity but mild glandular development primarily receive liposuction, with a small incision for gland resection if necessary.
Component-based Classification Algorithm for Gynaecomastia Which Can Be Applied to Tailor the Treatment and Achieve the Desired Result in a Stand-alone Clinic.
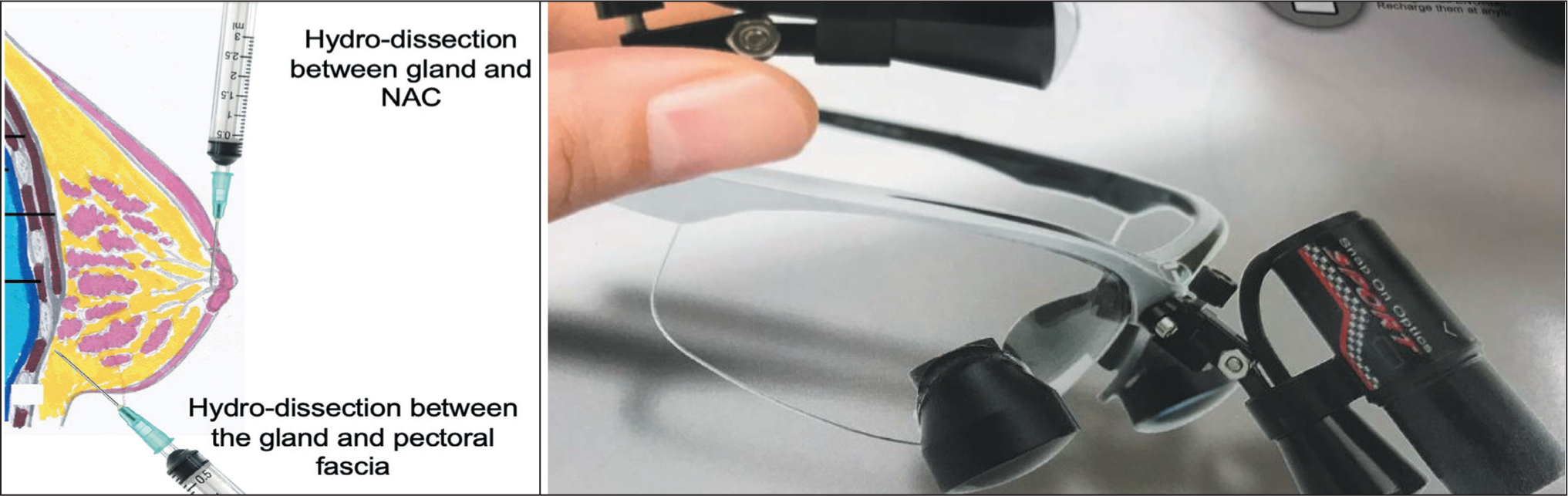
Method of Hydrodissection and Example of Surgical Magnifying Loupes Which Aids in Excision of the Gland in Gynaecomastia Surgery.
Existing classification systems provide a straightforward framework for diagnosis, but the component-based approach introduced here takes a more nuanced view by offering a tailored plan for addressing each patient’s specific anatomical issues. This extends beyond simple assessments of breast size and skin redundancy, especially in cases where nipple repositioning or selective tissue excision is required. This ensures that gynaecomastia surgery is adapted to each individual’s unique proportions with their concerns and expectations addressed during early consultations.
Preoperative weight loss is important in overweight or obese patients who can be prone to a mismatch in proportions between the chest and abdomen. This reduces the risk of a postoperative disproportionate body shape and highlights why en bloc removal of gynaecomastia tissue is often inappropriate. Instead, the focus should be on the specific components requiring sculpturing and judicious use of liposuction for feathering rather than for volume reduction.
Safety Measures and Anaesthetic Protocols
During the pandemic, restrictions at larger hospitals necessitated the development of innovative approaches for elective procedures. The stand-alone day-case clinic developed a protocol driven service, starting with a comprehensive pre-anaesthetic assessment. Each patient’s medical history, comorbidities and body mass index (BMI) are carefully evaluated to determine suitability for day-case surgery. A sexual hormone assay and liver function tests are requested when indicated, especially in patients with suspected AAS use.
Only patients who are designated ASA categories 1 or 2, indicating that they have either no systemic illness or mild systemic disease, are deemed eligible for day-case surgery. Those with ASA 3 or higher, significant obesity or co-morbidities would be directed to hospital-based facilities. To bolster patient safety, the clinic negotiates service level agreements with nearby NHS and corporate hospitals. This means that urgent transfers can be arranged if complications such as severe haemorrhage or anaesthetic emergencies, exceeding the clinic’s capacity for intervention, were to arise.
In view of performing correction of gynaecomastia, which is a non-essential procedure, all patients are monitored with pulse oximetry using the monitoring equipment for general anaesthetic even if using only local anaesthetic. All the patients will have intravenous access for emergency use. General anaesthetic or sedation is only used when a patient cannot tolerate tumescent liposuction using local anaesthetic. This may be the case in AAS-induced gynaecomastia where patients often have fibrous breast tissue adherent to the pectoral fascia. The dose of local anaesthetic and adrenaline used for tumescent liposuction is calculated based on weight and appropriately diluted in normal saline depending upon the size and extent of the gland. A clinical trial by Klein and Jeske showed the maximum safe dose of tumescent lidocaine with adrenaline without liposuction is 28 mg/kg and with liposuction is 45 mg/kg. 7
Holt stresses the importance of having lipid emulsion available to treat any toxicity because high doses are often used and the amount of absorption in each individual can vary. 8 Bupivacaine is also used for tumescent liposuction. Paik et al. surveyed US plastic surgeons who reported using bupivacaine in doses ranging from 62.5 mg to 150 mg. 9 Some smaller studies have shown that it may offer faster recovery times and improved pain control. 10 Mohan et al. describe use of tumescent anaesthetic as an effective method for liposuction without the use of general anaesthetic which is ideal for a stand-alone day-case centre. They also used tranexamic acid which greatly reduced the chance of bleeding. 11
Once the antiseptic solution is applied on the proposed site only one side is infiltrated and then the nursing staff complete painting, draping and isolation of the anterior chest wall. This allows the local anaesthetic to act for approximately 8 minutes-10 minutes. Before closure of the first incision, the opposite side is infiltrated in order to give adequate time for the local anaesthetic to take effect. This sequence makes the procedure time efficient, minimises blood loss and reduces risk of anaesthetic toxicity.
A resuscitation kit including a defibrillator and lipid emulsion antidote for local anaesthetic toxicity is always available. Following the National Institute of Clinical Excellence (NICE) guidelines for perioperative care 12 and presence of a consultant anaesthetist during all procedures ensures patient safety at all times.
Surgical Technique
Incisions and Gland Excision
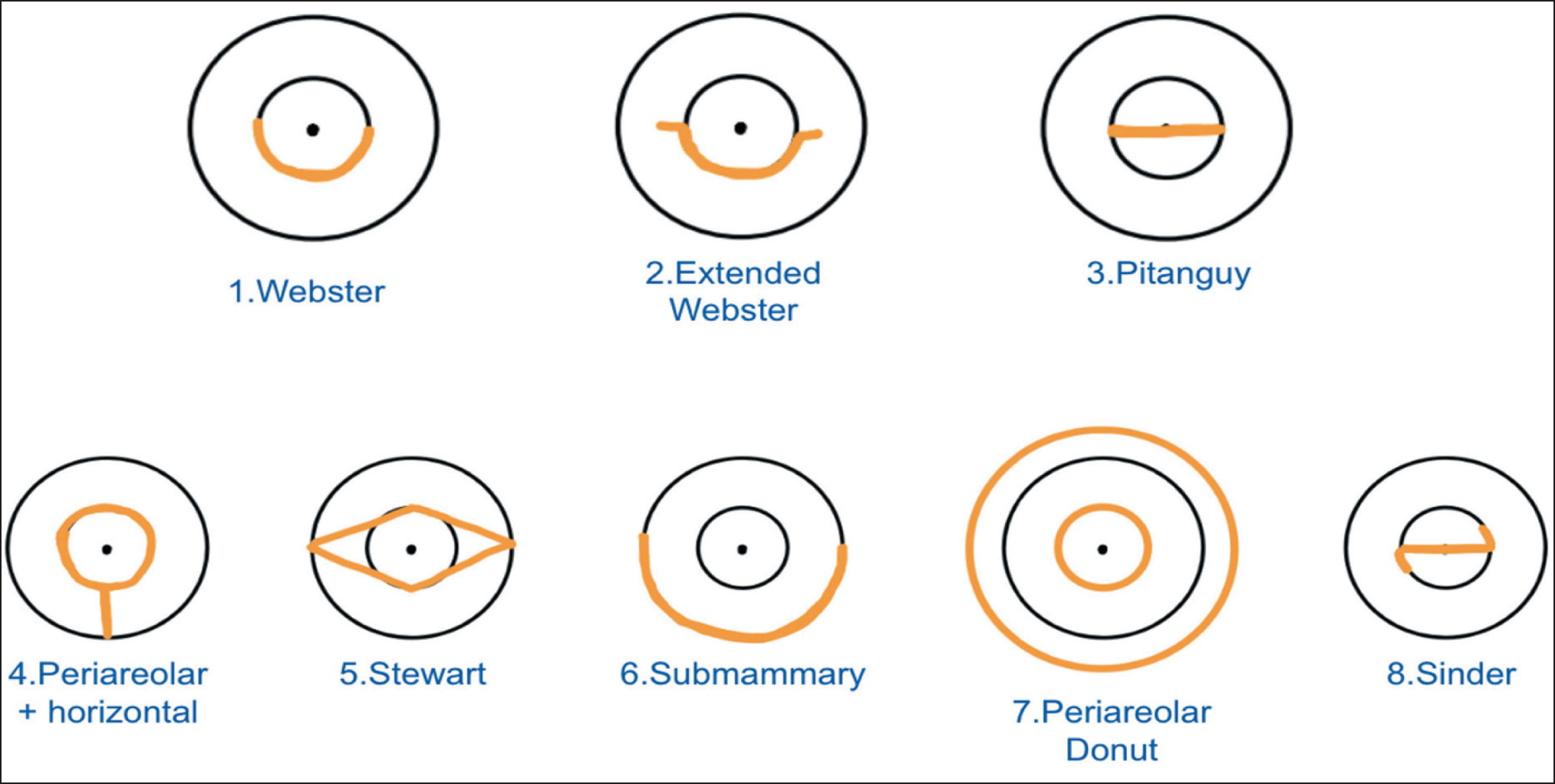
Figure 3 summarises the different incisions described in the literature for gynaecomastia surgery. 13 For straightforward cases requiring direct gland excision without nipple reduction, the Webster incision offers adequate access whilst minimising visible scarring. 14 An extended Webster incision can be used if the gland is particularly large and widespread to allow better access. The senior author favours the Pitanguy’s incision if nipple reduction along with gland excision is required as it allows for direct access to the gland (Figures 4 and 9). 15 Although an axillary approach has been cited in the literature, it is less commonly utilised in this clinic and would require further evaluation for efficacy and feasibility. 16 Mastectomy and free NAC graft are used mostly in patients who are undergoing gynaecomastia surgery post massive weight loss. In these cases, assistance from an additional surgeon in the theatre is essential to reduce theatre and general anaesthetic time particularly in a stand-alone day-case centre (Figure 11).
Adapted from Verbicário et al. 13 Incisions That Can Be Used for Gynaecomastia Correction Surgery. The Senior Author Prefers to Use Incisions 1-3 (Top Row) Rather Than Incisions 4-8 (Bottom Row).
During excision, hydrodissection is extremely valuable in delineating the gland from the underlying pectoral fascia and the NAC (Figure 2). Use of surgical magnifying loupes with a headlight allows the precise identification and removal of fibroglandular tissue whilst preserving a thin layer of subcutaneous fat to prevent saucer-shaped deformities (Figure 2). The use of liposuction is then only needed to create an aesthetically pleasing result mainly for feathering the edges following gland excision. As mentioned above, the senior author believes that liposuction should not be used for volume reduction as it can cause upper/lower trunk disproportion if it is used in obese patients without optimising BMI beforehand.
An Example of the Use of Horizontal Pitanguy’s Incision for Excision of Bilateral Gynaecomastia Plus Nipple Reduction in Two Patients with the Excised Gland and Nipple Shown in Figure 4b.
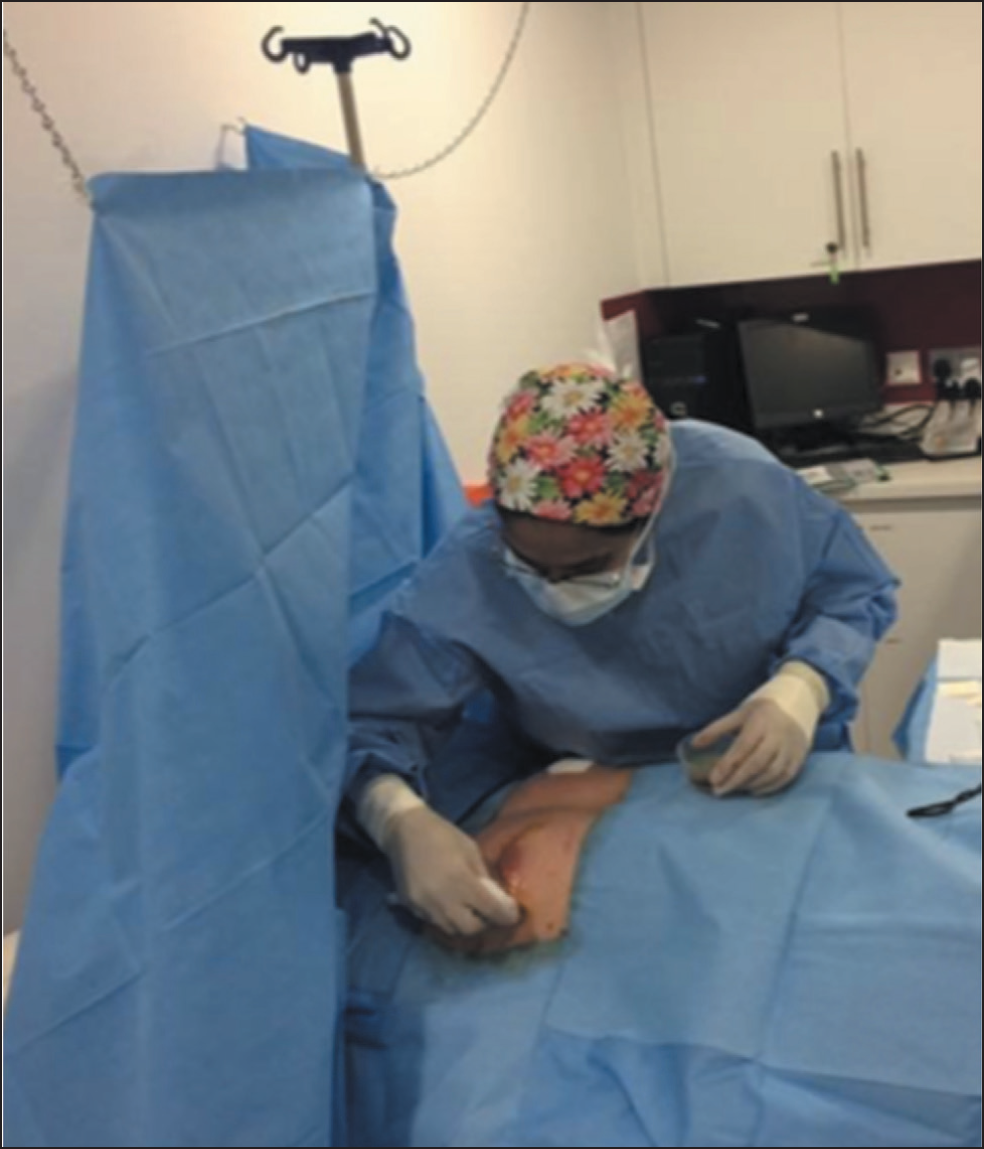
Use of a Ceiling Mounted Sterile Curtain Ensures Patient Comfort. Chains from the Ceiling Are Used Rather Than an Intravenous (IV) Fluid Stand to Utilise Theatre Space More Effectively.
Liposuction
During initial consultations, assessment and physical examination should not focus solely on the chest wall but the entire body. Noting the deposition of fat in the abdomen is important to avoid the possibility of creating a ‘pear shaped’ deformity following the procedure. In such cases, the patient may benefit from weight loss prior to the surgery (Figure 10).
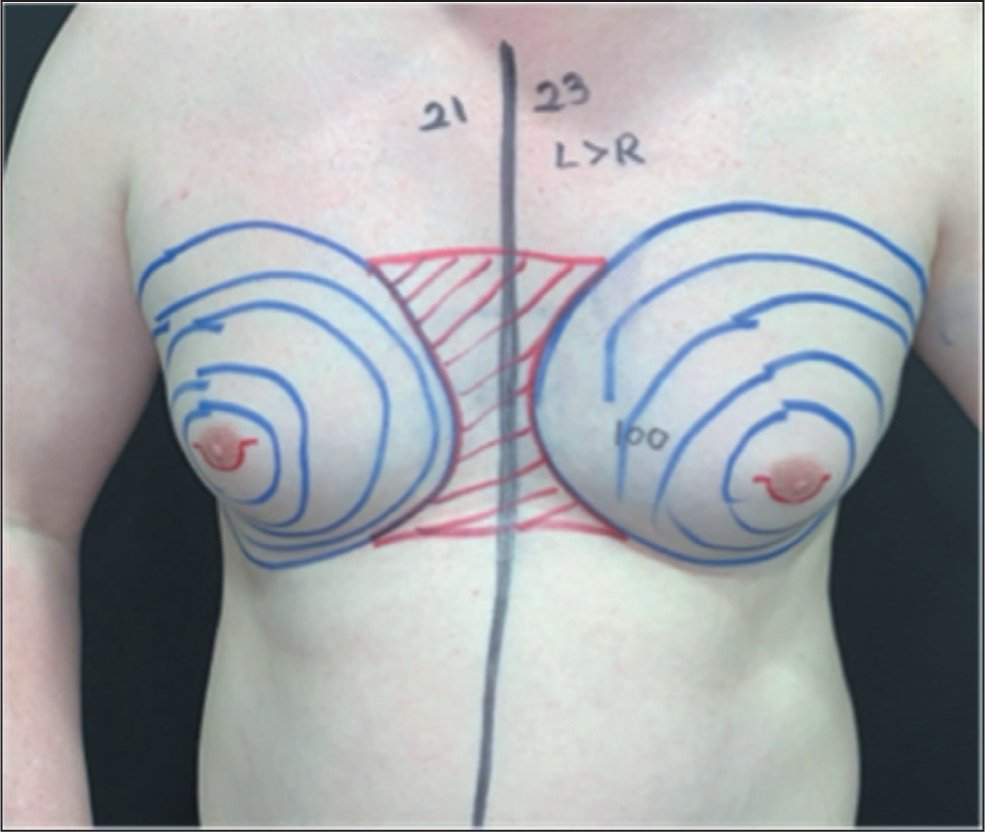
Liposuction serves primarily as a finishing step to feather the edges and ensure a smooth chest contour. Using local anaesthetic and tumescent liposuction, the surgeon can carefully sculpt fat deposits (Figure 6). It is important to note, however, that gland removal remains the primary objective in most cases. This marks a move away from the techniques first proposed by Courtiss in 1987 where liposuction was the primary method of treatment. 17 The senior author ensures a thorough and uniform removal of fat by inserting the liposuction cannula through both the ipsilateral and contralateral periareolar incisions using a cross-chest technique, allowing access to the treated region from multiple angles. Figure 2 shows the pre surgical markings for liposuction used by the senior author. The technique avoids the need to make a further incision for liposuction and subsequent additional scars, a benefit which has been evaluated by Singamsetty et al. 18
A ceiling mounted sterile curtain separating the patient’s chest and head is particularly beneficial for procedures performed under local anaesthetic (Figure 5). This setup is space efficient and also enhances patient comfort and convenience.
Nipple Reduction
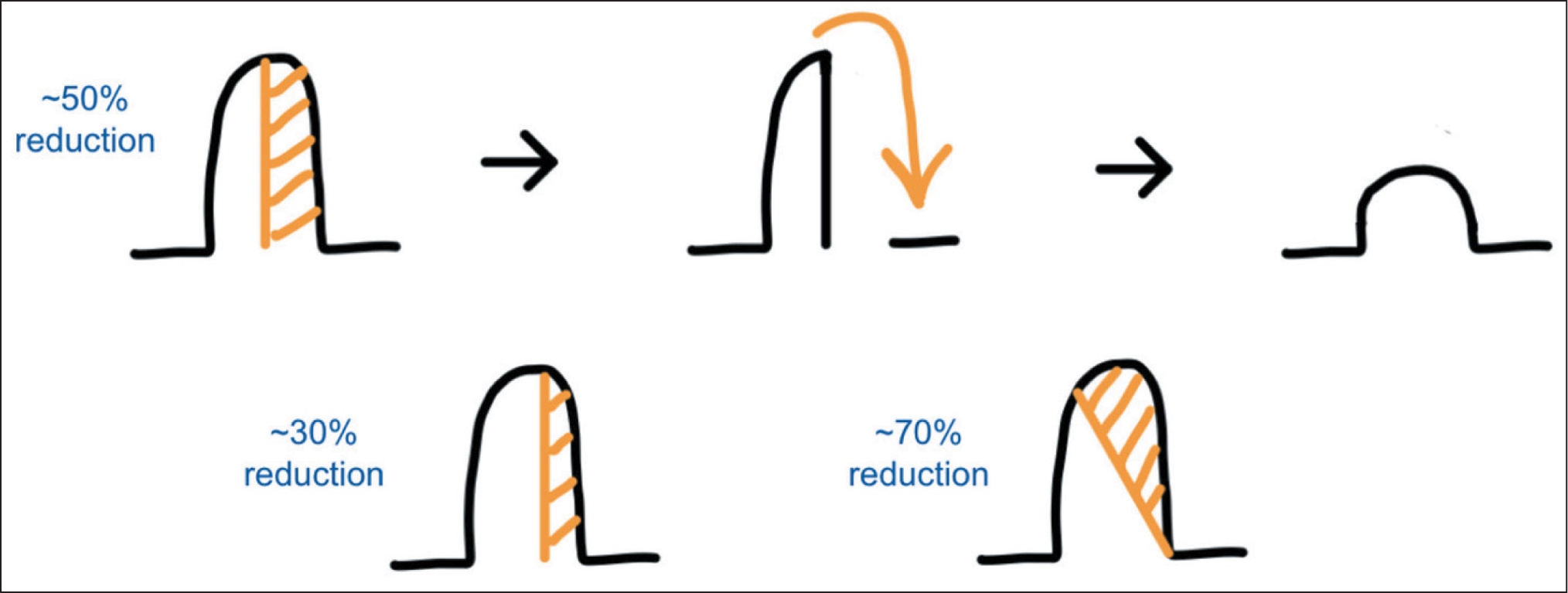
Nipple reduction is offered to patients whose nipples are over projecting or elongated. This can cause social anxiety, sensitisation due to friction against fabric and restrict the selection of clothing patients can wear. A vertical split excision is used as shown in Figure 7. The design of the excision and flap is modified according to the nipple reduction requirement. This versatile and flexible approach allows for the best outcomes in accordance with the patient’s wishes (Figure 8).
Presurgical Skin Markings for Liposuction Using Cross-chest Technique to Ensure a Uniform Result. Also Note the Markings for an Extended Webster Incision Used for This Patient Who Requires a Large Gland Excision.
Simple Representation of Nipple Reduction Using a Vertical Excision. The Position of the Excision Can Be Tailored to the Amount of Reduction Required.
Before and After Images of a Patient Who Underwent Nipple Reduction Procedure. The Underlying Gynaecomastia Was Not the Primary Concern to the Patient and Therefore Only Nipple Reduction Was Performed. This Highlights the Importance of Using a Patient-centred Approach.

Postoperative Care
At the end of each procedure, layered absorbable sutures (3–0, 4–0 and 6–0 Monocryl) are placed to achieve a neat closure. Patients are instructed to wear a compression vest for four to six weeks to support the newly contoured chest and reduce the risk of seroma and haematoma formation. A follow-up visit occurs at one week for wound review and dressing changes, followed by a more comprehensive evaluation at two to three months to document healing, final contour and patient satisfaction. Patients are strongly advised against vigorous physical activity or weightlifting during the early postoperative period to prevent wound dehiscence and subsequent haematoma formation.
Results
The treatment received by the 74 patients is summarised in Table 1. Local anaesthetic was used for 64 patients, 3 of whom had to be sedated during the procedure and 2 of these patients had AAS-induced gynaecomastia. General anaesthetic was used for 10 patients including 2 who started with local infiltration but needed to be converted to general anaesthetic due to intolerance of pain.
Results of Gynaecomastia Correction Surgery Performed on 74 Patients Between March 2014 and January 2025.
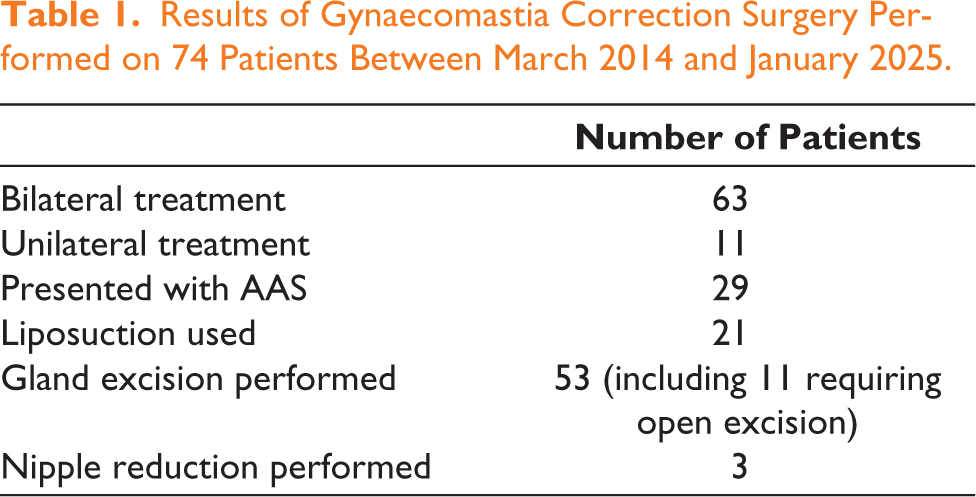
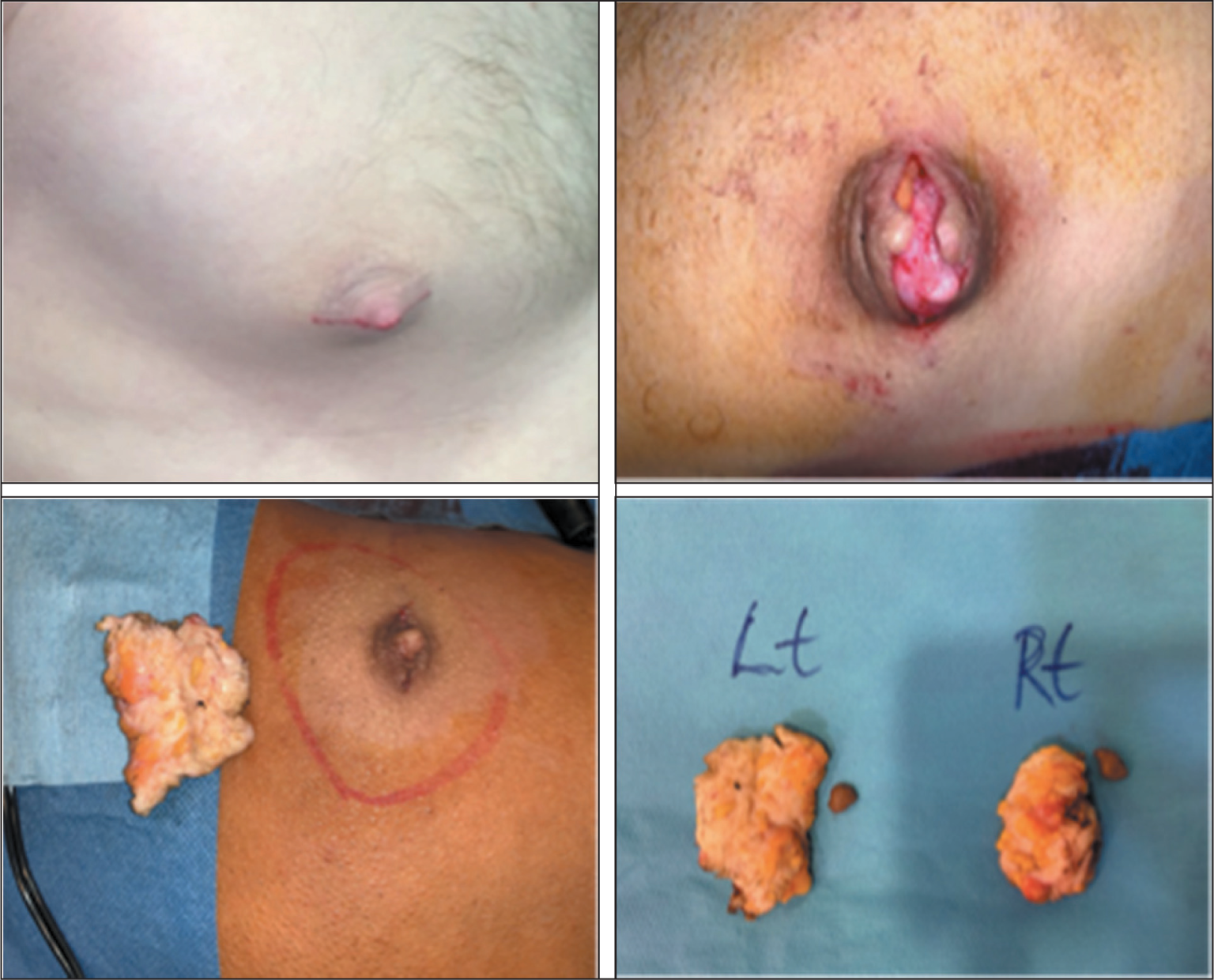
Patients achieved successful outcomes with only four patients experiencing complications. One patient had a haematoma and required transfer to a local hospital for evacuation under general anaesthetic. This was a patient with AAS-induced gynaecomastia who continued to use AAS and began exercising after the procedure. Those with AAS-induced gynaecomastia often have dense fibroglandular tissue and dilated blood vessels proportionate to their pectoral muscle mass, posing a slightly higher risk of early postoperative complications, especially if they resume intense training prematurely (Figure 12). There were three cases of epithelial loss into the lower part of the NAC whilst using the Webster approach. This is a complication which may happen due to compromised blood supply of the NAC following gland excision just underneath the NAC. This required monitoring of the patient and dressing changes for an extended time of up to four to six weeks.
This Patient Underwent Both Excision of Bilateral Gynaecomastia and Nipple Reduction Using Local Anaesthetic.
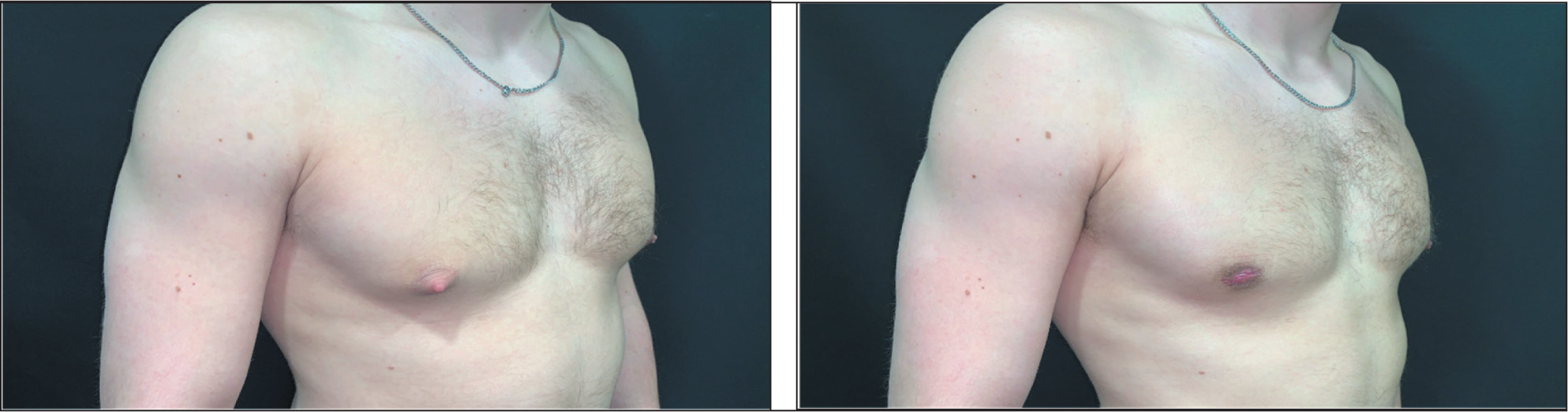
This Patient Was Encouraged to Lose Weight Before Surgery to Avoid a ‘Pear-shaped’ Body Disproportion. In the Left Image the Patient Was 103.7 kg, in the Centre Image the Patient Was 88.1 kg. The Right Image Shows the Patient Post-surgery Weighing 82.09 kg, Following Liposuction-assisted Open Excision Using Periareolar Approach.
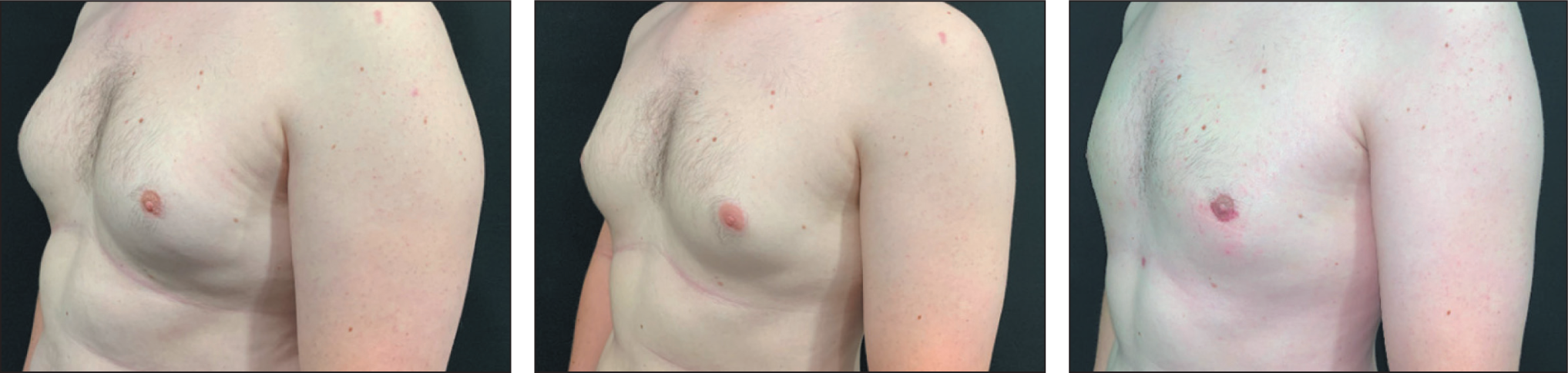
A Patient Who Underwent Mastectomy and Free NAC Composite Graft Following Massive Weight Loss Under General Anaesthetic. The Image on the Right Was Taken Four Months Post-surgery. In a Stand-alone Day-case Centre This Is Only Done with the Assistance of a Second Surgeon to Save Theatre and General Anaesthetic Time.

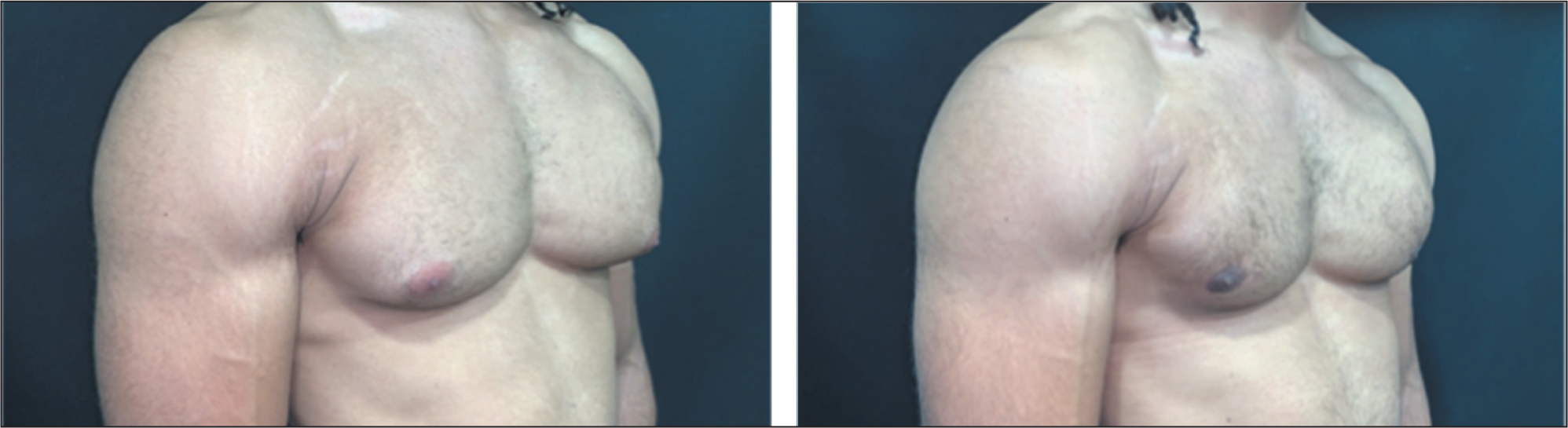
A Patient Presenting with Androgenic Anabolic Steroid-induced Gynaecomastia Before and After Surgery. The Procedure Was Performed Under Local Anaesthetic.
All patients were discharged the same day, which align with the stand-alone clinic’s day case strategy. There were no cases of anaesthetic toxicity. Patient satisfaction appeared high, likely due to reduced costs, shorter wait times and a more personalised treatment experience compared to larger hospital environments.
The figures below highlight patient cases where the component-based classification system has been applied.
Discussion
Classification of Gynaecomastia
It is important to adopt a flexible classification system that recognises the variable contributions of fat (including obesity), glandular tissue, skin tone/excess, nipple projection, level/position of NAC and AAS-induced gynaecomastia. Traditional classification methods often categorise gynaecomastia by overall breast size and ptosis. Whilst useful, these may not fully capture which specific elements require correction. By tailoring the procedure to the patient’s anatomy, surgeons can achieve more precise results, avoid overtreatment of unaffected areas and reduce the likelihood of contour irregularities. Our proposed classification system allows the surgeon to think about which treatment is most suited for the patient, right from the time of assessment until execution of the surgery. It can be used in conjunction with the other classification systems to both diagnose and plan management for gynaecomastia.
Existing classification systems for gynaecomastia include the widely recognised Simon classification, which designates four grades based on the extent of breast enlargement and the presence of excess skin. Grade I involves minor enlargement without excess skin, grade IIa indicates moderate enlargement with no additional skin, grade IIb indicates moderate enlargement plus redundant skin and grade III is characterised by marked enlargement and significant skin excess.19,20
Rohrich et al. classified gynaecomastia based on the degree of hypertrophy, ptosis and whether the tissue is primarily glandular or fibrous. 21 Grade I denotes minimal hypertrophy with no ptosis, grade II indicates moderate hypertrophy without ptosis, grade III involves severe hypertrophy with grade I ptosis and grade IV features severe hypertrophy with grade II or III ptosis. It has been argued, however, that ptosis is seen in cases with a lesser degree of hypertrophy which according to the Rohrich classification is present only in grades III and IV.
More recently Punia and Gupta 22 introduced a system that incorporates the presentation of puffy nipples and presence of fat rolls in the inframammary and axillary regions; a feature which is crucial to address with liposuction to create a uniform chest contour. This classification also provides estimates of the fat volume to be removed, suggests treatment plans and whether the procedure should be performed using local or general anaesthetic. Klinger et al. 23 created a classification system which utilised ultrasound to diagnose the cause of gynaecomastia as being only the gland, only fat or both gland and fat. This was further categorised into patients who had ptosis and those who did not. This can then be used to plan treatment. This did not include those with nipple hypertrophy or AAS-induced gynaecomastia. Additionally, Innocenti et al. devised an algorithm based on patient body type and BMI. 24 Patients are categorised from those with an athletic physique and BMI<25 with only a small amount of glandular tissue to those who are overweight with more fat volume than glandular tissue. This classification also includes ptosis and size of the NAC along with treatment options for each type of gynaecomastia.
Other notable classification systems include those by Barros and Sampaio 25 , Ratnam 20 and Gusenoff et al. 26 These focus on tissue hypertrophy, ptosis severity, position of the NAC and the inframammary fold. A 2017 systematic review evaluated all gynaecomastia classification systems published in the literature at the time. 27 A total of 11 classification systems were found and each typically incorporated two to three of the features mentioned above as well as skin elasticity, absence of sternal notch, chest shape, breast tuberosity and upper abdominal laxity.
Our classification algorithm encompasses elements which enable the surgeon to make a patient centred decision regarding the best treatment. It includes patients with gynaecomastia due to gland hypertrophy, excess fat, ptosis, patients who have skin laxity due to massive weight loss, obesity requiring weight loss before surgery and AAS-induced gynaecomastia. Unlike other classifications, nipple protrusion has been included despite not technically falling under the definition of gynaecomastia. We believe that achieving the most favourable aesthetic outcome requires considering the nipple when correcting a chest wall deformity (Figure 1).
Consideration of Androgenic Anabolic Steroid-induced Gynaecomastia
Recently, an increasing subset of patients seeking correction at the clinic has gynaecomastia associated with AAS use. This is often very painful and tender to touch. The health effects of AAS are not just limited to gynaecomastia and have been well documented. These include sexual dysfunction, acne, cardiovascular conditions and even increased mortality rate. Hospital admission is also more common in these individuals. 28 Studies have also shown that AAS use can increase risk of social anxiety due to concerns over their appearance and body image. They may also experience symptoms of depression. 29 AAS-induced gynaecomastia can restrict patient’s day-to-day activities and affect the relationships with their families. AAS-induced gynaecomastia can resolve spontaneously upon stopping all use of AAS, but in some cases, it may not and therefore requires surgical management.
Patients typically present with denser and more fibrous glandular tissue which is adhered to the pectoral fascia to an extent that it is almost calcified with lateral extension into the chest wall. 30 In practice, we have observed that the gland takes on a horizontal oval-shaped appearance rather than round seen in other forms of gynaecomastia. Preoperative screening includes a hormonal profile and liver function tests, given the potential endocrine disturbances linked to AAS use. It is also important to address any underlying anxiety linked to body image that these patients have so that the expectations and outcomes of the treatment are clear. They are also instructed to stop all steroid use at least six weeks prior to the procedure.
The fibrous nature of AAS often requires a more careful hydrodissection to separate the gland from the fat, NAC and particularly the pectoral fascia in the lateral part of the chest wall. Intraoperative haemostasis is crucial to ensure complications do not arise.30,31 The procedure is primarily done using local anaesthetic, but the patients are fasted and ready with intravenous access, should sedation be required. Patient motivation to resume training often remains high; therefore, close follow-up is essential to ensure proper healing and to mitigate the risk of complications. Babigian and Silverman described that recurrence of gynaecomastia may occur in these patients as a small disc of glandular tissue may remain below the NAC following surgery which would then respond and proliferate if the patient was to resume use of AAS. 32 Strict postoperative instructions are crucial, emphasising the dangers of returning to heavy lifting too soon, which can lead to wound breakdown or haematoma formation which is the most common postoperative complication in AAS-induced gynaecomastia.
Choice of Incision
The senior author prefers to use a Webster periareolar incision when only gland excision is indicated. Extreme care must be taken to maintain a delicate balance between removing an optimum amount of gland whilst preserving the vascularity of the NAC when using this incision. If the NAC flap consists of residual gland, patients may experience dissatisfaction due to the palpability of the remaining gland beneath the NAC. Conversely, excessive gland removal can compromise the vascularity of the NAC, leading to partial necrosis of the lower part of the areola or epithelial loss, which may require extended postoperative monitoring.
A horizontal extension of the Webster approach (shown in Figure 3) is preferred if excision becomes difficult, and consent regarding this possibility is obtained for all patients. As mentioned above Pitanguy’s incision is useful when both gland excision and nipple reduction are indicated. The Sinder’s incision is avoided due to concerns about tip necrosis of the areolar flap. If skin reduction is required for gynaecomastia correction, particularly following massive weight loss, mastectomy with a free NAC composite graft is the preferred approach. This technique consistently provides a predictable and satisfactory outcome without the risk of stretching or hypertrophic scarring associated with periareolar donut, periareolar with horizontal, Stewart or submammary as shown in Figure 3. We have observed aesthetic disfigurement due to stretching or hypertrophic scarring, including an expanded areola, in patients who have undergone surgery with these techniques elsewhere, making them less favourable in senior author’s practice.
Stand-alone Clinic Advantages and Limitations
The day-case approach offered in a stand-alone clinic setting provides certain distinct benefits, including cost-effectiveness and continuity of care. Patients often report feeling more at ease than in large hospital wards due to the more confidential environment and less exposure to infectious diseases. Expenses in a stand-alone facility tend to be lower, allowing fee structures that can compete with popular medical tourism destinations. This allows patients to access treatment in a local setting, reducing the need to travel abroad. The use of magnifying loupes with a headlight mentioned before mitigates the need for ceiling mounted theatre lights in a clinic setting which can cost upwards of £10,000. 33
Stand-alone clinics must carefully assess patients to ensure they do not exceed the clinic’s capacity for managing complications. Advanced reconstructions, multiple concurrent procedures or patients with significant comorbidities may be better served in hospitals equipped with multi-specialty teams and extended postoperative care facilities. Future audits should focus on collecting additional evidence to validate the efficacy of day-case gynaecomastia surgery in these settings.
Conclusion
Gynaecomastia surgery in a stand-alone clinic can be safe, effective and patient-centred, provided there is a clear framework for patient selection, robust perioperative protocols and a readiness to manage potential complications. This is an artistic procedure which should be tailored to the individual circumstances of the patient. Our new classification allows the surgeon to develop and apply the insights in the form of various components during physical examination, planning and performing the procedure, to improve aesthetic outcomes and patient satisfaction. Whilst the COVID-19 pandemic served as a catalyst for the expansion of services in smaller clinics, the strategies outlined here remain valuable even as healthcare systems have returned to normal operations, representing an evolution in practice. Continued data collection will further establish the viability and advantages of management for gynaecomastia in stand-alone aesthetic surgery day-case centres.
Footnotes
Authors’ Contributions
S.V. conceived the concept for this article, contributing extensive experience and expertise in gynaecomastia correction surgery and supervised the co-authors, providing feedback and edits to refine the final manuscript.
S.N. conducted a literature review on existing research and knowledge related to gynaecomastia surgery and synthesised all information and authored the final version of the article.
M.C. collected and analysed patient data whilst researching existing classification systems.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.