
Abstract
The technique of large-volume fat grafting is gaining recognition in plastic and reconstructive surgery for its potential to restore facial volume and enhance aesthetic outcomes. However, a major challenge remains—the unpredictable retention of grafted fat over time. To improve consistency and long-term results, a deeper understanding of the biological mechanisms governing fat survival and integration after transplantation is essential.
This case series examines the long-term outcomes of large-volume autologous fat grafting to the face, focusing on fat survival, patient follow-up and technique refinement for enhanced facial rejuvenation.
Introduction
Autologous fat transfer has emerged as a valuable technique to address facial atrophy, restoring volume and balance to achieve a rejuvenated appearance. 1 ISAPS 2023 global statistics show 4.7% of all plastic surgery procedures involved facial fat grafting. 2 Autologous fat transplantation can be further classified into two types based on the volume of the graft: large-volume and small-volume fat grafting. There is currently no unified standard for defining large-volume fat grafting. Small-volume fat grafting typically involves grafts of <100 ml, while large-volume fat grafting generally refers to grafts between 100 and 300 ml in a single session, with some experts defining it as mega-volume fat grafting when the injection exceeds 300 ml.3-5
Ageing disrupts balanced fat distribution, causing excess and atrophy unlike the harmony of youth. Recent anatomical studies reveal that the face comprises distinct fat compartments that age independently, rather than as a single confluent mass. This compartmentalised ageing explains the predictable patterns of fat redistribution and their correlation with changes in overall body fat. 6 Areas of fat hypertrophy such as the jowls often coexist with atrophy in regions like the midface or periorbital area. This highlights the importance of precisely understanding facial anatomy and ageing when planning aesthetic interventions. Large-volume autologous fat transfer offers a promising approach to restore facial volume and balance, addressing atrophic regions while avoiding overcorrection that leads to a ‘pan-hypertrophied’ appearance.
This case series investigates the outcomes of large-volume autologous fat grafting to the face, focusing on fat survival, patient follow-up and long-term results. By analysing clinical outcomes and anatomical considerations, this study aims to refine techniques and enhance understanding of facial rejuvenation using large-volume fat grafting.
The Technique
The areas of concern were marked preoperatively. The donor site was selected and marked based on the patient’s preference and potential cosmetic benefit. Preoperative photographic documentation of both donor and recipient sites was done. Any baseline asymmetries, if any, were noted. Preoperative routine blood tests were performed. The patients were advised to stop smoking and alcohol consumption four weeks prior to the procedure.
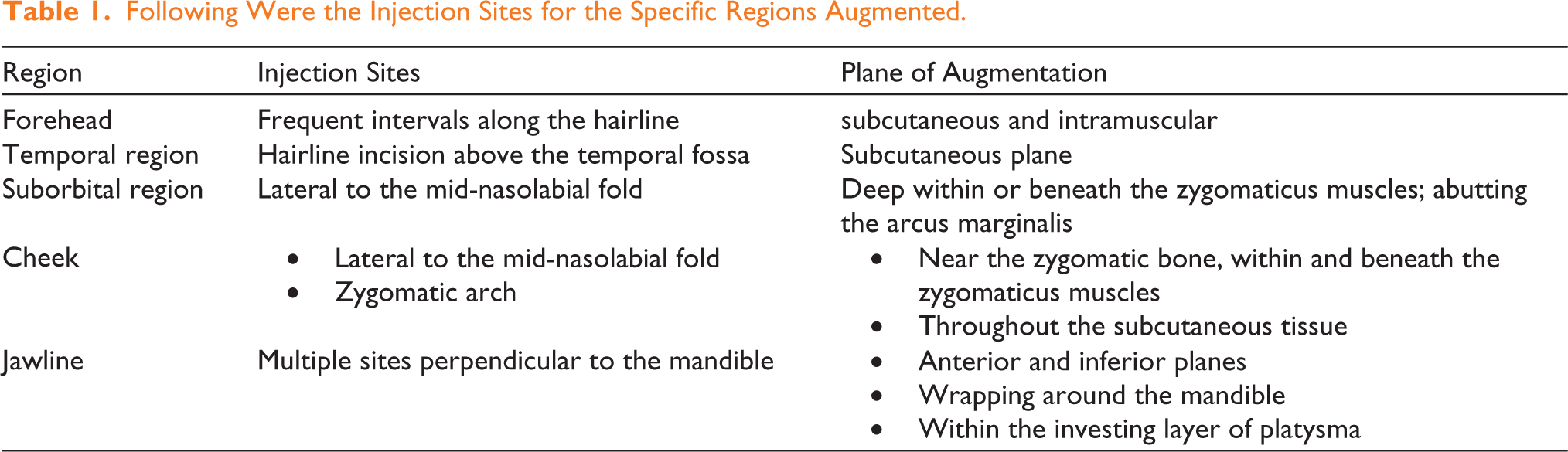
The patient was positioned on a sterile table, the procedure was done under general anaesthesia. Following administration of preoperative antibiotics, a stab incision of about 2-3 mm was made. Klein tumescent infiltration using a 2-mm cannula was done into the donor site. After 10 minutes, fat harvesting began using a 10-ml Luer lock syringe with open-tipped cannula. No centrifugation of fat was done. The fat was decanted and transferred into 1-ml syringes for injection. Dressing and compression plasters were applied to the donor sites. After prepping the face, fat was injected using a blunt 18-gauge cannula attached to a 1-ml syringe. Entry sites were made with an 18-gauge needle. The fat was injected in a radial fashion at the desired plane (direction of injection varies based on the area) (Table 1) and the areas were slightly massaged. It is important to apply even pressure to the injection cannula, with the thenar eminence of the dominant hand on the plunger, thus, placing small aliquots of fat on the withdrawal of the cannula.
Following Were the Injection Sites for the Specific Regions Augmented.
Antibiotics were initiated intraoperatively and continued until post-operative Day 5. The injection sites were cleansed, and Steri-Strips were applied. Patients were advised on managing swelling or bruising during the early post-operative period and instructed to avoid compression or pressure on the face. They were also directed to sleep in a supine position for one week. They were also instructed to avoid smoking and alcohol consumption for at least four weeks after the procedure.
Case Report
In this report, we discuss two patients who underwent the procedure.
Patient 1
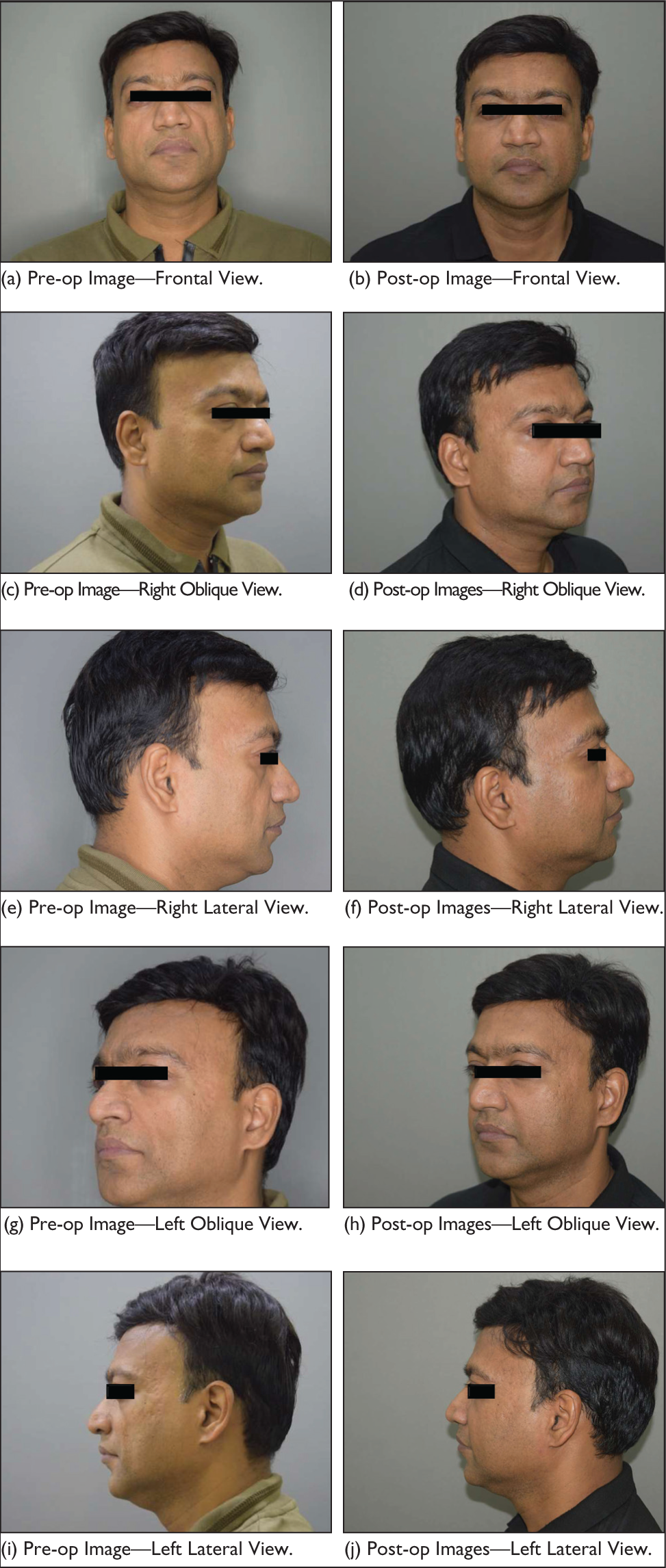
A 44-year-old patient with loss of volume in the bilateral cheek, bilateral under eye and bilateral temple regions. No known comorbidities. No habits.
Areas addressed:
Microfat
Forehead: 28 ml Brow: 4 ml each side (total: 8 ml) Temple: 18 ml right side and 20 ml left side (total: 38 ml) Suborbital area: 5 ml each side (10 ml) Mid Cheek: 15 ml each side (30 ml) Lateral cheek: 8 ml each side (16 ml) Mandible: Right side: 24 ml; left side: 20 ml (total: 44 ml) Chin: 15 ml Nasolabial fold: 5 ml each side (total: 10 ml) Labiomental folds: 4 ml each side (total: 8 ml) Lips: 2 ml Nano fat—all over the face—48 ml Total fat grafted: 257 ml
Figure 1 displays the pre-op and one-year post-op images.
A 44-year-old Patient with Loss of Volume in the Bilateral Cheek, Bilateral Under Eye and Bilateral Temple Regions—Total Volume of Fat Fill: 257 ml.
Patient 2
A 31-year-old female complained of fat loss on her face. Autologous face fat transfer [fat fill] done. Post-fat fill pictures taken after one year.
Areas addressed:
Microfat
Forehead: 30 ml Brow: 5 ml each side (total: 10 ml) Temple: 15 ml right side and 25 ml left side (total: 40 ml) Suborbital area: 6 ml each side (12 ml) Mid cheek: 15 ml each side (30 ml) Lateral cheek: 12 ml each side (24 ml) Mandible: Right side: 23 ml; left side: 21 ml (total: 44 ml) Chin: 15 ml Nasolabial fold: 5 ml each side (total: 10 ml) Labiomental fold: 4 ml each side (total: 8 ml) Lips: 2 ml Nano fat—all over the face—24 ml Total fat grafted: 247 ml
Figure 2 displays the pre-op and one-year post-op images.
A 31-year-old Female Complained of Fat Loss on Her Face—Total Volume of Fat Fill: 247 ml.

Discussion
Since 2001, Coleman has studied a procedure that uses autologous fat tissue to restore facial volume.
Fat graft survival is explained by three key theories: the host replacement theory, the cell survival theory and the graft replacement theory. The host replacement theory suggests transplanted fat is replaced by new fat cells from the recipient site. 8 The cell survival theory emphasises revascularisation, where viable adipocytes survive through blood supply, while others necrose. 9 The graft replacement theory, introduced in 2012, divides fat graft survival into survival, regenerating and necrotic zones. 10 Studies show both graft-derived and host-derived stem cells contribute to graft survival. While these theories apply to small-volume grafts, large-volume fat grafting presents unique challenges, such as reduced vascularisation and increased ischaemia, which can lead to hypoxia and cell death. 11
Large-volume fat grafting presents unique challenges distinct from small-volume procedures, primarily due to differences in oxygenation, vascularisation, and immune responses. The slower angiogenesis delays nutrient and oxygen supply, and delayed infiltration of macrophages into the graft makes large volume grafts susceptible to necrosis and fibrosis.
Thus, optimising fat graft retention in large-volume procedures involves selecting appropriate harvesting/processing/injection techniques and post-care, to minimise inflammation, apoptosis and cell damage, while promoting angiogenesis. All of the above are preferred for their ability to reduce cell trauma, enhance laminar flow, and thus higher retention rates.
In our study, we have used larger diameter cannulas for harvesting and decantation method. The fat was injected in a radial, multi-lamellar and criss-cross pattern. This technique enables the safe injection of larger fat volumes into the face by distributing the fat across multiple areas, thus avoiding the risks associated with large single-site injections.
Post-injecting gentle massaging of the area was done.
Although compartmentalised aging gives a predictable pattern of fat loss, we also advocate treating the face as a whole instead of concentrating only at the site of loss to create a more natural looking result. This has shown better long-term outcomes. Both these patients were followed up for over a year, and there were no complications.
We feel it is critical to improve the fat quality, viability and long-term retention. Irrespective of the specific surgical technique employed, a consensus exists among plastic surgeons that the implantation of a high percentage of viable adipocytes contributes significantly to the long-term efficacy of fat grafting procedures.
There are studies in the literature that a multi-faceted approach is crucial for optimising fat graft survival. This includes physical interventions and exogenous drugs to improve the graft microenvironment, as well as careful post-graft care, such as avoiding compression, providing nutritional support and considering adjunctive therapies like hyperbaric oxygen therapy to enhance angiogenesis.
However, further research is needed to understand the specific survival mechanisms in large-volume fat grafts.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Patient consent for publication of photographs was obtained.