
Abstract
Introduction:
Aesthetic surgery, while enhancing physical appearance, has significant psychological implications. This study explores the psychological factors influencing patient satisfaction following aesthetic surgery, focusing on the role of preoperative psychological screening and counselling in improving outcomes.
Methodology:
A cross-sectional study was conducted with 290 patients who underwent elective aesthetic surgery between March 2023 and December 2024. The Iowa Personality Disorder Screen (IPDS) was used to assess psychological vulnerabilities, including anxiety, body image concerns and maladaptive behaviours. Demographic factors such as gender, smoking status, prior surgeries, comorbidities and symptoms were analysed. Data were evaluated using frequency distributions, descriptive statistics and the z-test to assess significant differences among variables.
Results:
Among 290 participants, females comprised 52.1%, while males accounted for 47.9%. A prior history of psychiatric illness was reported in 3.4% of participants. The most prevalent maladaptive trait was reluctance to confide in others (23.79%), followed by bearing grudges (18.10%). Smokers exhibited significantly higher rates of mood instability (28.57%, Z = 3.67, P < .001), reluctance to confide (40.48%, Z = 16.4, P < .001) and difficulty with long-term goals (28.57%, Z = 4.05, P < .001).
Conclusion:
Addressing personality disorder is vital in aesthetic surgery to ensure successful outcomes. Preoperative psychological evaluations, setting realistic expectations and providing tailored postoperative support improve satisfaction and reduce decision regret. A holistic approach that integrates mental health care with surgical precision promotes long-term emotional well-being, making psychological support a cornerstone of patient-centred aesthetic surgical practices.
Keywords
Introduction
Aesthetic surgery has seen a significant global rise in demand due to its potential to enhance physical appearance and improve self-esteem. While many patients report positive outcomes, such as improved body image and confidence, aesthetic surgery also presents complex psychological challenges. These include anxiety, depression, body dysmorphic disorder (BDD), and postoperative regret, highlighting the need to address not only physical outcomes but also the psychological well-being of patients. 1 Understanding these psychological dimensions is critical for ensuring holistic patient care.
Unrealistic preoperative expectations and pre-existing psychological vulnerabilities are key factors influencing postoperative outcomes. For example, individuals with BDD, characterised by a distorted self-image with perceived physical flaws, may experience persistent dissatisfaction despite successful surgical results. Such patients often face heightened psychological distress, underlining the necessity of thorough preoperative psychological screening to identify at-risk individuals and provide early intervention. 2
Psychological risk assessments (PRAs) have emerged as an essential tool in the preoperative evaluation of candidates for aesthetic surgery. PRAs facilitate tailored counselling and expectation management, reducing the likelihood of dissatisfaction and postoperative regret. 3 Research indicates that inadequate psychological preparation and unrealistic expectations are primary contributors to adverse mental health outcomes post-surgery. 4
Postoperative mental health outcomes are highly variable, ranging from enhanced self-esteem and life satisfaction to ongoing psychological struggles such as anxiety, depression, or regret. These outcomes are influenced by factors such as pre-existing mental health conditions and the alignment of preoperative expectations with surgical realities. Continuous psychological support, including preoperative counselling and postoperative follow-up, has been shown to foster long-term psychological well-being and mitigate dissatisfaction.
This study explores the psychological factors influencing patient satisfaction following aesthetic surgery, focusing on the role of psychological screening and preoperative counselling in improving outcomes. The findings aim to enhance preoperative assessments, counselling strategies and postoperative care to optimise patient satisfaction and well-being.
Methodology
This study employed a cross-sectional, questionnaire-based design to investigate the psychological factors in understanding personality disorders in patients undergoing elective aesthetic surgery. The Iowa Personality Disorder Screen (IPDS), a well-validated and widely utilised tool for screening personality disorders, was used to assess psychological vulnerabilities. The IPDS was chosen for its brevity, reliability and relevance in evaluating traits such as preoperative anxiety, body image concerns and personality disorder characteristics that could impact surgical outcomes.
A total of 290 participants, all of whom had undergone elective aesthetic procedures, were included in the study. Preoperative counselling tailored to the specific surgical procedure was provided to each patient. This counselling aimed to align expectations with realistic outcomes, address body image concerns and prepare patients for the postoperative recovery process.
In the absence of tools specifically designed for assessing the psychological status of aesthetic surgery patients, the IPDS was determined to be the most suitable instrument. The IPDS consists of 11 binary (yes/no) items that assess psychological factors, including anxiety and indicators of potential personality disorders.
Data collection included demographic profiling of participants, with responses to the IPDS analysed using frequency distributions and descriptive statistics. The z-test was employed to detect the significance of differences in personality disorders according to gender, smoking status, prior surgeries, comorbidities and other symptoms. These analyses evaluated the prevalence of psychological vulnerabilities, including negative responses and concerns, and provided insights for improving patient care protocols and counselling strategies.
Results
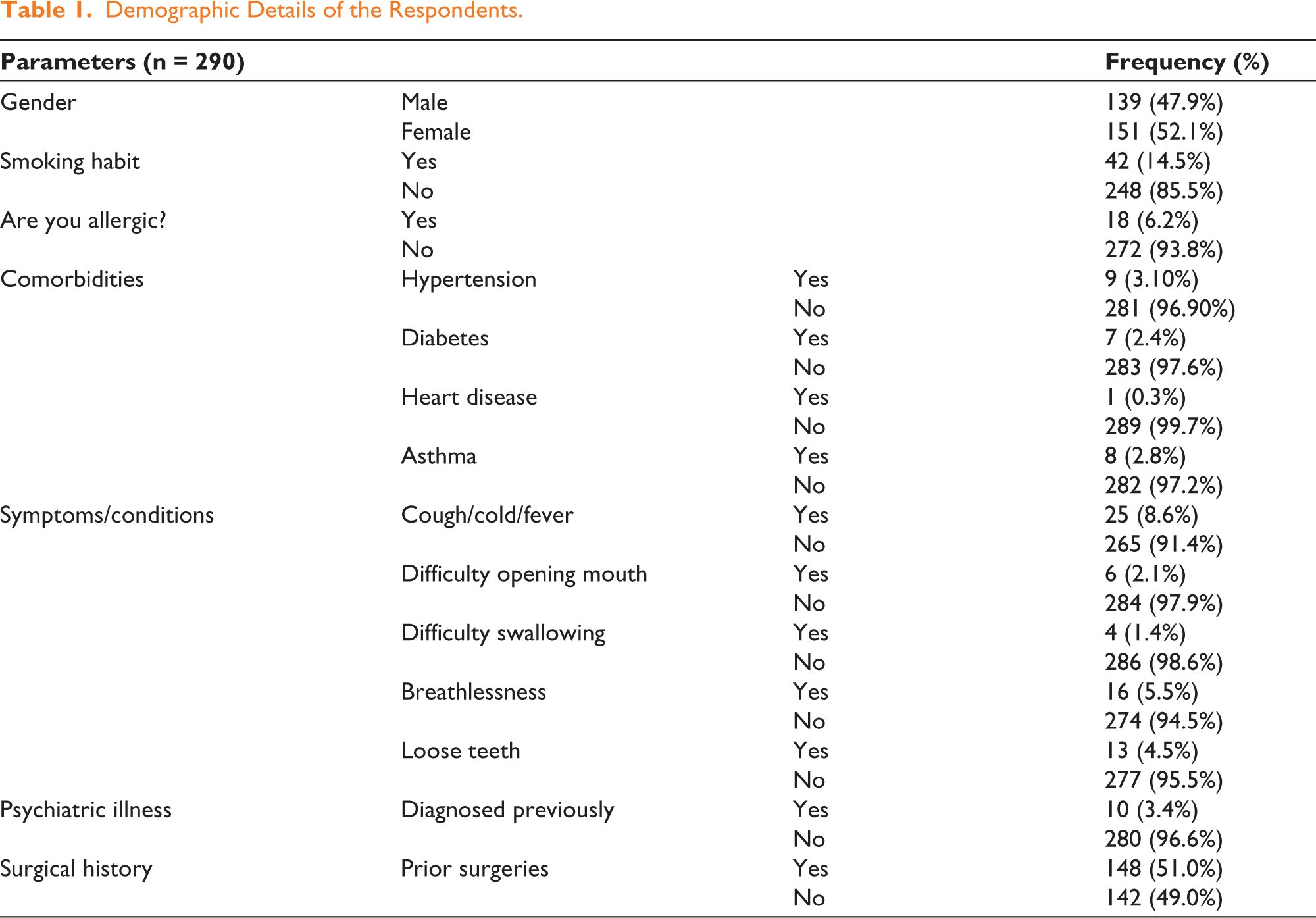
Between March 2023 and December 2024, a total of 290 patients participated in this study by completing the questionnaire. Females comprised 52.1% of the cohort, with males accounting for 47.9%. The majority of participants were non-smokers (85.5%) and reported no known allergies (93.8%). Comorbidities were infrequent, including hypertension (3.1%), diabetes (2.4%), asthma (2.8%) and heart disease (0.3%).
The main symptoms reported were cough, cold, or fever (8.6%) and breathlessness during routine activities (5.5%). Other conditions, such as loose teeth (4.5%), difficulty opening the mouth (2.1%) and difficulty swallowing (1.4%) were seen in a few cases. A prior history of psychiatric illness was reported in 3.4% of participants. Importantly, more than half (51.0%) had undergone previous surgical interventions (Table 1). The responses on personality disorder screening have been categorised as major (reported by more than 15%), Moderate (reported by 10%-15%) and Minor (reported by less than 10%). The most commonly reported maladaptive trait was reluctance to confide in others (23.79%), followed by bearing grudges or being unforgiving (18.10%). As these traits were identified in a significant portion of the sample, they suggest a notable impact on interpersonal dynamics (Table 2).
Demographic Details of the Respondents.
Responses as per the Questionnaire.
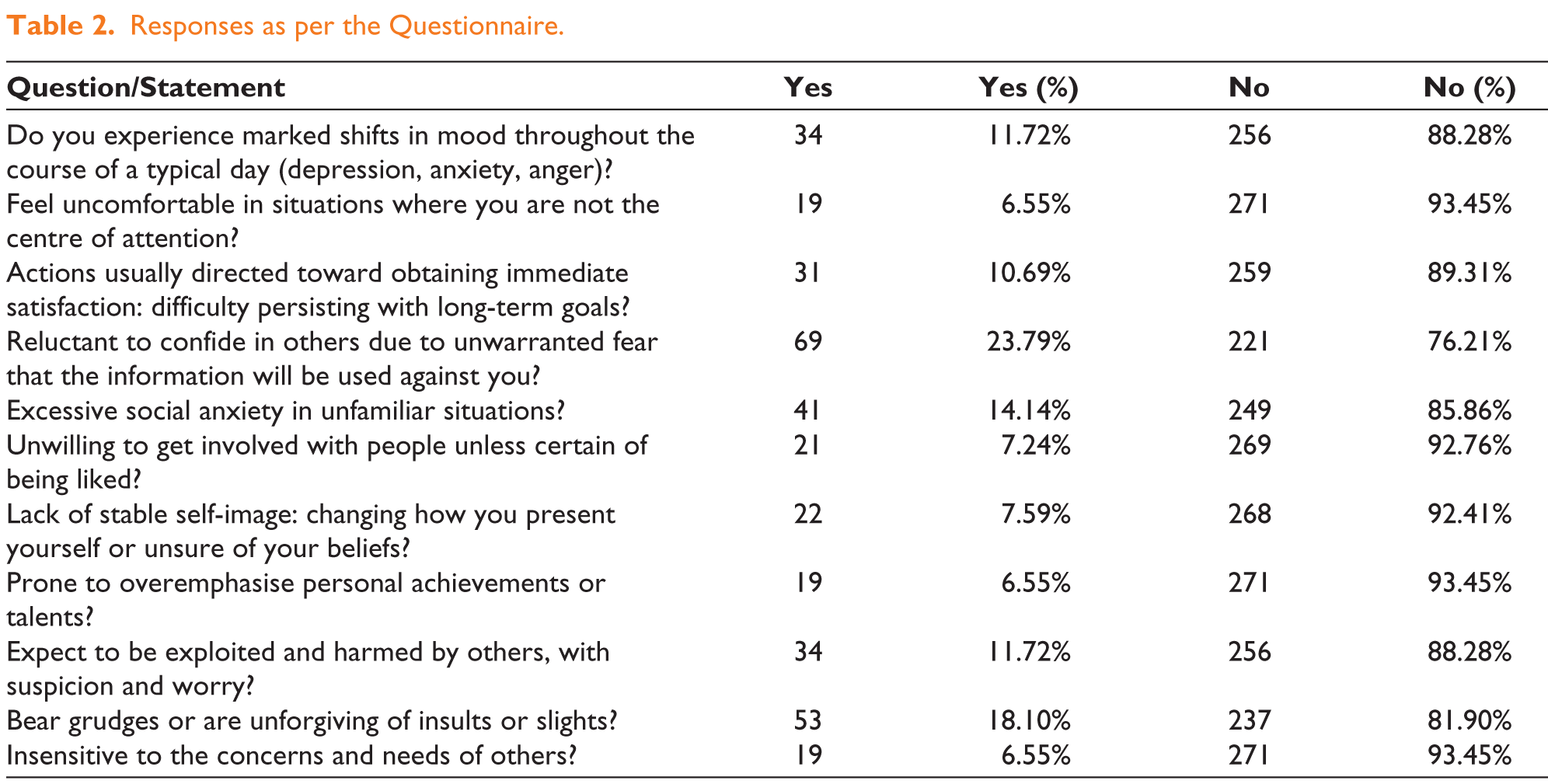
Moderate personality disorders included excessive social anxiety in unfamiliar situations (14.14%), mood instability (11.72%), fear of exploitation (11.72%) and difficulty in pursuing long-term goals (10.69%). Other maladaptive tendencies, such as overemphasising achievements, an unstable self-image, and insensitivity to others’ concerns, were observed in less than 10% of participants. Among the major and moderate personality disorders, Smokers showed a significantly higher prevalence of maladaptive traits, including mood instability (28.57%, Z = 3.67, P < .001), reluctance to confide in others (40.48%, Z = 16.4, P < .001) and difficulty with long-term goals (28.57%, Z = 4.05, P < .001) (Table 3).
Differences in Personality Traits as per Gender, Smoking Status, Prior Surgeries and Other Symptoms.
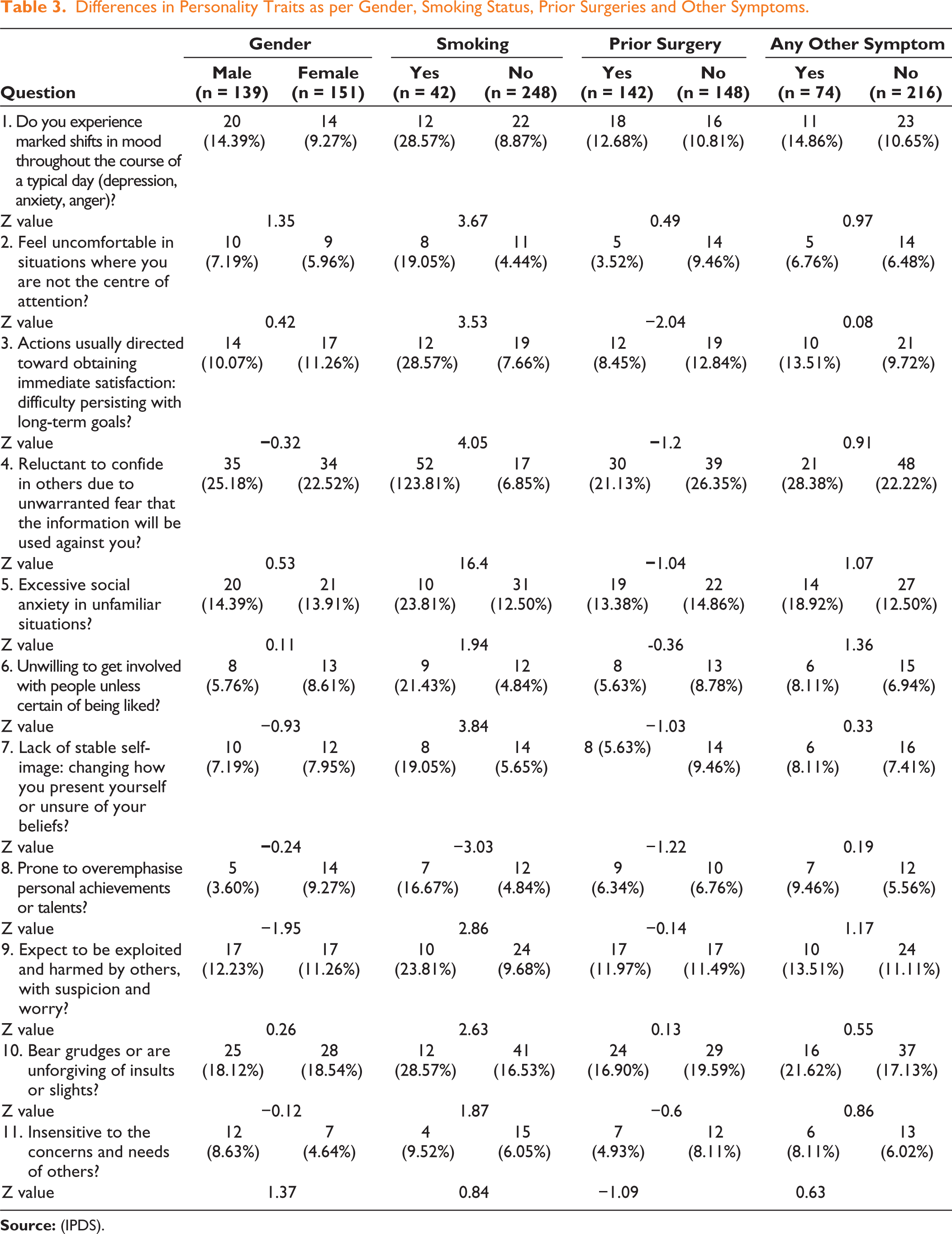
Females were more likely to overemphasise achievements (9.27% vs. 3.60%) and males exhibited slightly higher rates of mood instability (14.39% vs. 9.27%). However, the differences were not statistically significant.Those who had previously undergone surgeries showed a lower prevalence of the personality disorder trait of feeling uncomfortable in situations where they are not the centre of attention (3.52% vs. 9.46%, Z = 2.04, P < .05) (Table 3).
Among the 11 personality-based questions in the Iowa questionnaire, one patient answered ‘yes’ to 10 questions, while two patients answered ‘yes’ to all 11. These three patients (1.03%) experienced a challenging recovery period. They required substantially more counselling time after surgery and remained dissatisfied during the postoperative phase.
No significant differences were observed between participants with the presence of any other symptoms and comorbidities. These findings underscore the importance of understanding personality disorders and integrating comprehensive psychological screening tools, such as the IPDS, into routine preoperative assessments with modifications in the Indian context.
Discussion
Aesthetic surgery offers the potential to transform physical appearance and boost self-esteem, but its psychological aspects play an equally critical role in determining outcomes. While it can enhance self-perception, it may also exacerbate underlying psychological issues, especially in individuals with unrealistic expectations or personality-related concerns.
Unrealistic expectations, as seen in high-profile cases like Michael Jackson, have been significant obstacles to achieving satisfaction. This dissatisfaction underscores the profound impact of BDD and a distorted self-image. Using the IPDS, we identified maladaptive traits that were predictive of postoperative regret. Consistent with the findings of Sarwer et al., 1 we emphasised that early detection of these traits allows for targeted interventions, reducing the likelihood of negative psychological outcomes.
Smoking emerged as a key lifestyle factor linked to increased psychological vulnerabilities, such as mood instability and challenges in maintaining long-term goals. Hollander et al. 5 proposed that addressing these vulnerabilities through focused counselling could enhance surgical outcomes. Moreover, gender-specific patterns were observed: female patients tended to place excessive importance on personal achievements, influenced by societal standards of appearance, 6 while male patients, although less socially anxious, faced difficulties with their self-image.
Patients who answer ‘Yes’ to most of the questions (10 or more) on the IPDS should undergo detailed preoperative counselling, not only by the surgical team but also by psychologists. Even after a successful surgical outcome, such patients can cause significant mental stress for both the surgical team and the patient’s family. We recommend that these patients receive psychological clearance before surgery to ensure they have realistic expectations following aesthetic procedures.
Structured preoperative counselling played a crucial role in aligning patient expectations with realistic outcomes. Consistent with the findings of Rankin et al. 4 and Klassen et al., 7 our study demonstrated that patients who underwent such counselling were emotionally better prepared, resulting in reduced decision regret. These counselling sessions also addressed concerns about social anxiety, helping to build psychological resilience. Additionally, social support was identified as a key factor in promoting emotional resilience and long-term satisfaction, as highlighted by Furnham and Levitas. 8
Our study reinforced the importance of incorporating mental health into the aesthetic surgery process, highlighting that collaboration between surgeons, psychologists and counsellors can minimise dissatisfaction and promote both physical and emotional well-being, as emphasised by Thompson et al. 9 and von Soest et al. 10
We also stressed that dissatisfaction rooted in psychological distress cannot be resolved by surgeons alone. Achieving lasting satisfaction requires addressing the patient’s emotional and mental needs throughout the surgical journey. 11
There are opportunities for further enhancement, such as expanding the sample size and ensuring a more homogeneous group, minimising reliance on self-reported data and incorporating long-term follow-up. Additionally, establishing causality between psychological factors and satisfaction presents an exciting avenue for future research.
Conclusion
Addressing personality disorders in aesthetic surgery is crucial for success. Preoperative psychological assessments, managing expectations and personalised postoperative care ensure safer, patient-centred outcomes. A holistic approach enhances satisfaction, minimises regret and supports long-term emotional well-being, making mental health support essential in modern aesthetic practices.
Footnotes
Acknowledgements
The authors would like to acknowledge Team APAR Health for medical writing assistance and data analysis (CARE Program).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.