
Abstract
Background:
Melasma is a hyperpigmentation disorder characterised by irregular brown to grey-brown facial patches. Managing melasma is challenging due to limited curative treatments and high recurrence rates.
Objective:
The aim of this study was to evaluate the efficacy of a standardised treatment protocol to treat melasma, reduce recurrence and improve quality of life.
Materials and Methods:
A retrospective analysis of 34 patients treated with our standardised multimodal treatment was done. A single session of controlled depth peel was followed by maintenance treatment with exfoliant/depigmenting actives. If deeper melanin persisted, microneedling or a Q-switch laser was performed. Severity was assessed using the Modified Melasma Area and Severity Index (mMASI), and quality of life was measured with the Melasma Quality of Life Scale (MelasQoL). Treatment outcomes were assessed after six months of completing treatment.
Results:
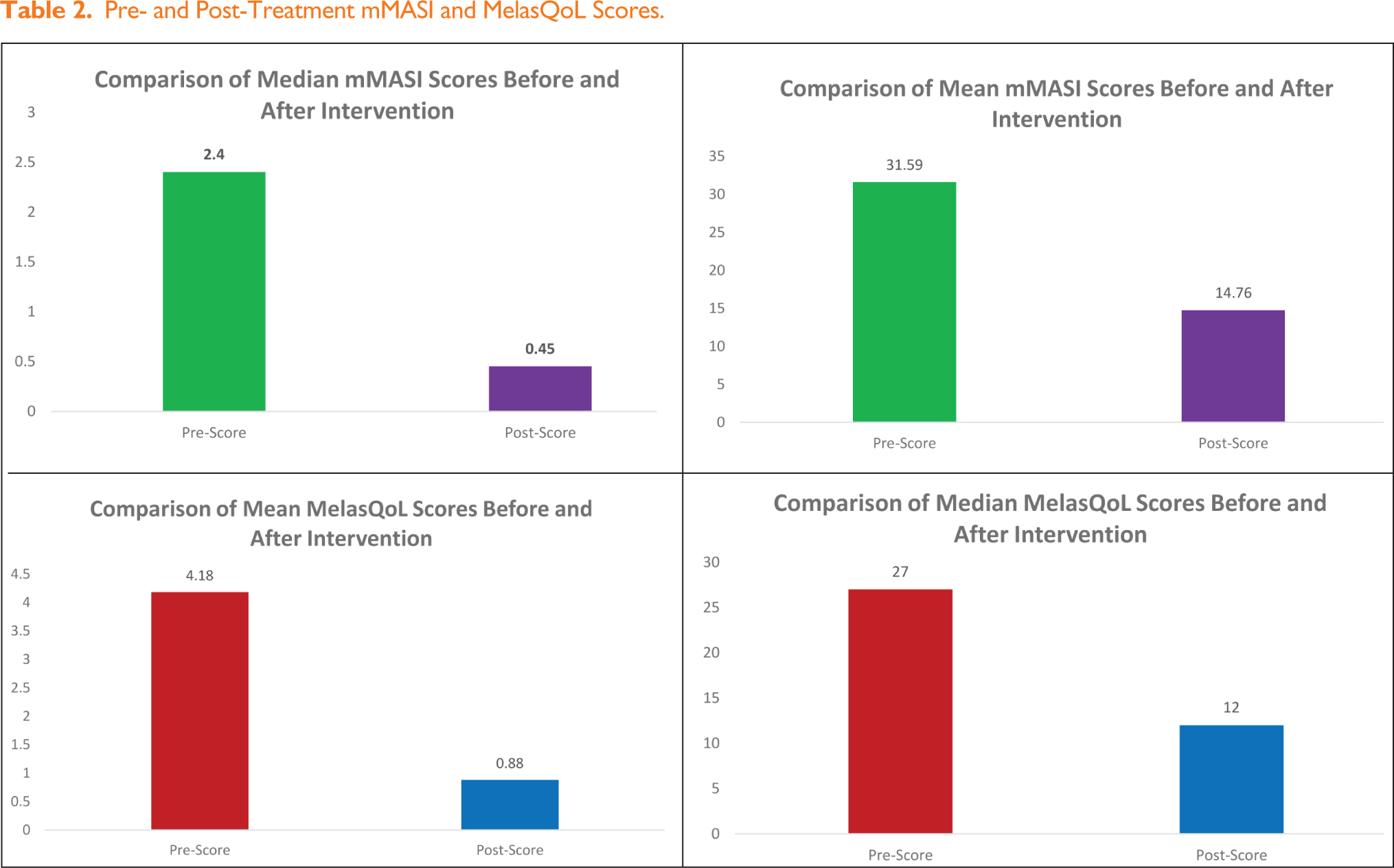
The mean MelasQoL score improved from 31.59 ± 15.46 to 14.76 ± 7.57, while the mean mMASI score decreased from 4.18 ± 3.97 to 0.88 ± 1.43 (P < .001). Of the total patients, 82% were satisfied with the improvement.
Conclusion:
A standardised treatment protocol combining topical depigmenting actives, procedural interventions and systemic therapy is effective in reducing the clinical severity and recurrence whilst improving the quality of life in the management of melasma.
Introduction
Melasma is a common hyperpigmentation disorder, characterised by irregularly shaped brown to grey-brown symmetric patches affecting sun-exposed areas of the face such as the cheeks, forehead and chin. 1 The overall prevalence ranges from 8.8 to 40%, depending on the ethnicity of the population and the geographical area.2-4 It predominantly affects women, especially those with Fitzpatrick skin types (FST) III-V. 2
The pathogenesis of melasma is multifactorial, involving genetic predisposition, hormonal factors, ultraviolet (UV) radiation and other environmental influences. 5 Histologically, melasma exhibits increased epidermal and/or dermal pigmentation, with enlarged melanocytes and a higher number of melanosomes. This may be confounded by other findings like solar elastosis, increased dermal blood vessels and perivascular lympho-histiocytic infiltrates.6,7
Management of melasma remains a challenge due to its chronic nature, limited curative options and high recurrence rates. 8 The condition not only impacts physical appearance but also adversely affects quality of life (QoL), underscoring the need for comprehensive, personalised approaches. 9
Current treatments include sun protection, oral and topical depigmenting agents and in resistant cases, procedural interventions often with varying degrees of success based on patient-specific factors.10,11 No single treatment has demonstrated consistent results. Thus, a multimodal treatment along with avoidance of exacerbating factors such as UV light exposure and hormonal contraception should be considered.12-14 This study aims to retrospectively evaluate the efficacy of a standardised multimodal treatment in reducing melasma severity, decreasing its recurrence and improving the patients’ QoL.
Materials and Methods
Study Design and Participants
This retrospective study evaluated data from 34 patients with melasma treated at a standalone aesthetic centre. Participants were included based on a specific criteria: clinical diagnosis of melasma between 18 and 65 years. Patients were excluded if they were pregnant, breastfeeding, had used oral contraceptives in the past 12 months, had a history of coagulation disorder/ thrombotic condition, were on anticoagulant medications or had active dermatological conditions such as herpes simplex lesions or facial warts. Patients were also excluded if the follow-up period was less than six months.
Treatment Protocol and Assessment
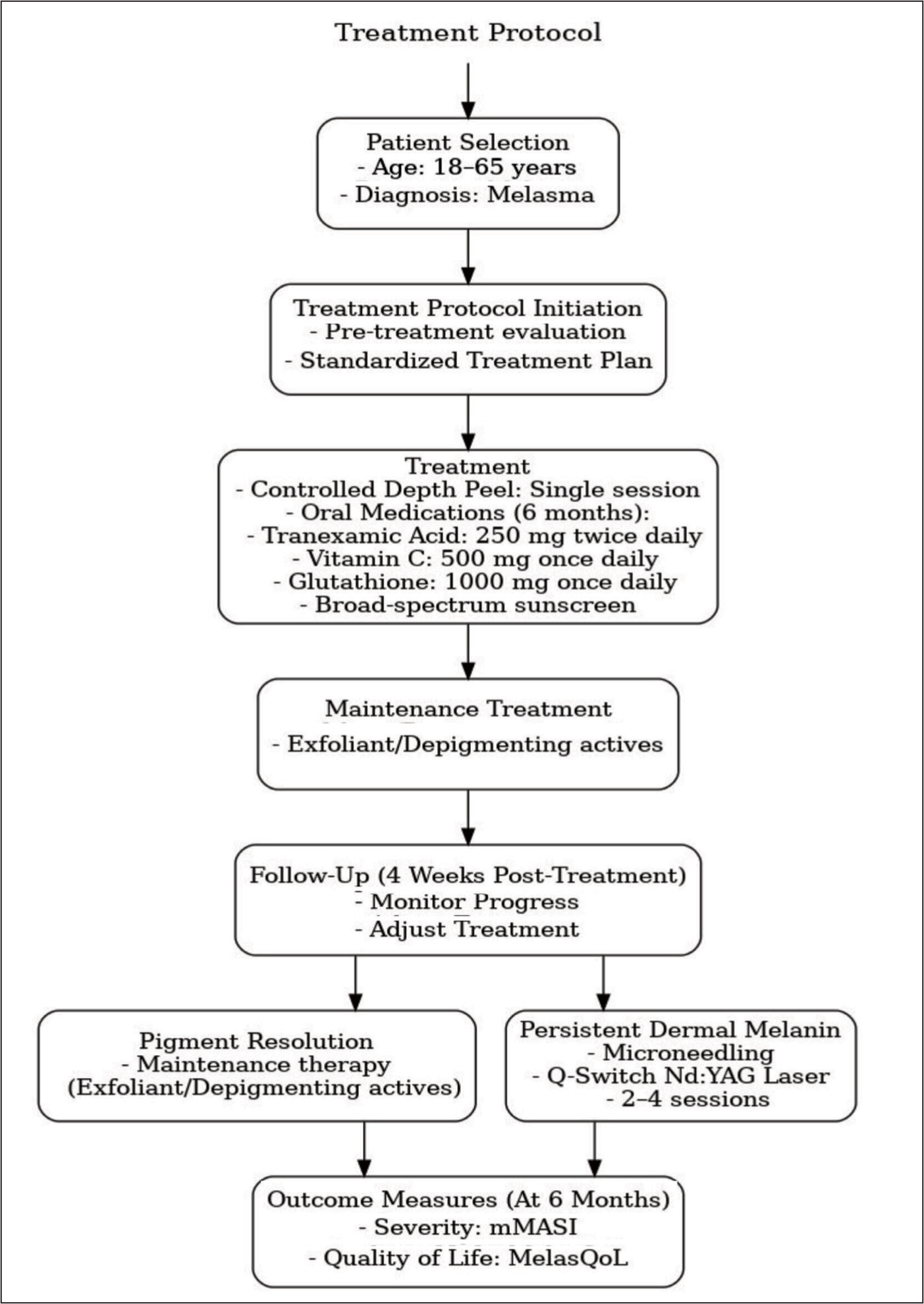
A single session of controlled depth peel (Cosmelan→ or Dermamelan→ depigmentation treatments by mesoestetic) was performed. This depigmenting treatment consists of an intensive phase where a peel is applied in-clinic settings and left on the skin for six to eight hours. This peel is then washed off with cold or lukewarm water at home. Subsequently, the patient begins the in-home treatment with a depigmenting cream consisting of multiple depigmenting actives like kojic acid, arbutin, vitamin C, retinoic acid to gradually reduce the pigment levels in the newly formed keratinocytes. Along with these depigmenting actives, 4% hydroquinone (4% HQ) is combined to achieve the desired bleaching effect; 6% or 12% glycolic acid is added for exfoliation. Patients were reviewed at four weeks to monitor progress and adjust the treatment plan, if needed.
If the pigmentation is resolving, patient is continued on the in-home treatment. If deeper pigment or dermal melanin is persisting during the treatment, microneedling with brightening/ depigmenting serums or Q-switch neodymium-doped yttrium aluminium garnet (Nd:YAG) laser was performed in two to four sessions, depending on the severity. The treatment is continued for six months following which the depigmenting actives/ exfoliants are continued with modified dosage/ frequency. The treatment protocol also included oral/ systemic therapy combining tranexamic acid (TXA; 250 mg twice daily), glutathione (1000 mg once daily) and vitamin C (500 mg once daily) (Figure 1).
Flowchart of Our Standardised Treatment Protocol for Melasma.
Outcome Measures
Demographic parameters were documented including age, sex and FST. The lesions were categorised based on their distribution, as either centrofacial, malar or mandibular and by type, as either epidermal, dermal or mixed melasma based on dermoscopy. 15 The effectiveness of the treatment was evaluated using two primary metrics. The severity of Melasma was assessed using the Modified Melasma Area and Severity Index (mMASI), while the impact on the patients’ QoL was measured using the Melasma Quality of Life Scale (MelasQoL). 16 These assessments were performed at the start and at six months after the completion of treatment.
Statistical Analysis
Statistical analyses were performed using SPSS version 21.0. The Shapiro–Wilk test was used to assess the normality of continuous variables, including mMASI and MelasQoL scores. As the data did not follow a normal distribution, the Wilcoxon signed-rank test, a non-parametric test for paired data, was employed to evaluate significant differences between pre- and post-treatment scores. Results were summarised using both mean ± standard deviation (SD) and median values with interquartile ranges (IQR), providing comprehensive insights into central tendency and variability. The mean values highlighted overall trends, while medians and IQRs minimised the influence of outliers in non-normal datasets. A P value of < .05 was considered statistically significant.
Confidentiality and Privacy
Informed consent was obtained. The data was collected by adhering to the ethical principles outlined in the Declaration of Helsinki 1975 (revised in 2008). Patient data were securely masked prior to analysis to prevent the identification of individuals. All records were stored securely and accessed only by authorised personnel.
Results
The cohort consisted of 94.1% females, with a mean age of 42.27 years (range 26–58). The most common age group was between 41 and 50 years (21–30 years—5; 31–40 years—9; 41–50 years—13; 51–60 years—7). The study participants were classified according to FST III-VI (see Table 1). Additionally, mixed-type melasma was the most common category in the clinical spectrum of melasma.
Distribution of Melasma Patterns, Fitzpatrick Skin Types, and Dermatoscopic Types in Study Participants.
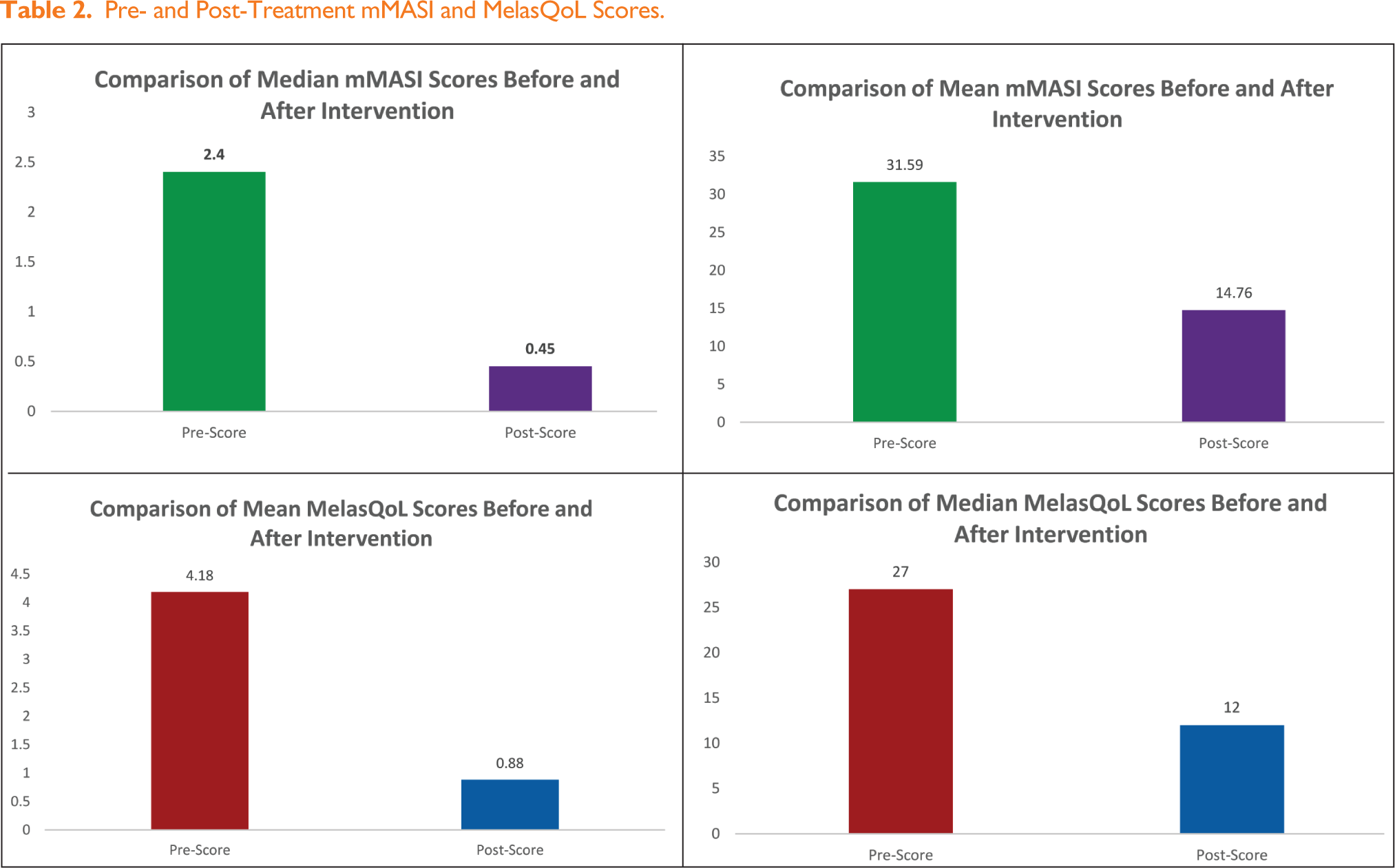
Post-treatment, the mean MelasQoL score improved from 31.59 ± 15.46 to 14.76 ± 7.57, while the mean mMASI score decreased from 4.18 ± 3.97 to 0.88 ± 1.43 (see Table 2). A Wilcoxon signed-rank test showed that post-treatment MelasQoL scores were significantly lower compared to pre-treatment scores (Z = −5.088, P < .001). Similarly, post-treatment mMASI scores were significantly lower compared to pre-treatment scores at six months (Z = −5.091, P < .001). The data shows a significant reduction in both pre-mMASI (median: 2.40, IQR: 1.80–5.18) to post-mMASI (median: 0.45, IQR: 0.00–0.90) and pre-MelasQoL (median: 27.00, IQR: 18.25–41.50) to post-MelasQoL (median: 12.00, IQR: 10.00–16.75) median scores.
Pre- and Post-Treatment mMASI and MelasQoL Scores.
Subgroup analysis indicated that patients with FSTs III and IV showed the most notable improvements. Of the total patients, 82% were satisfied to extremely satisfied by the improvement (28 out of 34 patients); 15% of the patients had relapse of the condition (5 out of 34 patients).
Discussion
Melasma is a chronic pigmentary disorder characterised by progressive worsening of the hyperpigmented patches as the patient is repeatedly exposed to hormonal stimulation and worsened by the environmental exposure. The presence of patches on the face, high recurrence rates and expensive treatments leads to reduced self-esteem, negatively affecting the QoL. Despite a strong therapeutic need, the treatment of melasma is challenging, as the patches are not cleared completely in most patients and recurrences are frequent. As we have developed a greater understanding of the pathophysiology behind development of this condition, newer treatment modalities have been added as part of a multimodal approach to achieve superior results.
The majority of melasma patients in our study belonged to FST III, IV and V. Also, females were more affected than males. This is similar in occurrence to other large scale studies.17,18 In a study with 302 melasma patients in Brazil, 34% of patients had FST III, 38% had FST IV and 16% had FST V. 19 Similarly, a study in Tunisia consisting of 188 melasma patients demonstrated that 14% of patients had FST III, 45% had FST IV and 40% had FST V. Another study in Brazil with 953 melasma patients showed a distribution of 13% patients with FST II, 36% with FST III, 40% with FST IV and 10% with FST V. 20 These findings suggest that the representation of FSTs in melasma studies closely mirrors the condition’s prevalence in different skin types.
Topical bleaching agents are considered the go-to treatment option for melasma. Triple combination creams (TCC) consisting of 4% HQ + 0.05% retinoic acid + 0.01% fluocinolone acetonide have remained the gold standard therapy for melasma and considered more effective than other individual/ dual combination therapies. However, the long-term use of TCC as maintenance therapy is not recommended as there is risk of atrophy, telangiectasias and other cutaneous side effects with daily usage against the disadvantage of incomplete resolution or recurrence with short-term usage. 1
Our study is unique in that a controlled-depth peel was used as a dual treatment modality (chemical peel followed by long-term topical depigmenting regimen). Standard chemical peels deliver high concentrations of exfoliating acids to the skin to brighten the complexion, even skin tone and to improve the appearance of patches in melasma. A peel can help fade the spots but the blemishes will appear again if the mechanisms that produce it are not addressed. The controlled depth peel treatment not only removes and attenuates spots (just like a peel) but it also provides a regulating action to correct the overproduction of pigmentation and prevent the spots’ reappearance. While chemical peels act on the surface of the problem, the controlled depth peel treatment targets the origin thereby reducing the chances of recurrence in melasma. A single session of controlled depth peel is also advantageous to repeated sessions of a standard chemical peel to avoid skin thinning, post-inflammatory hyperpigmentation (PIH) and the associated risk of rapid aging due to repeated exfoliation.
If after consistent use of topical depigmenting actives, deeper pigment or dermal melanin still persists, microneedling with brightening/ depigmenting serums like glutathione, vitamin C, and TXA or Q-switch Nd:YAG laser was considered. These procedures are able to address the deeper melanin trapped in the dermal layer. Microneedling allows the depigmenting serums to penetrate deeper into the dermis, whereas Q-switch Nd:YAG laser destroys the trapped intra-dermal melanin by photoacoustic effect rather than photothermolysis. This prevents further inflammation in the dermis and the subsequent risk of PIH.
In addition to topical therapy and in-clinic procedures, oral or systemic depigmentation therapy is emerging as a complementary treatment option for melasma. Our treatment protocol included oral TXA (250 mg twice daily), oral glutathione (1000 mg once daily) and vitamin C (500 mg once daily) for six months. In our opinion, ours is the first study that combined the benefits of three oral agents that have individually shown promise in melasma. No side effects were reported following the use of these depigmenting/anti-oxidant medications.
TXA in the form of oral or topical therapy has proven effective in the treatment of melasma. It contributes to depigmentation by two main mechanisms: affecting melanin synthesis by inhibiting the plasminogen-plasmin pathway and by controlling the vascularity of dermis. A systematic review including 22 studies and 1280 patients found TXA to be beneficial against melasma, either alone or in combination with other treatments. Also, the meta-analysis showed a greater MASI score reduction in treatments involving TXA. The optimal dose of this drug is 250 mg two or three times per day for 12 consecutive weeks.21,22 Due to rare risk of deep vein thrombosis, screening for risk factors needs to be done before initiating treatment with TXA. 1 Oral glutathione has anti-melanogenic and antioxidant properties and has become popular as a skin lightening agent. A systematic review of the impact of glutathione in melasma showed a reduction in melanin index as compared to placebo. The doses ranged from 250 to 500 mg once a day. Our study is different in that patients received 1000 mg once day. No side effects were reported by the patients in our study. 23 Vitamin C or ascorbic acid is a potent anti-oxidant and a reactive oxygen species (ROS) scavenger. Oral vitamin C supplementation has been studied for the treatment of hyperpigmentation disorders including melasma and found to be effective in combination with other treatments.1,24
The combination of topical depigmenting/bleaching actives with oral medications and in-clinic procedures can provide faster and predictable results, although strategies for the prevention of further relapses are poorly reported. The use of controlled depth peel in our study removes and attenuates spots whilst providing a regulating action to correct the overproduction of pigmentation and prevent recurrence.
Consistent sun protection mitigates UV radiation’s role in melanocyte activation, which is crucial for both treatment success and recurrence prevention. Sunscreens containing iron oxide offer protection against the shorter wavelengths of visible light besides the broad UVA and UVB protection.5,25,26 Incorporating patient education on photoprotection into the treatment protocol further empowered participants to actively manage their condition.
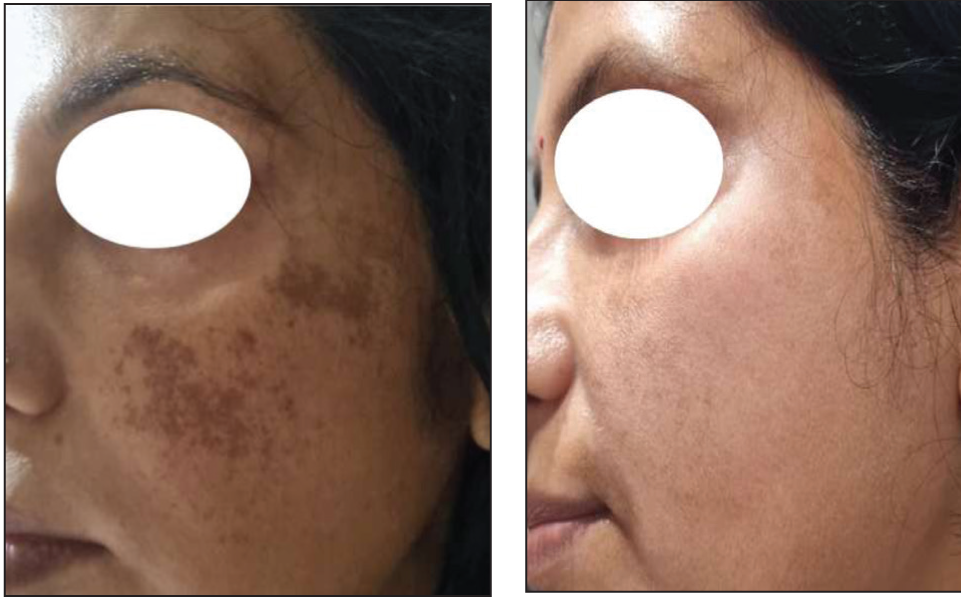
The significant reduction in mMASI scores (75%) and improvement in MelasQoL scores (53.8%) reflect the effectiveness of our standardised multimodal treatment in addressing both the clinical and psychosocial dimensions of melasma. These results also highlight the importance of addressing melasma as a multipronged approach with a combination of treatments tailored to each individual especially in patients with FST IV-VI and mixed-type melasma (see Figures 2–11). These groups often present a greater challenge due to increased melanin activity and deeper dermal involvement.
and 3. Before and After Treatment Images of a 38-Year-Old Female with FST III and Malar Melasma: Pre mMASI-9 and Post mMASI-0.6.

Before and After Treatment Images of a 45-Year-Old Female with FST IV and Malar Melasma: Pre mMASI-4.5 and Post mMASI-0.3.

Before and After Treatment Images of a 33-Year-Old Female with FST IV and Malar Melasma: Pre mMASI-1.8 and Post mMASI-0.

Before and After Treatment Images of a 47-Year-Old Female with FST IV and Malar Melasma: Pre mMASI-1.8 and Post mMASI-0.3.
Before and After Treatment Images of a 56-Year-Old Female with FST IV and Pre mMASI-3.6 and Post mMASI-0.

A robust combination of controlled depth peel, topical bleaching treatment with 4% HQ and other depigmenting actives, triple combination oral/systemic depigmentation therapy, consistent sun protection and patient education contributed to the superior outcomes observed in our study. Additionally, specific targeting of dermal melanin using Q-switch Nd:YAG laser whilst minimising PIH and microneedling to disrupt melanin deposits whilst stimulating collagen remodelling has complemented the effects of topical depigmenting actives. Comparative studies have suggested that multimodal therapies have superior outcomes than monotherapies. 11 This aligns with the current study’s findings, supporting the notion that an approach targeting multiple pathogenic pathways yields superior results.
Limitations
Despite these strengths, certain limitations warrant further investigation. The study’s cohort of 34 patients limits the generalisability of the findings. Larger, multi-centre studies are needed to validate the efficacy of this multimodal protocol across diverse populations and help refine treatment protocols. The retrospective design limits the ability to control confounding variables, while a shorter (6 month) follow-up period does not address melasma’s long-term recurrence rates. A longer duration of observation would provide insights into the durability of treatment effects and the frequency of relapse.
Additionally, integrating psychosocial support and counselling could address the substantial psychological burden associated with melasma, as studies indicate that improved mental well-being correlates with better adherence to treatment protocols .
Conclusion
A standardised multimodal treatment combining topical depigmenting actives, procedural interventions and oral/systemic depigmentation therapy is effective in achieving durable remission while minimising recurrence in the management of melasma.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.