
Abstract
Autologous fat grafting has been shown to enhance breast, but its use as a standalone treatment for breast reconstruction after mastectomy is underexplored. This case report evaluates the efficacy of fat grafting in restoring breast aesthetics post-unilateral mastectomy and radiation. A 28-year-old female with recurrent ductal carcinoma-in-situ underwent nipple sparing mastectomy (NSM) with radiation, resulting in severe breast scarring, volume loss and nipple-areola complex distortion. She opted for multisession autologous fat grafting to avoid implants and external scars. The patient underwent five sessions of fat grafting, starting immediately after mastectomy, using the Coleman technique. The patient achieved satisfactory volume restoration. This case highlights that fat grafting can be an effective standalone method for breast volume restoration post-mastectomy even in unilateral cases and is oncologically safe. While multiple sessions are required to achieve optimal results, fat grafting offers natural consistency, minimal donor-site morbidity and improved breast symmetry.
Introduction
There is enough evidence in the literature which supports the cosmetic enhancement of the breast in terms of size and shape with the use of autologous fat. However, post-oncosurgical breast defects still continue to pose a challenge to plastic surgeons who have attempted to restore the form in such cases using various methods like loco regional flaps, free flaps, implants and grafts. This case highlights that fat grafting can be used as an efficient standalone tool in the armamentarium of a plastic surgeon for restoration of breast volume and contour and not just as an adjunct to other reconstructive options.
Case Report
A 28 year old female was diagnosed with ductal carcinoma in situ of the left breast in 2019 for which she underwent lumpectomy followed by radiation therapy. Sentinel lymph node biopsy was negative. Patient had a recurrence in the upper quadrant of the left breast in 2021 and was advised to undergo nipple sparing mastectomy (NSM). She was also counselled for breast reconstruction, and various options were discussed. Since the patient was young, nulliparous, unmarried, she did not opt for any foreign implant, extensive scarring in other body parts, use of external prosthetics or changes in the contralateral breast. Therefore, after thorough discussion, sequential fat grafting was chosen as the treatment of choice. Patient underwent NSM in 2021 followed by immediate intraoperative session of fat grafting; 120ml of micro fat was grafted in the muscle and nanofat in the skin flaps under vision. Further radiotherapy was planned for her by the radiation oncologist.
On her follow up visit post healing and drain removal, the surgical site was examined, there was extensive scarring of the left breast with obvious volume deficit, contraction of the nipple areola complex (NAC), scaring along the incision line, superiorly displaced inframammary fold due to fibrosis with difference in the levels of bilateral NAC. The goal was not only to add volume but also to expand the footprint and release the scars, providing as much symmetry as possible.
She underwent a total of 5 sessions of fat grafting and rigottomy 1 at an interval of 3-4 months each over a period of 1.8 years. All the procedures were performed under total intravenous sedation after thorough pre-anaesthetic work up and markings. A standard Coleman approach was used to harvest the fat from either medial or later aspect of thigh or abdomen in each of the sessions. A tumescent fluid containing (1 Litre NS, 10ml Loxicard, 5ml 0.2% ropivacaine and 1 ml adrenaline) was used with manual infiltration the donor area as per superwet technique. A Tonnard harvester super luerlock (2.4mm × 20cm) multihole aspirator was used to aspirate the fat after a contact time of 15 minutes. Fat was processed by washing and decantation.
An average of 340 ml of fat was injected intramuscularly and subcutaneously in the following subsequent grafting sessions. Conservative rigottomy was done in each session with focus on inferior and lateral quadrants to expand the plane by releasing the fibrosed tissue. For subareolar & incision scar, 2 sessions of triamcinolone injections and nano fat grafting were done; 3 months after the final session, micropigmentation tattooing of the areola was done for cosmetic improvement. There were no associated complications and we were able to deliver excellent aesthetic symmetry after the final procedure.
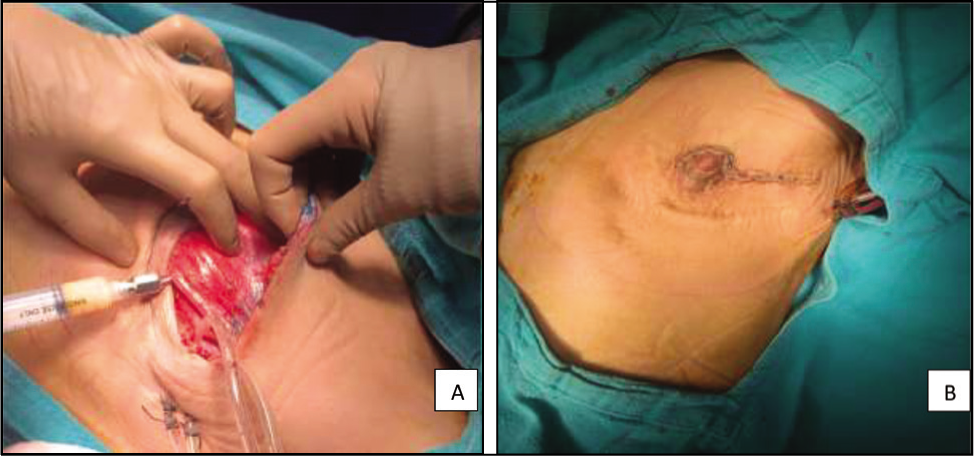
A. Intramuscular Fat Grafting Immediately Post-NSM; B. Immediately After Closure Post-NSM and Fat Grafting.
Presentation Post-NSM Showing Severe Volume Deficit with NAC and Incision Contracture.

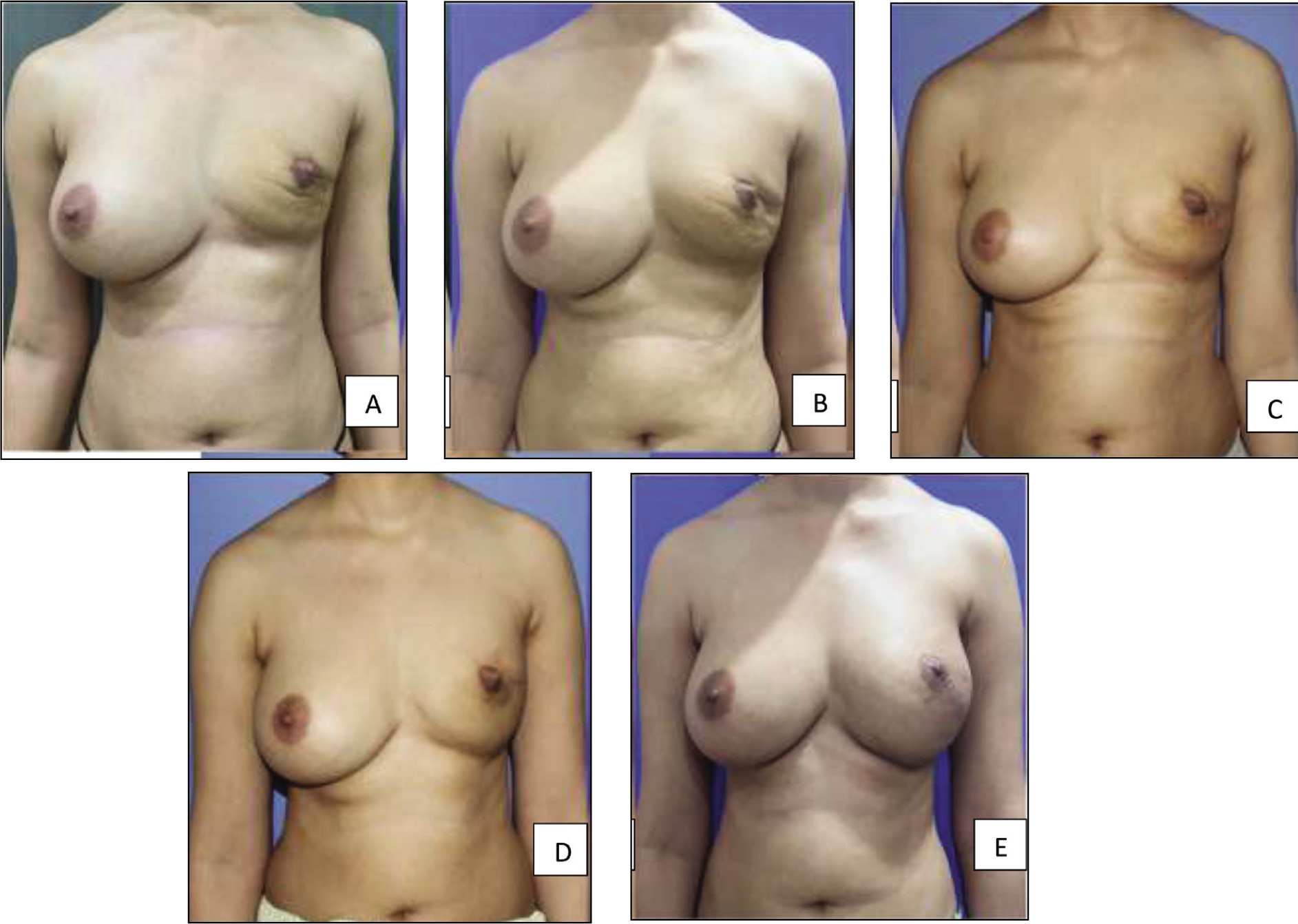
A. Immediately post NSM and 1st session of fat grafting (120cc); B. After 2nd session (320cc); C. After 3rd session (380cc); D. After 4th session (320cc); E. After 5th session (340cc).
Discussion
Recent studies have established that autologous fat grafting has the potential to replace or act as an alternate option for recontouring of the breast in various medical conditions.2,3 However there is still a paucity of literature available that has emphasized the role of autologous fat grafting as a standalone modality for breast contouring post mastectomy. The main surgical goal in this case was to correct the severe volume deficit in the left breast along with scar release since the right breast of the patient was of a relatively larger volume. However, this had to be done while maintaining the viability of the overlying skin envelope and ensuring sufficient graft take in each session which posed a higher degree of surgical challenge.
The number of sessions and volume can vary depending on the desired final outcome. We are proponents of multiple sessions of moderate volume to maximise the graft uptake and safely expand the skin envelope. Clinically, volume loss has been reported between 40% and 60%.4,5 Also, a larger volume can reduce the surface area contact between graft and recipient, delaying neovascularisation of the graft, hence increasing rate of resorption up to 32.9% as shown in a study by Hong Youl Kim et al. 6 Since the amount of fat to be grafted is limited by factors like donor site availability, number of sessions and volume, we utilised the Coleman principle of gentle extraction of fat, and placement of the fat in tiny aliquots to maximize revascularization by maximising area of contact. As recommended by Coleman and Saboeiro, 7 We also used a 10ml syringe with smaller calibre multihole canula for fat harvesting to reduce the negative impact of pressure as demonstrated by Hong Youl Kim et al. who used a 50 mL syringe with a 3 mm calibre cannula to result in high negative pressure and derive large fat parcels, which may have damaged the fat parcels and negatively influenced fat graft outcomes possibly contributing to their higher complication rates of 17.65%. Fat was placed into the pectoralis major muscle for volume and projection, and also into the more superficial tissues to control the shaping of the breast and to expand the envelope.
As far as oncological implication fat grafting has been successfully used in post lumpectomy patients. It has also been found that adipose derived mesenchymal stem cells (ASCs) have reduced and reversed radiation damage due to their regenerative properties. 8 Initially the angiogenetic and proliferating potential of ASCs was questioned in terms of safety for use in patients with history of breast cancer. But then it was found that ASCs behave differently when part of adipose tissue in situ as opposed to when isolated and culture expanded to a pure population, thus suggesting that clinical fat grafting does not induce breast cancer cell growth. 9 The main criticism of fat transfer in breast reconstructive surgery was the potential radiological obstruction. Several meta-analyses and systematic reviews have unanimously concluded that autologous fat transfer does not lead to an increased rate of locoregional breast cancer recurrence10,11 and in no way hindered accurate radiologic breast imaging, thus supporting it is oncologic safety.
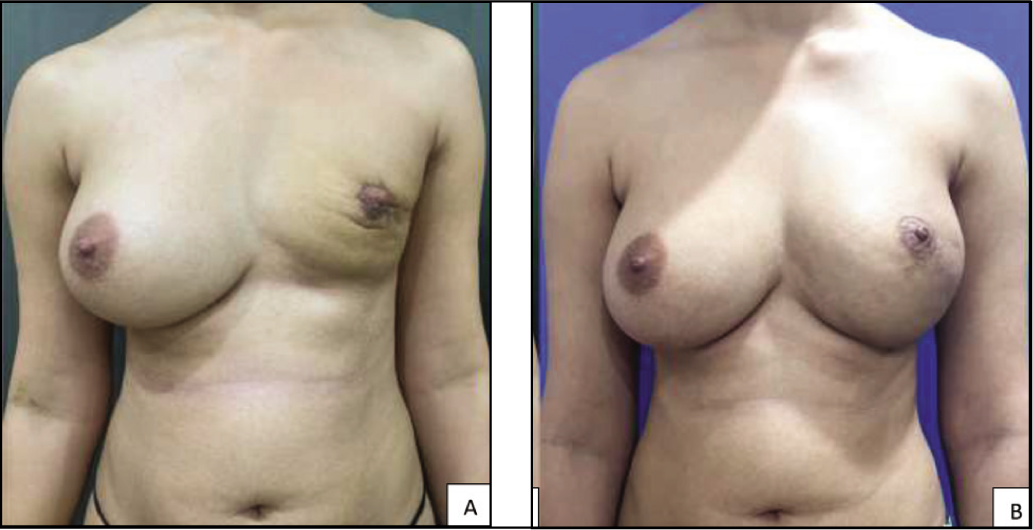
A & B – Final images showing expansion of the envelope, Volume Restoration, Scar Release and NAC Reconstruction of the Left Breast in Comparison to the Right Breast.
This technique of using only fat grafting for breast reconstruction post mastectomy is best suited for a small or medium sized breast to address volume, contour, scar and asymmetry but we have demonstrated that it can be safely utilised for larger volume reconstruction too. When constructing a breast mound with a small volume, a relative lack of upper quadrant fullness is not unexpected. For implant reconstruction, it is difficult to obtain a natural breast shape specially with a round implant. Benefits of fat grafting include creating a natural appearance and feel to the breasts without the added risks associated with implant-based breast augmentation such as the development of capsular contracture, possibility of implant rupture, or the need for implant exchanges. Flap reconstruction, though it achieves considerable volume to the breast and is a one-stage procedure, has few drawbacks. It does involve a significant donor site morbidity, prolonged operative time, is technically demanding and causes additional incision scars. The major limitation of fat grafting as a standalone procedure is the need for multiple sessions to achieve the desired proportions.
A & B – Images Showing Sideways Comparison Between the Normal and the Reconstructed Breast Showing Symmetrical Projection and Volume.

Some studies have also proposed that fat grafting prevents contracture and nerve entrapments, thereby improving the post mastectomy pain syndrome.12,13 Early fat grafting in irradiated breasts has shown to alleviate radiation induced fibrosis by progressive regeneration, including neo vessel formation and improved hydration. 13 Our first session of fat grafting was also done during the mastectomy where the goal was to lay the foundation for future sessions and possibly help in alleviating the post mastectomy pain.
Lipofilling following breast cancer treatment leads to a low complication rate of 8.2% 14 ; most of them are liponecrosis or oil cysts. There was some bruising witnessed after the second session and third session of fat grafting in this case, which resolved spontaneously in 2 weeks’ time.
Most studies have highlighted the use of fat grafting as an adjunct to breast implants and latissimus dorsi reconstructed breasts 15 but in our opinion, lipomodelling of the breast as a primary treatment can yield promising results and should be explored. Though there has been a study by Yanaga H. et al. 16 where cultured mature adipocytes and conditioned medium containing MCP-1 was used to reconstruct a unilateral breast post mastectomy, in our case report we have demonstrated that direct fat grafting alone can be used to correct post unilateral mastectomy defect to match the contralateral breast with equally satisfactory results. We do believe that some procedure done on the contralateral breast (breast lift or reduction) is likely to lessen the number of sessions of fat grafting required and help achieve better symmetry. Autologous fat grafting, besides being a safe procedure also offers other advantages like autologous reconstruction, cost effectiveness, reproducibility, natural consistency and appearance of breast, breast symmetry and treatment of fat deposits in the donor regions. Fat grafting can also be done as a day care procedure without adding significant morbidity, work hour loss or prolong hospital stay for the patient.
Conclusion
This case study suggests that fat grafting has been an underutilised tool and represents a promising intervention for the management of breast defects post mastectomy thereby improving the quality of life of these patients without any major or noticeable morbidity to any other body part. To provide definitive guidance to surgeons undertaking fat grafting for breast reconstruction deformities, larger prospective studies are required. We strongly believe that in well-selected cases, sequential fat grafting can be considered a standalone procedure to restore breast aesthetics. In others, it can also be used to build up tissue volume for future implant-based reconstruction if need be for better and quicker results.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Considerations
The study was approved by the institutional ethical committee and written informed consent was obtained from the patient for publication of this case report.
Funding
The authors received no financial support for the research, author-ship and/or publication of this article.