
Abstract
Introduction
The rising prevalence of obesity across all age groups in the U.S. poses increasing challenges to healthcare. Older adults with hip fractures are already medically vulnerable, and obesity compounds issues during preoperative optimization, intraoperative management, and postoperative planning. This study evaluates how obesity affects clinical and radiographic outcomes in older patients undergoing surgery for peritrochanteric hip fractures.
Methods
Patients aged 55+ treated for low-energy peritrochanteric hip fractures at our institution from January 2015 to May 2017 were identified. Patients were divided into non-obese (BMI <30) and obese (BMI ≥30) cohorts. A retrospective chart review was performed to assess outcomes.
Results
We identified 134 non-obese and 19 obese patients. Aside from BMI, there were no significant differences in age, gender, or Charlson Comorbidity Index. Obese patients had significantly longer operative times (P = .049) and a trend toward higher estimated blood loss (P = .057). They also experienced higher rates of deep vein thrombosis (P = .026) and any venous thromboembolism (P = .042). No significant differences were found in length of stay, transfusion needs, pulmonary embolism, mortality, discharge disposition, or 90-day readmission rates. Radiographically, there was no difference in average Tip Apex Distance (TAD) (P = .748) or proportion with TAD >25 mm (P = 1.000).
Conclusion
In older adults, obesity is associated with longer operative times, increased blood loss, and higher rates of thromboembolic events after surgical treatment of peritrochanteric fractures. These findings underscore the need for careful perioperative planning in obese patients, particularly regarding fluid management and thromboprophylaxis.
Introduction
The prevalence of obesity is increasing at a concerning rate. A study conducted by Harvard T.H. Chan School of Public Health in 2019 predicted that by 2030, nearly 50% of adults in the United States will be obese, with 25% classified as severely obese. 1 This alarming trend combined with a 26.2% increase among individuals aged 55 and older in the United States population from 2010 to 2020 have raised concerns about increased stress on the current healthcare system. 2
One known consequence of an aging population is the increased incidence of fragility hip fractures. These fractures are defined as fractures resulting from falls occurring at standing height or lower, with the most common locations being the thoracic spine, hip, and distal radius. These low-energy fractures are particularly worrisome due to their associated higher healthcare costs, greater disability, and increased mortality compared to other osteoporotic fractures. 3 Over 300 000 fragility fractures occur in the United States each year, 4 with an increased incidence in patients aged 50 and older and those with low bone mineral density.5,6 We can anticipate a more rapid escalation in the incidence of these fractures when we consider that obesity increases the risk of hip fragility fractures in post-menopausal women by an odds ratio of 22.05 compared to non-obese women. 7
Current management for intertrochanteric, basicervical, and subtrochanteric femur fractures includes surgical intervention with cephalomedullary nail (CMN) or sliding hip screw (SHS) constructs to allow early mobilization and avoid the morbidities and mortality risk associated with prolonged bedrest. 8
Outcomes following hip fracture treatment have been extensively reported; however, the literature examining perioperative and intraoperative outcomes for older obese patients with fragility hip fractures is limited. Prior studies have stated that obese hip fracture patients are at no greater risk for cardiac or non-cardiac post-operative complications,9,10 but demonstrated poorer functional outcomes after rehabilitation and higher reoperation rates.11,12 Furthermore, to our knowledge, no study has investigated the success of implant positioning in the obese hip fracture population, which is an integral factor in determining the success of operative intervention. 13
Thus, the objective of this study is to evaluate perioperative outcomes with a focus on implant positioning in older obese patients with peritrochanteric hip fractures. We hypothesized that the final implant positioning would not be affected by obesity status, though surgical times would be longer amongst obese patients. Additionally, we hypothesized that 30-day postoperative complication rates in obese patients with peritrochanteric hip fractures will be worse than in non-obese patients.
Materials and Methods
Study Design
For this institutional review board-approved study (#2017-7681), we identified all patients who sustained a low-energy hip fracture operatively treated at our institution between January 2015 and May 2017 utilizing the proprietary Clinical Looking Glass (CLG) research software. Inclusion criteria were all adult patients over the age of 55 who sustained low-energy peritrochanteric femur fractures during the above time frame, and who were treated with CMN or sliding hip screw fixation. Patients were excluded if they sustained a high-energy fracture or non-peritrochanteric fracture, were treated non-operatively, or had insufficient records. A retrospective chart review was performed to verify the above criteria prior to collecting demographic information, radiographic, intraoperative, and postoperative outcomes.
Patient Treatment Pathway
After presentation to the emergency room and diagnosis of a peritrochanteric fracture, patients were simultaneously evaluated by the orthopaedic and geriatrics teams. Once admitted to the co-managed geriatric orthopaedic service, patients were evaluated and optimized for surgery by fellowship-trained geriatrician physicians. Our institution has a standardized protocol for the evaluation and medical optimization of hip fracture patients with an emphasis on rapid evaluation and clearance for the operating room.
Once medically optimized, the patient was evaluated by the on-call anesthesia attending and taken to the operating room for fracture stabilization. Patient positioning and implant choice were left to the surgeon’s discretion and consisted of either a short or long CMN or a SHS construct.
Postoperatively, all patients were treated with a prophylactic dose of low molecular weight heparin (LMWH) in accordance with our institution’s standard protocol and in adherence to the clinical guidelines established by the American Society of Hematology in 2019. Additionally, if medically stable, patients initiated physical and occupational therapy on postoperative day one.
Data Analysis
The study was divided into two parallel analyses, clinical outcomes and radiographic outcomes. For the clinical outcomes, identified patients’ demographics were recorded, including age, weight, height, body mass index (BMI), and Charlson Comorbidity Index (CCI). The CCI is a widely used comorbidity index employed to evaluate survival rates in patients with multiple comorbidities. A higher score typically indicates an increased risk of mortality. Perioperative and postoperative outcomes were analyzed including operative time, estimated intraoperative blood loss, incidence of deep vein thrombosis (DVT) and pulmonary embolism (PE), postoperative disposition, time from admission to surgery, length of stay (LOS), and 90-day readmission rate. Operative time was delineated as the time from first incision until complete closure. Estimated blood loss was determined and agreed upon by the surgeon and anesthesiologist. The incidences of DVT and PE were determined through confirmatory ultrasound or Computed Tomography Angiography (CTA) when clinically indicated. For analysis of discharge disposition, data was only available on 133 non-obese and 18 obese patients, as one patient from each cohort expired before discharge.
For the radiographic analysis, radiographs demonstrating implant position were used as a surrogate for successful surgical intervention. The tip-apex distance (TAD) was used to measure the adequacy of lag screw fixation. Originally described by Baumgaertner et al. in the setting of determining the propensity for failure of sliding hip screw constructs,
13
the usage of TAD was adopted as a predictor of failure in CMN and SHS.14,15 In our study, the tip apex was measured using the technique modification described by Johnson et al.
16
This adaptation allows for the utilization of intraoperative fluoroscopic imaging, and the calibration of the measured values using a picture archiving and communication system (PACS).
16
Using the screening techniques mentioned above, 153 eligible patients were successfully identified. Of these, 6 did not have intraoperative fluoroscopic images saved in the system and an additional 30 patients had poor quality fluoroscopy images or insufficient radiographic views to measure TAD. These 36 patients were excluded from the radiographic analyses but were included in the clinical outcomes analyses (Figure 1). CONSORT Diagram of Patients With Peritrochanteric Hip Fractures
Statistical analysis was performed using both R (R Foundation for Statistical Computing, Vienna, Austria) and SPSS (IBM Corp, IBM SPSS Statistics. Armonk, NY) utilizing Fisher’s Exact test for categorical variables, and Welch’s unpaired t-test for continuous variables. The P-value for significance was set to .05.
Results
Patient Demographics
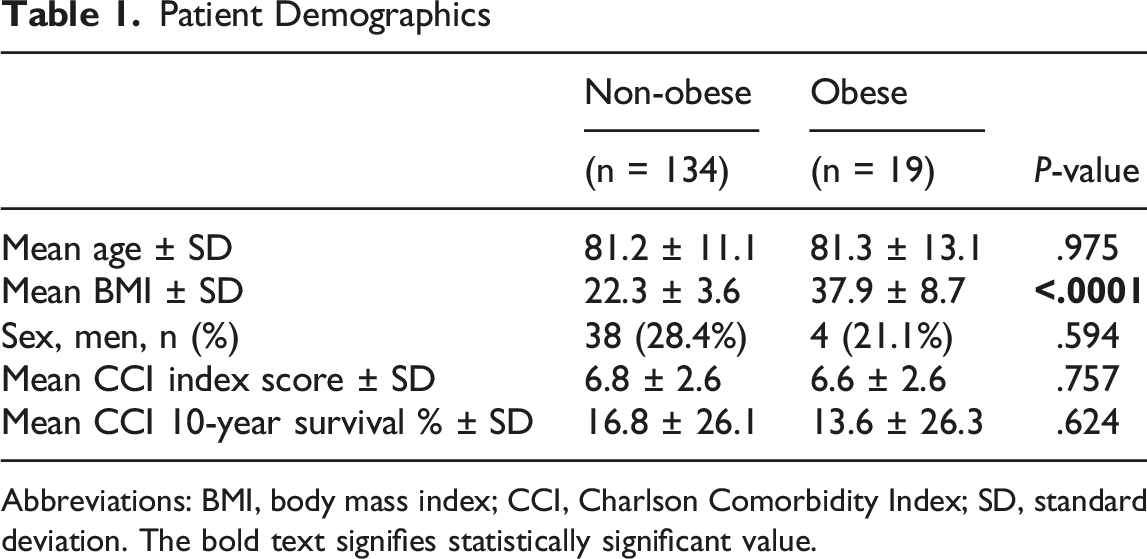
Abbreviations: BMI, body mass index; CCI, Charlson Comorbidity Index; SD, standard deviation. The bold text signifies statistically significant value.
Patient Comorbidities

Clinical Outcomes of Non-Obese vs Obese Patients Surgically Treated for Peritrochanteric Fractures

Abbreviations: DVT, deep vein thrombosis; OR, operative room; PE, pulmonary embolism; TAD, tip-apex distance; VTE, venous thromboembolism. The bold text signifies statistically significant value.
aAnalysis based on non-obese (n = 133) and obese (n = 18) to account for mortality among the cohorts before discharge.
bTAD calculations based on non-obese (n = 104) and obese (n = 13).
The radiographic analysis included 104 non-obese and 13 obese patients (36 patients were excluded due to the lack of quality imaging to support TAD measurements). The average TAD of the obese cohort (21.3 mm) and non-obese cohort (20.6 mm) was not significantly different (P = 0.748). The proportion of implants placed with a TAD greater than 25 mm was not different between the obese and non-obese (3/13 vs 30/104, P = 1.000) cohorts was also not statistically different (P = 1.000), suggesting that there were no outliers with regard to implant position (Table 3).
Discussion
Considering the rapid demographic shift towards an aging population and the concurrent surge in obesity, the demand for surgical treatment of peritrochanteric fractures within this population will continue to rise. Consequently, it is increasingly important for orthopaedic surgeons to possess familiarity with management considerations that are specifically relevant to this patient population. While previous studies have extensively documented the impact of obesity on VTE, wound complications, infection, and blood loss in patients undergoing total joint arthroplasty,17-23 there is limited research analyzing the incidence of perioperative complications associated with obesity in the context of fragility fractures.3,9,10,24,25 Furthermore, there is a scarcity of research that addresses the challenges faced by surgeons during surgical fixation of hip fractures in this cohort, which includes the increased radiation exposure experienced while operating on obese patients. 26
Regarding the radiographic outcomes of our study, we found no significant difference in TAD (P = .748) between the obese and non-obese cohorts. We selected the TAD as a proxy for appropriate implant positioning because the literature demonstrates it closely correlates with implant failure. 13 Although the center-center position could also be considered a proxy for appropriate implant placement, we felt that its analysis would be confounded by surgeon technical preferences. This is because there are some surgeons prefer a more interior and/or posterior screw or blade placement to engage the femoral calcar.
Although many surgeons perceive obese patients’ cases as more technically challenging and prone to implant malposition, the literature 27 and our study show no increased risk. We found no difference in TAD (P = 0.748) or in the proportion of implants with TAD greater than 25 mm (P = 1.000). However, even with optimal final implant positioning, obese patients had longer operative times than non-obese patients (94.2 vs 71.0 minutes, P = 0.049). This difference was not explained by variations in the use of long versus short CMN (57.9% vs 67.2%, P = .446) and is likely related, at least in part, to additional time required for adequate fluoroscopic imaging, establishing the start point, and closure.
Additionally, a trend towards higher estimated blood loss in the obese cohort (254 mL) compared to the non-obese cohort (123 mL), though it was not statistically significant (P = .057). This finding is likely attributable to the dissection of a larger soft tissue envelope. Given this, preoperative fluid resuscitation or blood transfusion should be considered on an individual basis to mitigate blood loss in this population. Maintaining proper volume status prior to surgery can help patients sustain effective circulating blood volume and blood pressure, potentially reducing intraoperative or postoperative complications, such as stroke and myocardial infarction, that are related to hypotension.
Furthermore, the incidence of VTE was significantly higher in the obese cohort. Obesity is a known independent risk factor for VTE, as it is considered a prothrombotic state due to multiple derangements in the normal hemostasis pathway. 28 While low molecular weight heparin (LMWH) is standardly used for VTE prophylaxis, dosing presents a unique challenge in obese patients, who have historically been underrepresented in studies assessing its efficacy at standard doses. 28 Although emerging evidence suggests that increasing the prophylactic dose of LMWH in obese patients is both safe and effective, this research remains limited. 29 Given the increased VTE risk in our obese cohort despite a standardized prophylactic protocol, clinicians should consider either increasing the LMWH dose or prescribing alternative anticoagulation agents for this patient population. We acknowledge that the exact dosage of TXA was not assessed in our study, but we still believe that these patients require increased measures of anticoagulation to mitigate their heightened VTE risk.
While our study found that older obese patients had longer operative times and a higher incidence of VTE, we must consider that these outcomes may not be solely attributable to BMI. Other confounding variables may have also played a role, such as malnutrition and socioeconomic disparity. Obesity can coexist with nutritional deficiencies, a condition sometimes referred to as “sarcopenic obesity,” where patients have excess fat mass but insufficient protein and micronutrients. 30 This can impair immune function and wound healing, potentially contributing to complications. Furthermore, while not seen in our study, socioeconomic disparities—which are often linked with higher rates of obesity31,32—have been associated with increased postoperative complications and longer hospital stays in other surgical populations.33,34
There are several limitations to this study. The retrospective nature of data collection introduces inherent limitations regarding completeness of the record, in this case availability of PACS imaging, and can therefore lead to unintentional bias. Additionally, the size of our obese cohort was limited, which may impact the generalizability of the study findings. Finally, limitation arises from potential treatment inconsistencies due to variations in the training and preferences of different operative surgeons, including their choice of positioning and implant. Larger, prospective studies are needed in order to understand these differences in outcomes as well as potential areas for intervention to reduce the discrepancy in outcomes between these two cohorts.
As the population in the United States continues to age, it is imperative that we understand the specific needs of the obese hip fracture population and make necessary changes to our protocol for the management of these individuals with specific attention to preoperative volume optimization and postoperative thromboembolic prophylaxis.
Conclusions
As the United States population continues to age, it is imperative that we begin to understand the unique challenges and needs of older, obese patients who sustain fragility hip fractures. While obese patients generally exhibited similar outcomes to their non-obese counterparts, there are important intraoperative differences to consider when caring for these patients. In anticipation of longer operative times and higher blood loss, preoperative volume optimization is critical for these patients to prevent hypotension-related complications intraoperatively. Postoperatively, obese hip fracture patients are at higher risk for VTE and alterations to the postoperative VTE prophylaxis protocol should be considered. We advocate for a continued multidisciplinary approach involving medical and anesthesia colleagues in order to address and potentially mitigate these differences to improve the outcomes of older patients with obesity who sustain low-energy hip fractures.
Footnotes
Ethical Considerations
Institutional review board (IRB) approval (#2017-7681) was obtained for this retrospective chart-review study.
Author Contributions
Simon Greenbaum: Conceptualization, Data curation, Writing - review & editing, Benjamin Levy: Conceptualization, Data curation, Methodology, Writing - review & editing, Abraham Goch: Conceptualization, Investigation, Methodology, Writing - review & editing, Danielle Putur: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing - original draft, Writing - review & editing, Andrea Munoz: Data curation, Formal analysis, Methodology, Writing - original draft, Writing - review & editing, Mani Kahn: Conceptualization, Investigation, Methodology, Supervision, Writing - original draft, Writing - review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
De-identified data are available from the corresponding author upon reasonable request and may require IRB approval.