
Abstract
Introduction:
Older patients with hip fractures require a long time to rehabilitate and recover after surgery. Although effective discharge instructions for long-term recovery are important, the discharge instructions of most acute-care hospitals are often presented as a brochure, which is difficult for older adults to follow. The purpose of this study was to develop rehabilitation instructions in the form of a mobile application for the physical recovery of older adults after hip fracture surgery.
Materials and Methods:
A mobile application for rehabilitation instructions after hip fracture surgery was developed in ADDIE order of analysis, design, development, implementation, and evaluation. The contents of the mobile application composed of rehabilitative exercises, activities of daily living, pain and nutrition management, fall prevention, and hospital visits. Nine experts evaluated the application and SPSS version 23.0 program was used for data analysis.
Results:
In the mobile application evaluation by the experts, the average score of the contents was 2.22 out of 3 points. The average score of understanding was the highest at 2.42, while accuracy was the lowest at 2.00 in the contents. The average score of the interface design was 2.32 out of 3 points. The average score of consistency was the highest at 2.42, while design suitability was the lowest at 2.25 in the interface design. The experts perceived the mobile application as simple and easy to understand while also suggesting some improvements.
Conclusion:
The average scores were highest for understanding of contents and consistency of the interface design and lowest for accuracy of contents and design suitability of the interface design. The mobile application was easy to understand and had consistency in design.
Introduction
The incidence of fragility fractures is increasing globally due to the progressive aging of the population. 1 Among fragility fractures, hip fractures often result in the most adverse consequences, including a higher rate of disability, higher healthcare costs, morbidity and mortality 2 and surgery has been reported as the standard treatment. 3 However, short hospital stay due to the burden of medical expenses 4 often lead to considerable burden on physical recovery for older adults and their families after discharge considering that rehabilitation is performed in the hospital where they received their operation depending on the healthcare providing system. 5
The discharge instructions from most acute-care hospitals are often presented as the form of brochure without any interaction with the patients. 6 Because older adults with hip fractures require a long time to rehabilitate and recover after surgery, 5 effective discharge instructions for long-term recovery are mandatory. Smartphones, with the advancement of mobile technology, can be used anytime and anywhere as a part of health-care education system 7 and the use of healthcare applications on it has increased exponentially. 8 Older people has been reported to show significant interest in how to access health-related information 9 and multimedia applications on smartphone devices 10,11 and iPads 12 was reported as effective tools for healthcare education in older adults. Moreover, a recent study 13 showed that understanding of how to use smartphones had significantly improved not only the life satisfaction, but self-esteem, and self-efficacy.
Although a recent report 14 showed the level of access to digital information to 91.7% for the elderly in their 60 s and to 79.4% for those in their 70 s or older, the level of digital literacy which represents the actual ability to use computers and mobile devices, fell sharply to 41.3% in older adults in their 60 s and to 16.2% in those in their 70 s or older. Several problems in smartphone use such as unfamiliarity with terms, small letters and screens, and the burden of cost have been reported to contribute to this low digital literacy levels, which implies the necessity for smartphone designed for easier use, with larger letters, and with less cost for older adults. Therefore, we developed rehabilitation instructions in the form of a mobile application for the physical recovery of older adults after hip fracture surgery, so that they could use it at home or in the community at any time after discharge. This study aimed to present preliminary data on the development and validation of a mobile application for older adults after hip fracture surgery.
Methods
We developed a mobile application in the analysis-design-development-implementation-evaluation (ADDIE) order 15 for rehabilitation instructions after hip fracture surgery.
Analysis
Previous studies were analyzed through academic search engines, including PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and Research Information Sharing Service (RISS), to identify the educational content of rehabilitation instructions after hip fracture surgery. The key words were hip fracture, surgery, management, rehabilitation, rehabilitative exercises, and discharge planning. We referred to the “Rehabilitation Treatment Guide for Hip-Fracture Surgery Patients” developed in a teaching hospital.
Design
All the authors took part in periodic meetings, and a literature review was conducted to develop the contents. The contents of the mobile application include rehabilitative exercises, activities of daily living (ADL), pain management, nutrition management, fall prevention, and hospital visits. The selection of rehabilitative exercises and ADL was evidence-based after the first and second authors reviewed the literature and discussed the exercises required after hip fracture surgery. The rehabilitative exercises are divided into bed, standing, and walking exercises, and we decided on a video format. The rehabilitative exercises also include goal setting in which older adults can set a count for bed and standing exercises and a duration for walking exercises for every day. For example, when they walk with their mobile phones in their pockets, the application is able to monitor the duration of the exercise. When the target time is reached, they can check the achievement of the goal. The ADL includes advice on how to use a bed and a toilet, correct posture, and postures to avoid while sitting in a chair, picking up things, taking a shower, cleaning, lying down, wearing pants, washing hair, and sitting in a car. We also decided to illustrate the actions of using a bed and a toilet using a video format, and correct postures and postures to avoid in the form of pictographs for easier understanding. The information on pain and nutrition management, fall prevention, and hospital visits was based on literature reviews and designed as static images and concise, large-sized characters.
Development
The main screen of the application was shown in Figure 1. We recorded videos of medical personnel doing rehabilitation exercises and ADL, and added a voice recording of the narration so that older adults can watch the videos and follow the actions. In rehabilitation exercises, bed exercises include lifting the leg, lifting the hip, lifting the leg to the side, and lifting the leg in a sitting position (Figure 2). Standing exercises include raising the leg forward, extending the leg backward, and pulling the leg sideways while in a standing position. Each exercise was recorded as a video with 5 repetitions. Walking exercises include a video of walking using a walker. This application was designed so that older adults set their rehabilitative exercise goals by clicking on an item and to check whether the daily goals were achieved in a rehabilitation journal.

Main screen.
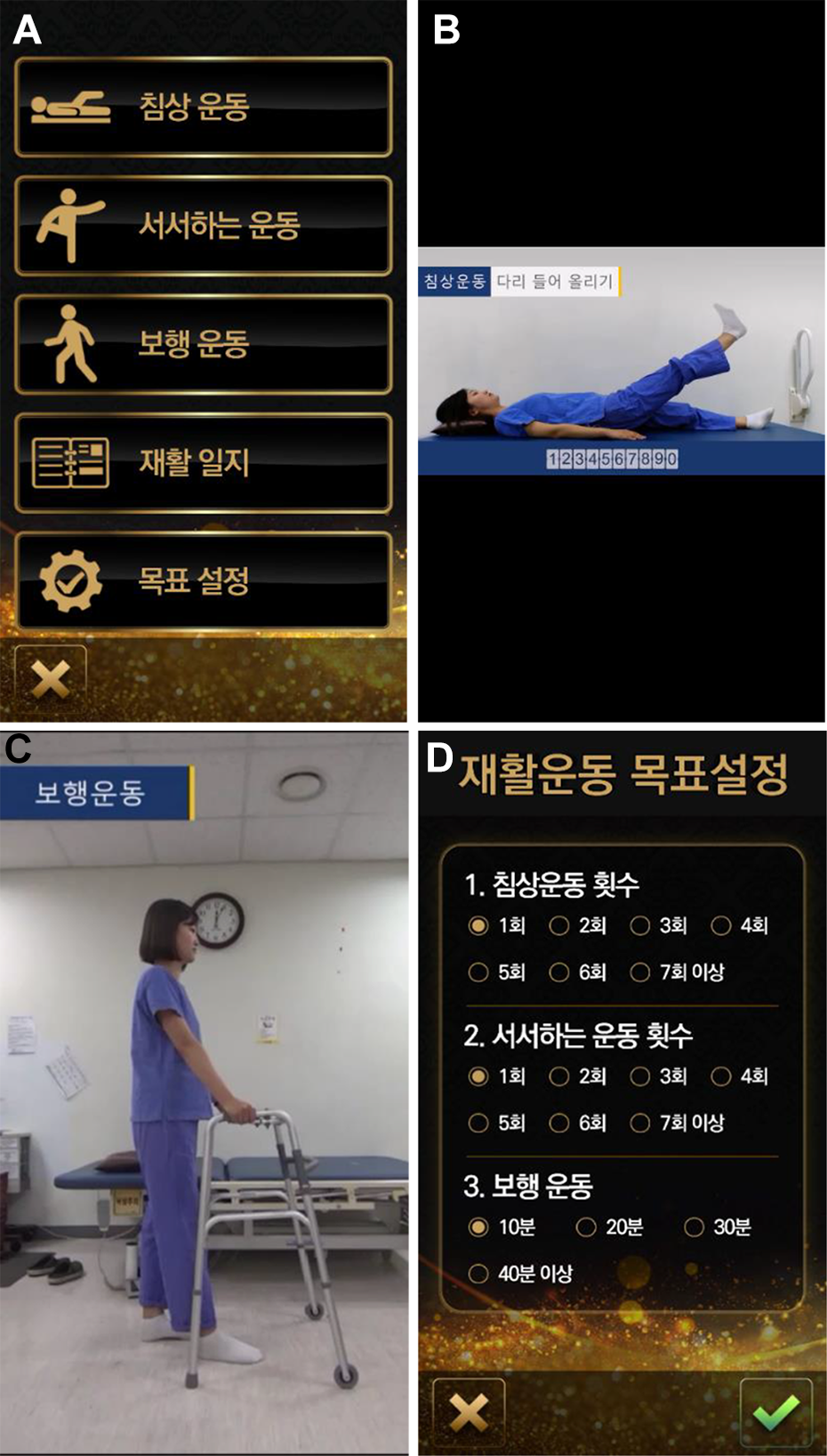
Rehabilitative exercises screen.
The actions of ADL were also recorded as a video of medical personnel demonstrating how to use a bed and a toilet. The video of using a bed demonstrates going to bed and moving from a wheelchair onto the bed. The video of using the toilet includes moving from the wheelchair onto the toilet seat and vice versa. Each correct posture and postures to avoid are represented in the form of pictographs (Figure 3). The contents of pain and nutrition management, fall prevention, and hospital visits are simple, with large, widely spaced characters (5 mm) (Figure 4). When pointing at the triangular button indicating “next” at the bottom right of the screen, the next screen opens with a sound feedback.

ADL screen.

Pain and nutrition management, fall prevention, and hospital visit screen.
The mobile application was developed based on the Android programming environment and we created a storyboard that determined how the screen should be structured with the help of professional application developers. We took into consideration visibility, such as color, font shape, and large-sized characters, and usability, such as minimal cost for Internet use. The name of the organization that developed this mobile application was indicated. The mobile application was developed with the name “rehabilitation instructions after hip fracture surgery,” in Korean from June to August 2018. This application can be downloaded free from Google Play Store.
Implementation and Evaluation
Nine experts, including a clinical instructor in orthopedic surgery, 3 orthopedic surgeons, 2 head nurses, and 3 orthopedic ward nurses with more than 5 years’ experience downloaded the application onto their mobile phones and used it for one week. Next, they evaluated the application using a healthcare smartphone application evaluation tool developed by Jin 16 which was approved by the original author via email. The validated healthcare smartphone application evaluation tool consists of 3 categories including contents of 9 items, interface designs of 11 items, and skills of 3 items. The 3 categories are divided into 7 sub-factors: accuracy of 2 items, understanding of 3 items, objectivity of 4 items for content, consistency of 3 items, design suitability of 5 items, vocabulary accuracy of 3 items for interface design, and security of 3 items for skill. The tool consists of a total of 23 questions with a four-point Likert scale, with a higher score indicating a higher quality. The mobile application developed in this study did not require personal information and security associated with skill. Accordingly, the healthcare smartphone application evaluation tool was modified by deleting a skill category that consisted of 3 questions.
Data Analysis
All data were analyzed using SPSS version 23.0. (SPSS, Inc., Chicago, IL, USA). The 2 categories and 6 sub-factors of the health-care smartphone application evaluation tool are indicated with means and standard deviations.
Results
The mobile application evaluation of the experts was shown in Table 1. In the healthcare smartphone application evaluation, the average score of the contents was 2.22 out of 3 points. The average score of understanding was the highest at 2.42, while accuracy was the lowest at 2.00. The average score of the interface design was 2.32 out of 3 points. The average score of consistency was the highest at 2.42, while design suitability was the lowest at 2.25.
Experts’ Evaluation of the Mobile Application for Rehabilitation Instructions After Hip Fracture Surgery.

Here are some of the experts’ comments and feedback: 1) The application is concise and simple, 2) The video of rehabilitation exercises is easy and helpful for older adults to follow, 3) A function to replay the rehabilitation exercise video is needed, 4) It is necessary to reorganize the exercises by dividing bed exercises into lying and sitting exercises, 5) Goal setting can be difficult for older adults. It is necessary to maximize the font size for goal setting, 6) Some of the video quality needs to be improved, 7) The background color of the application is suitable, but the yellow text is not easy to read.
Discussion
This study adopted the ADDIE model to develop the mobile application-based rehabilitation instructions for older adults after hip fracture surgery. While rehabilitative education after hip fracture surgery is important for older adults, it is often provided in the form of a brochure without an explanation during the short hospital stay 17,18 and is difficult for low-literate, older adults to read and follow once they are discharged. 18 Thus, effective implements to educate older adults are needed to develop 12 and mobile applications gain popularity to provide health-care education. 8 Since most older adults in many countries 14 are possessing mobile devices, rehabilitative instructions in the form of a mobile application might be effective for physical recovery if some of the problems that older adults may experience when using mobile phones are resolved.
Through literature reviews and experts meetings, the content of the mobile application was developed to include rehabilitative exercises, ADL, pain management, nutrition management, fall prevention, and hospital visits. The content was similar to a previous study 12 that included exercises specific to hip fracture surgery, precautions when moving such as how to transfer safely onto and off a bed or a chair. Notably, rehabilitative exercises and ADL were developed in a multimedia format, allowing older adults to watch and follow instructions sequentially. The multimedia format of rehabilitative exercises and ADL was also found in another study 17 that developed a health-education Compact Disc (CD) regarding pre- and post-operative care, pain control, rehabilitative exercise, methods for safely rising from a bed, and the use of walking aids for patients with total knee replacement. It is likely to contribute to a high score for easy-to-understand healthcare contents in the mobile application evaluation conducted by the experts of this study. Multimedia-based materials can be viewed repeatedly, cost-effectively, and are suitable for patients with a low level of education. 17 Goal setting and watching its achievement as a strategy for improving confidence in rehabilitative exercises in this study can be useful to manage self-care effectively. 19
As evaluated by experts, the healthcare contents are more accessible and may connect ADL effectively through this mobile application’s pictographs. The pictographs are explained as simple line drawings of full-body figures with no distracting background to state actions as “DOs” and “DON’Ts”. 18 Visual materials are suitable to low-literacy older adults for easier learning. 18,20 Choi 21 found that 15 low-literate older adults who participated in a focus group after hip replacement surgery perceived that pictograph-based instructions were helpful in understanding the step-by-step procedures of discharge actions.
Information on pain, fall prevention, and hospital visits, including potential complications, were included briefly in this application with text and static images as they have been reported as the most important learning needs of patients after hip fracture surgery. 22 Although this information was similar to the booklet by Lin et al 23 educating postoperative issues and home self-care with copious pictures for hip fracture patients, it was difficult to compare this study with previous studies because of few relevant studies on the development of mobile applications for those with hip fracture surgery. Malnutrition has been reported to increase mortality rates 24 and thus, nutrition management is important in the rehabilitation of frail older adults after osteoporotic hip fracture. 25 However, nutrition management was addressed in some mobile applications for patient with colorectal cancer 26 or kidney transplantation, 27 but not for those with hip fracture surgery. Thus, we believe that our study to develop the mobile application and validate it might be meaningful to improve rehabilitation in older adults after hip fracture surgery.
Meanwhile, the score was lowest for the accuracy of the contents. We speculated that this low accuracy might originate from the person responsible for the accuracy and verification of the data was not indicated in the mobile application. A study 28 found that the criteria for evaluating accuracy of health information on the Internet included the source notation, responsibility, and verification as well as the accuracy of the contents. For the reliability and clarity of healthcare information, it is necessary to specify not only the organizations that developed this mobile application but also information providers and data verification.
The interface design of the mobile application consists of consistency, design suitability, and vocabulary accuracy. Consistency scored the highest, while design suitability scored the lowest. Consistency has been reported the most important when evaluating a design, and includes the unified arrangement of the contents, use of a single color in the graphics, and grouping. 16 Meanwhile, the visual components in the design suitability scored the lowest at 1.88 and was comparable to the results of post-operative self-care application evaluation for those after kidney transplantation. 27 The visual components in the design suitability were connected with a comment from experts that the yellow letters on a black background were difficult to read despite the significant difference in color and brightness. 29 A study found that bright letters on a dark background facilitated readability for older adults. 30 Further validation is necessary with the end users to maximize their relevance. 18 Additionally, some comments from experts, including a function to replay the rehabilitation exercise video, subdividing bed exercises, the font size of the goal settings, and video quality, indicate areas for improvement.
Our study was limited because the mobile application was evaluated by experts in a teaching hospital, but not by end-users including patients themselves and further evaluation by end-users are needed to validate its clinical value.
Conclusion
Our findings showed that the average score was highest for understanding of contents and consistency of the interface design and lowest for accuracy of contents and design suitability of the interface design. The mobile application was easy to understand and had consistency in design. It might be helpful for older adults to manage their rehabilitation status after hip fracture surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT, and Future Planning (NRF-2017R1C1B5075973).